PIP Joint Fracture-Dislocation ORIF: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on Proximal Interphalangeal (PIP) joint fracture-dislocation open reduction and internal fixation (ORIF). We'll meticulously cover surgical anatomy, preoperative planning, precise intraoperative steps, instrument selection, fixation techniques, and critical pearls to ensure optimal outcomes for these challenging finger injuries. Learn to restore stability and function for complex articular fractures.
Alright, team, let's gather around. Today, we're tackling a challenging, yet critically important, injury: a Proximal Interphalangeal (PIP) joint fracture-dislocation. These are not just "jammed fingers," fellows; they're complex intra-articular injuries with significant soft tissue involvement, and if not managed meticulously, they can lead to devastating long-term stiffness, pain, and functional loss. Our goal here is not just reduction, but stable, anatomic fixation that allows for early motion and preserves long-term joint function.
Understanding the PIP Joint: Essential Surgical Anatomy
Before we make any incision, let's re-familiarize ourselves with the intricate anatomy of the PIP joint. This is a hinge joint, a true ginglymus, formed by the radial and ulnar condyles of the proximal phalanx articulating with matching concavities on the base of the middle phalanx. This bony congruence is our primary stabilizer, allowing for a remarkable 120 degrees of flexion and extension, which accounts for approximately 85% of the motion required for effective grasp. However, it offers very limited abduction and adduction.
Soft Tissue Restraints: The stability of this joint is also heavily reliant on its robust soft tissue envelope.
* Volar Plate: This is a strong, fibrocartilaginous structure on the palmar aspect of the joint. It's taut in extension and acts as a critical restraint against dorsal hyperextension and dorsal subluxation. In dorsal fracture-dislocations, it often avulses distally from the middle phalanx base, frequently taking a significant articular fragment with it.
* Checkrein Ligaments: These are slender, proximal extensions of the volar plate. They anchor the volar plate to the proximal phalanx, restricting hyperextension. Critically, branches of the digital arteries and nerves pass beneath these ligaments, supplying the joint and the flexor tendon vincula. We must be exquisitely careful here to protect these vital neurovascular structures.
* Collateral Ligaments: These are the primary soft tissue stabilizers against abduction and adduction stresses.
* Proper Collateral Ligaments (Radial and Ulnar): These originate from the sides of the proximal phalanx head and insert onto the middle phalanx. They are taut in flexion and provide the main resistance to varus and valgus stress. The radial collateral ligament is injured far more frequently than the ulnar collateral, almost six times as often, particularly in dorsal dislocations.
* Accessory Collateral Ligaments: These arise volarly to the proper collateral ligaments and insert onto the volar plate. They are taut in extension.
* Extensor Complex: On the dorsal aspect, the extensor mechanism limits volar directed stress.
* Central Slip: This is the direct continuation of the extensor digitorum communis tendon, inserting onto the dorsal tubercle at the base of the middle phalanx. It's the primary extensor of the PIP joint.
* Conjoint Lateral Bands: These run obliquely on each side of the joint, contributing to both PIP extension and DIP extension.
* Transverse Retinacular Ligament: This connects the central slip and the conjoint lateral bands, extending laterally.
For a dislocation to occur, fellows, at least one, often two, and sometimes all three of these major stabilizing structures—the volar plate, collateral ligaments, and extensor complex—must be significantly disrupted.

