Mastering Below-Knee Amputation: An Intraoperative Masterclass for Complex Lower Extremity Tumors
Key Takeaway
This masterclass details below-knee amputation for extensive lower extremity tumors. We cover comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution, emphasizing precise neurovascular management, optimal flap creation, and robust myodesis. Learn critical pearls, pitfalls, and post-operative rehabilitation strategies to achieve functional outcomes and prevent complications.
Introduction and Epidemiology
Extensive tumors of the distal leg, ankle, and foot frequently necessitate a below-knee amputation, clinically referred to as a transtibial amputation, as the primary modality of surgical extirpation. Historically, the evolution of musculoskeletal oncology has heavily favored limb salvage; however, the distal lower extremity presents unique anatomical and biomechanical constraints. The paucity of expendable soft tissue coverage and the dense proximity of vital neurovascular structures in the foot and ankle dictate that attempts at marginal limb salvage often yield a functionally inferior, insensate, or chronically painful extremity.
Conversely, modern advances in prosthetic design, socket engineering, and dynamic response components allow transtibial amputees to achieve exceptionally high-level functional outcomes. In many complex oncologic and orthopedic scenarios, a well-executed below-knee amputation provides superior biomechanical function, a significantly lower complication profile, and a more rapid return to ambulation compared to complex limb-sparing procedures necessitating free tissue transfer and extensive skeletal reconstruction.
Epidemiologically, primary bone sarcomas of the foot are rare entities, comprising approximately 1% of all osteosarcomas and Ewing sarcomas. Soft tissue sarcomas, such as synovial sarcoma, clear cell sarcoma, and epithelioid sarcoma, exhibit a higher predilection for the distal extremity. For high-grade sarcomas, particularly those involving the plantar aspect of the foot, and low-grade lesions with extensive compartmental infiltration or neurovascular encasement, transtibial amputation remains the definitive oncologic gold standard.
Surgical Anatomy and Biomechanics
Osteology and Compartmental Anatomy
The structural foundation of a durable transtibial amputation relies on the meticulous management of the tibia and fibula. The tibial diaphysis is distinctly triangular in cross-section, necessitating a careful and precise beveling of the anterior crest to prevent soft tissue ulceration at the anterior distal aspect of the residual limb. The fibula must be transected 1 to 2 centimeters proximal to the tibial cut. This proximal resection creates a conical residual limb, preventing lateral socket impingement and mitigating the risk of fibular abduction during the swing phase of gait.
The leg is divided into four distinct fascial compartments: anterior, lateral, superficial posterior, and deep posterior. The standard long posterior flap technique, popularized by Burgess, relies almost exclusively on the superficial posterior compartment (gastrocnemius and soleus complex) to provide robust, well-vascularized soft tissue padding over the distal bone ends. The robust vascular supply to the medial and lateral heads of the gastrocnemius via the sural arteries ensures flap viability even in cases of moderate peripheral arterial disease.

Neurovascular Topography
The principal anatomic focus during a below-knee amputation is the systematic identification, ligation, and management of the crural neurovascular bundles. Failure to meticulously manage these structures inevitably leads to catastrophic hemorrhage or debilitating neuroma formation.
The anterior tibial artery, accompanied by its venae comitantes and the deep peroneal nerve, courses deep to the anterior tibialis muscle and lateral to the tibial crest, resting on the interosseous membrane. These structures must be isolated and individually ligated. The deep peroneal nerve requires traction neurectomy—applying distal tension, ligating to prevent bleeding from the vasa nervorum, and sharply transecting—to allow it to retract deep into the proximal muscular bed, safely away from the distal weight-bearing surface.
Posteriorly, the anatomy becomes more complex. The posterior tibial artery, vein, and tibial nerve are situated posterior to the tibia and tibialis posterior muscle, but anterior to the soleus within the deep posterior compartment. The peroneal artery and veins course posterior and lateral to the tibia, residing in the interval between the tibialis posterior and the flexor hallucis longus.
The superficial peroneal nerve, located within the lateral compartment, typically pierces the crural fascia approximately 10 to 12 centimeters proximal to the lateral malleolus. Failure to identify and sharply transect this nerve under tension frequently results in a highly symptomatic neuroma at the anterolateral aspect of the prosthetic socket brim. Additionally, the saphenous nerve medially and the sural nerve posteriorly must be identified and managed with similar traction neurectomy techniques.
Biomechanics of the Transtibial Amputee
Preservation of the knee joint drastically alters the metabolic demands of ambulation compared to a transfemoral amputation. Classic orthopedic literature dictates that a unilateral transtibial amputee requires only a 10% to 20% increase in energy expenditure above baseline normal ambulation. In stark contrast, a transfemoral amputee requires a 60% to 70% increase. The preservation of the quadriceps mechanism and native knee kinematics allows for efficient forward propulsion, proprioception, and shock absorption. This underscores the critical importance of preserving tibial length whenever oncologically and vascularly feasible, as the length of the tibial lever arm directly correlates with the mechanical advantage required to control the prosthesis.
Indications and Contraindications
The decision to proceed with a transtibial amputation must carefully balance oncologic clearance, vascular viability, and the anticipated functional outcome of the patient. While this text focuses primarily on oncologic indications, the surgical principles apply broadly across a spectrum of orthopedic pathologies, including severe trauma, chronic osteomyelitis, and end-stage peripheral vascular disease.

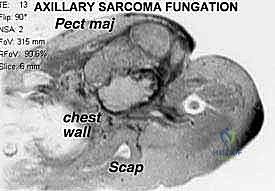
Primary oncologic indications include tumor recurrence in the distal tibia, ankle, and foot that is not amenable to limb salvage techniques. Infiltrative high-grade soft tissue sarcomas or extensive bone sarcomas that encase or compromise the major neurovascular bundles of the distal leg preclude functional salvage. Furthermore, amputation is indicated for palliation in cases of fungating, painful tumors, or following failed attempts at radiation therapy for dorsal and plantar foot tumors resulting in chronic ulceration, intractable pain, and osteoradionecrosis.

Operative Indications Versus Limb Salvage
| Clinical Scenario | Indication for Transtibial Amputation | Indication for Limb Salvage |
|---|---|---|
| High Grade Foot Sarcoma | Plantar aspect involvement, extensive multi-compartmental invasion | Dorsal aspect, easily resectable with wide negative margins |
| Neurovascular Involvement | Encasement of posterior tibial and dorsalis pedis arteries | Displacement without encasement, reconstructable vessels |
| Recurrent Disease | Local recurrence post-radiation with a stiff, insensate foot | First-time occurrence with highly favorable anatomic location |
| Metastatic Disease | Palliative control of a fungating, painful, or bleeding lesion | Systemic control achieved, isolated resectable metastasis |
| Trauma and Infection | Unreconstructable mangled extremity (MESS > 7), chronic osteomyelitis | Adequate bone stock and robust soft tissue for free flap coverage |

Pre Operative Planning and Patient Positioning
Advanced Imaging Modalities
Meticulous preoperative planning is paramount to ensure negative oncologic margins while simultaneously maximizing residual limb length. The surgical plan must be entirely dictated by the proximal extent of the pathology.
Although plain radiographs lack the sensitivity to delineate soft tissue tumor margins, they are requisite for the initial evaluation of osseous integrity, identifying primary bone sarcomas, evaluating periosteal reactions, or detecting cortical destruction from adjacent soft tissue lesions.
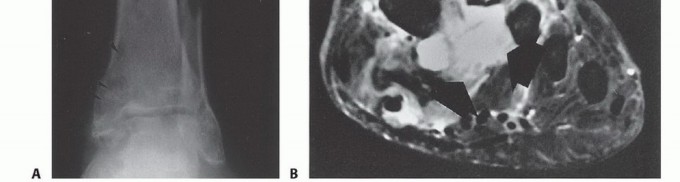
Computed tomography (CT) and magnetic resonance imaging (MRI) are the absolute cornerstones of preoperative staging. MRI meticulously determines the proximal extent of intramedullary tumor involvement and maps the extraosseous soft tissue extension. T1-weighted coronal and sagittal sequences are critical for evaluating marrow replacement and identifying skip lesions, while T2-weighted fat-suppressed axial images delineate the precise relationship of the tumor mass to the tibial and peroneal neurovascular bundles.
Bone scanning utilizing Technetium-99m or Positron Emission Tomography (PET) is mandatory if the primary tumor is located at or proximal to the ankle joint. Standard oncologic principles dictate that the level of bone transection should be 4 to 7 centimeters proximal to the most proximal abnormal uptake on the bone scan or MRI, ensuring a wide oncologic margin.
Angiography or CT Angiography is highly valuable, particularly in older patients, diabetics, or those with prior radiation therapy. It determines the patency of the anterior and posterior tibial arteries. Tumor involvement or vascular occlusion of these vessels dictates flap design; a compromised posterior tibial artery may preclude the use of a standard long posterior flap, necessitating alternative approaches such as sagittal flaps, skew flaps, or a higher level of amputation (e.g., through-knee or transfemoral).
Biopsy Confirmation Principles
A definitive histologic diagnosis via core needle or incisional biopsy is an absolute prerequisite prior to proceeding with an amputation. The biopsy tract must be meticulously planned by the operating surgeon. It should be longitudinal and placed directly in line with the planned surgical incisions for the amputation, ensuring that the entire biopsy tract is excised en bloc with the surgical specimen to prevent iatrogenic tumor seeding of the residual limb.
Patient Positioning and Preparation
The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to correct natural external rotation, bringing the patella to face directly anteriorly. A pneumatic tourniquet is applied to the proximal thigh. Tourniquet use is standard for oncologic resections to minimize blood loss and provide a bloodless field for neurovascular identification. However, it must be used with extreme caution or avoided entirely in patients with severe peripheral vascular disease to prevent ischemic complications to the surgical flaps.

Detailed Surgical Approach and Technique
Flap Design and Incision Marking
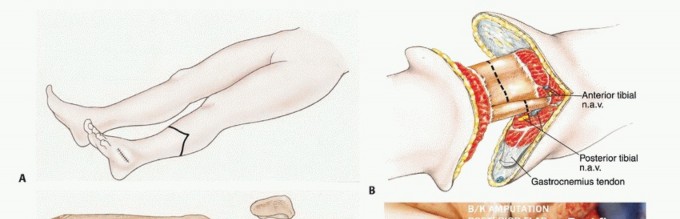
The ideal level of surgical resection for a standard transtibial amputation is at the musculocutaneous junction of the gastrocnemius muscle. This provides optimal soft tissue padding and a reliable blood supply for the posterior flap. The ideal tibial length is generally 12 to 15 centimeters from the medial joint line, though this is ultimately dictated by oncologic margins.
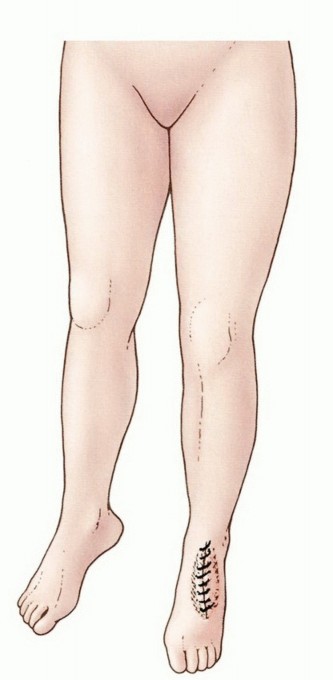
The anterior incision is marked transversely across the anterior half of the leg at the predetermined level of tibial transection. The posterior flap is designed to be longer than the anterior flap, typically measuring one-third to one-half the circumference of the calf at the level of the anterior incision. The medial and lateral limbs of the incision drop distally from the edges of the anterior incision, curving posteriorly to form a broad, U-shaped posterior flap.
Anterior Dissection and Neurovascular Isolation
The anterior incision is carried sharply through the skin, subcutaneous tissue, and crural fascia. The anterior compartment musculature (tibialis anterior, extensor hallucis longus, extensor digitorum longus) is transected at the level of the skin incision.
Deep to the anterior tibialis, the anterior tibial neurovascular bundle is identified. The anterior tibial artery and venae comitantes are doubly ligated with non-absorbable suture and transected. The deep peroneal nerve is grasped, pulled distally under tension, ligated, and sharply transected, allowing it to retract deep into the proximal muscle belly to prevent neuroma formation at the distal stump. The lateral compartment musculature (peroneus longus and brevis) is similarly transected, and the superficial peroneal nerve is identified and managed with traction neurectomy.
Osteotomy and Bone Management
The periosteum of the tibia is incised circumferentially. A retractor is placed posterior to the tibia to protect the deep posterior compartment. The tibia is transected using an oscillating saw. A critical step is the creation of an anterior bevel. A 45-degree oblique cut is made on the anterior tibial crest, starting 1.5 centimeters proximal to the transverse cut. The edges of the tibia are then meticulously smoothed with a rasp to remove any sharp prominences that could cause delayed skin breakdown.

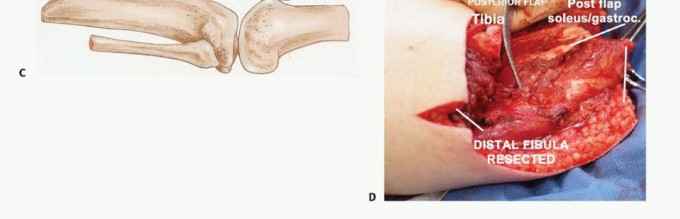
Attention is turned to the fibula. The fibula must be cut 1 to 2 centimeters proximal to the tibial osteotomy. The surrounding musculature is elevated, and a narrow oscillating saw is used to transect the bone. The lateral aspect of the fibula is rasped smooth. Care must be taken to avoid excessive subperiosteal stripping of the fibula, which can lead to devascularization, subsequent ring sequestrum formation, and chronic osteomyelitis.

Posterior Dissection and Flap Elevation
With the bones transected, a bone hook is placed in the distal tibial segment to apply anterior traction. The deep posterior compartment musculature is transected. The posterior tibial neurovascular bundle and the peroneal neurovascular bundle are identified.

The posterior tibial artery and peroneal artery are meticulously isolated, doubly ligated, and divided. The tibial nerve is isolated, pulled distally, ligated to prevent bleeding from the vasa nervorum, and sharply transected high in the wound.
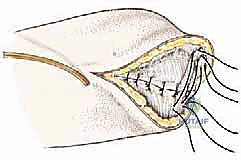
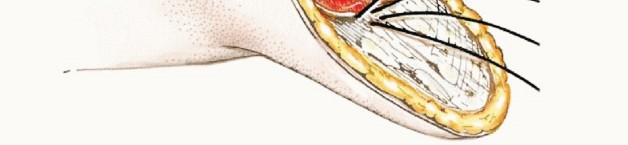
The amputation is completed by beveling the posterior flap. The gastrocnemius and soleus muscles are divided from deep to superficial, angling the scalpel distally to taper the muscle mass. This ensures the myofascial flap will fold smoothly over the distal tibia without excessive dog-ears, redundant tissue, or problematic bulk that complicates socket fitting.
Myodesis and Wound Closure
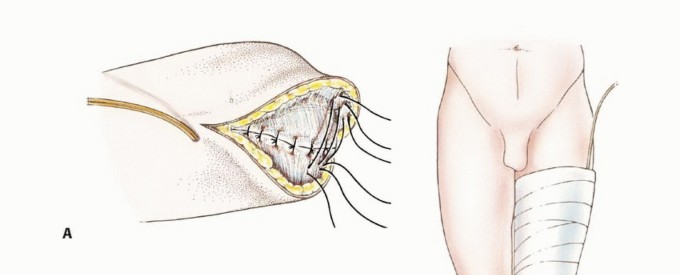
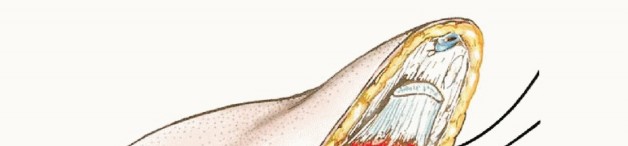
To optimize prosthetic control, prevent distal bone prominence, and maintain the physiological tension of the musculature, a myodesis is performed. The deep fascia of the posterior flap (gastrocnemius-soleus complex) is brought anteriorly and sutured directly to the anterior tibial periosteum and the deep fascia of the anterior compartment. This is achieved through pre-drilled osseous tunnels in the anterior tibia or via robust periosteal sutures.

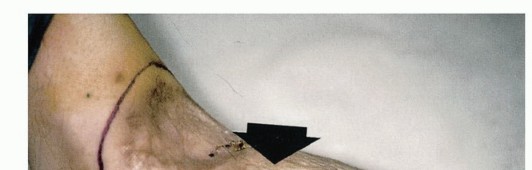
A closed suction drain is placed deep to the muscle layer to prevent hematoma formation, which is a primary catalyst for infection and wound dehiscence. The subcutaneous tissue is closed with interrupted absorbable sutures, and the skin is approximated with non-absorbable sutures or staples, ensuring a tension-free closure. The resulting surgical scar should lie anteriorly, proximal to the distal weight-bearing surface of the residual limb.
Complications and Management
Despite meticulous surgical technique, transtibial amputations carry a distinct complication profile, particularly in the oncologic population where neoadjuvant or adjuvant therapies (chemotherapy, radiation) may severely compromise wound healing.
Knee Flexion Contracture
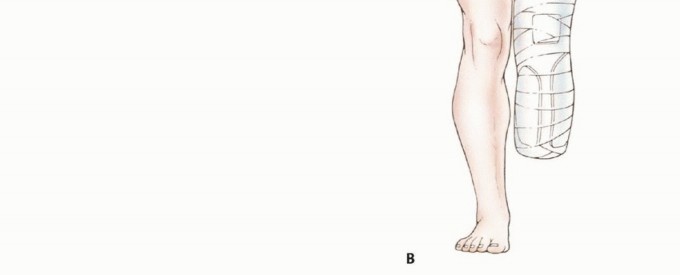
The most significant functional complication is a knee flexion contracture. Because the gastrocnemius crosses the knee joint, postoperative pain and positioning often lead patients to rest with the knee in a flexed position. A contracture greater than 15 degrees severely compromises prosthetic fitting, alters the center of gravity, and dramatically increases the energy expenditure of ambulation. Prevention via immediate postoperative rigid dressings (IPRD) or knee immobilizers is paramount.
Neuroma Formation
Symptomatic neuromas occur when a transected nerve adheres to the distal scar or bone, subjecting it to mechanical irritation from the prosthetic socket. The superficial peroneal, deep peroneal, tibial, and sural nerves are the most common culprits. Management begins with socket modification and pharmacotherapy (gabapentinoids). Refractory cases require surgical excision of the neuroma. Modern surgical management heavily favors Targeted Muscle Reinnervation (TMR) or deeper proximal burying of the nerve stump into vascularized muscle bellies.
Summary of Complications
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategies |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 10% - 15% | Ischemia, excessive wound tension, prior radiation therapy, malnutrition | Local wound care, negative pressure wound therapy, revision amputation to a higher level |
| Knee Flexion Contracture | 20% - 30% | Poor postoperative positioning, lack of early rehabilitation, prolonged pain | Aggressive physical therapy, serial casting, dynamic splinting, posterior capsule release (rare) |
| Symptomatic Neuroma | 5% - 10% | Inadequate proximal nerve retraction during index surgery, superficial neuroma tethering | Socket relief, gabapentinoids, surgical excision with Targeted Muscle Reinnervation (TMR) |
| Phantom Limb Pain | 60% - 80% | Cortical reorganization, central sensitization, preoperative pain severity | Multimodal analgesia, mirror box therapy, neuromodulation, TMR |
| Bone Prominence / Bursitis | 5% - 10% | Inadequate tibial beveling, fibula left too long, severe muscle atrophy | Prosthetic modification, surgical revision with bony contouring and soft tissue advancement |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation of the transtibial amputee is a multiphasic process requiring coordinated multidisciplinary care involving orthopedic surgeons, physiatrists, prosthetists, and physical therapists.
Acute Postoperative Phase (Days 1 to 14)
The immediate clinical goals are edema control, meticulous wound healing, and contracture prevention. In the operating room, a rigid removable dressing (RRD) or an immediate postoperative prosthesis (IPOP) is frequently applied. The RRD protects the residual limb from trauma, controls edema, and rigidly maintains the knee in full extension. The patient is mobilized on postoperative day one with physical therapy, focusing on contralateral limb strengthening, core stability, and upper extremity conditioning for walker or crutch use.
Pre Prosthetic Phase (Weeks 2 to 6)
Following suture removal (typically at 2 to 3 weeks, though frequently delayed in oncologic patients receiving systemic chemotherapy), the focus shifts to aggressive residual limb shaping. Shrinker socks are utilized to promote a conical shape and reduce interstitial edema. Desensitization techniques, including tapping, massage, and variable texture stimulation of the distal limb, are initiated to prepare the skin for socket contact. Range of motion exercises for the hip and knee are intensified to ensure full extension is maintained.
Prosthetic Phase (Weeks 6 and Beyond)
Once the residual limb volume has stabilized and the surgical wound is fully consolidated, the patient is casted for a preparatory (temporary) prosthesis. This phase involves intensive gait training, focusing on weight shifting, balance, and symmetrical stride length. The alignment of the socket must accommodate any minor flexion contractures while promoting a smooth transition from heel strike to toe-off. As the limb continues to atrophy and mature over the first 6 to 12 months, frequent socket modifications and ply-sock additions are required before a definitive prosthesis is fabricated.
Summary of Key Literature and Guidelines
The surgical and functional principles of transtibial amputation are deeply grounded in classic orthopedic literature and modern oncologic guidelines.
The metabolic demands of amputation levels were definitively quantified by Waters et al., demonstrating the exponential increase in energy expenditure as amputation levels move proximally. This seminal work remains the primary academic justification for preserving the knee joint in oncologic resections whenever clear margins can be obtained.
The design of the long posterior flap, popularized by Burgess, remains the workhorse technique globally. Burgess demonstrated that utilizing the well-vascularized gastrocnemius muscle provides superior healing rates and a more durable weight-bearing surface compared to equal anterior-posterior flaps or fish-mouth incisions, particularly in dysvascular patients.
In the realm of musculoskeletal oncology, guidelines from the Musculoskeletal Tumor Society (MSTS) and the National Comprehensive Cancer Network (NCCN) dictate that while limb salvage is preferred, amputation remains strongly indicated when negative margins cannot be achieved without sacrificing the major neurovascular bundles of the foot and ankle. Modern outcome studies confirm that for distal extremity sarcomas, patients undergoing transtibial amputation often report higher functional scores (e.g., Toronto Extremity Salvage Score) and fewer reoperations compared to those undergoing complex distal limb salvage with compromised biomechanics.
You Might Also Like