FIG 1 • A detailed diagram illustrating the complex anatomical structures of the PIP joint, including the volar plate, checkrein ligaments, proper and accessory collateral ligaments, and the extensor complex.
Pathogenesis and Classification: Understanding the Injury
The PIP joint is uniquely susceptible to injury due to its exposed position and high functional demands. The pattern of injury is dictated by the direction, degree, and rate of force application. We classify these into three main groups based on mechanism and deformity:
Dorsal Subluxation or Dislocation (Most Common)
This typically results from hyperextension and axial loading. The middle phalanx is forced dorsally on the proximal phalanx, often resulting in a fracture involving the volar base of the middle phalanx. The size of this volar lip fragment is crucial for stability.
* Stable: Less than 30% of the articular surface involved. Reduces in extension.
* Tenuous: 30% to 50% of the articular surface involved. Reduction maintained with less than 30 degrees of flexion.
* Unstable: Greater than 50% articular surface involvement, or 30% to 50% but requiring more than 30 degrees of flexion to maintain reduction. This is our territory for operative intervention.
Volar Subluxation or Dislocation
Less common, caused by forced flexion of an extended joint.
* Stable: Joint reduction in extension.
* Unstable: Palmar subluxation of the middle phalanx with the joint extended. Often involves an avulsion of the central slip.
Pilon Injuries
Caused by an axial force on a partially flexed PIP joint, leading to comminution of the articular surface of the middle phalanx (commonly, volar and dorsal articular fragments surrounding a central depressed fragment). These are almost always unstable and require operative fixation. Unicondylar fractures of the proximal phalanx head, while a variant, are also often unstable and amenable to similar approaches.
History and Physical Findings: The Diagnostic Workup
Patients typically present after a traumatic event, though sometimes it's delayed, initially dismissed as a "jammed finger."
* Acute Presentation: Primary complaints are pain and swelling.
* Subacute/Chronic Presentation: Patients focus on stiffness, loss of function, and persistent swelling, with pain being secondary.
Key elements of our examination:
1. Mechanism of Injury: Crucial for understanding the forces involved.
2. Inspection: Look for swelling, deformity (extension deformity for volar dislocations, flexion deformity for dorsal dislocations), and any open wounds. Axial or rotational malalignment may indicate articular depression of a condyle, subtly seen as angulation during full extension.
3. Palpation: Pinpoint tenderness helps identify injured soft tissue structures.
4. Neurovascular Exam: Always assess capillary refill and sensation (paresthesias) both pre- and post-reduction.
5. Range of Motion (ROM): Note the active and passive ROM, and importantly, the range through which the joint remains reduced.
6. Elson Test: To assess central slip integrity. With the PIP joint flexed 90 degrees over a table edge, ask the patient to actively extend the PIP against resistance.
* Intact Central Slip: You'll feel extension force at the PIP, and the DIP joint remains flail.
* Complete Central Slip Rupture: Absence of PIP extension force, with fixed extension at the DIP joint (due to lateral bands acting alone). This test can be painful, so a digital block may be necessary.
Imaging and Diagnostic Studies
Our radiographic evaluation is paramount.
* Standard Views: Posteroanterior (PA), true lateral, and partially supinated and pronated oblique radiographs of the involved digit.
* Oblique Views: Essential for identifying fracture planes and comminution, which directly impacts our surgical planning.
* True Lateral Film: CRITICAL. This must be in full PIP joint extension to accurately determine the amount of articular involvement and assess stability. Radiographs can be misleading, showing a small fragment that is actually the major attachment of a ligament or volar plate, indicating gross instability.
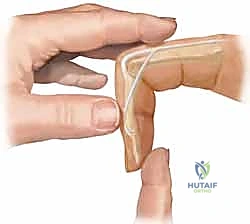

FIG 4 • A. Lateral radiograph of an unstable dorsal PIP fracture-dislocation, revealing significant volar articular surface involvement (over 50%). Such extensive involvement indicates a high degree of instability.
- V Sign: On a post-reduction true lateral radiograph, divergence of the dorsal articular surfaces from the central portion of the joint creates a V-shaped gap. This indicates an incompletely reduced joint.
- Dynamic Fluoroscopy: Extremely valuable. It allows us to dynamically assess reduction and, crucially, its stability through a range of motion. We can determine the exact joint position where instability or redislocation occurs, which guides our decision-making for conservative management (e.g., extension block splinting) or operative intervention.
- Hinged Flexion: A variant of the V-sign where congruent rotation is replaced by abnormal translation across flattened fracture segments during active flexion/extension.

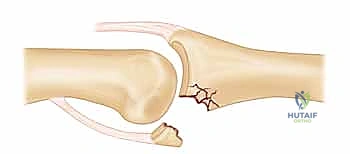
FIG 4 • B. The V-sign on a lateral radiograph indicating an incompletely reduced dorsal fracture-dislocation, characterized by a V-shaped gap created by the divergence of the dorsal articular surfaces.
Nonoperative Management: When is it an Option?
While many PIP fracture-dislocations are disabling, a significant number can be treated nonoperatively with closed reduction, splinting, and early motion.
* Closed Reduction Technique:
* Dorsal Dislocations: Gentle traction on the finger with the wrist neutral. Then, press the base of the middle phalanx volarly while stabilizing the proximal phalanx.
* Volar Dislocations (without rotation): Gentle traction with the wrist neutral, applying a dorsally directed force to the middle phalanx and a volarly directed force to the proximal phalanx.
* Volar Dislocations (with rotation): These are often difficult to reduce closed due to entrapment of the proximal phalanx head between the central slip and a lateral band. Try placing the MCP and PIP joints in 90 degrees of flexion with the wrist extended, applying light traction, and rotating the middle phalanx opposite to the deformity.
Surgical Warning:
Always perform a careful neurologic examination before administering an anesthetic block. Ensure adequate anesthesia prior to any manipulation. Be gentle, and limit reduction attempts. Irreducible dislocations are usually due to soft tissue interposition (volar plate, collateral ligament, flexor or extensor tendon).
Surgical Management: Indications and Goals
Surgical management of PIP fracture-dislocations is technically demanding due to small, comminuted fragments and the critical need for rigid fixation to allow early motion.
Indications for Open Reduction and Internal Fixation (ORIF):
- Unstable and tenuous fractures: Requiring more than 30 degrees of flexion to maintain reduction.
- Irreducible fractures: By closed methods, where fragments are amenable to internal fixation.
- Significant articular depression, displacement, or incongruity.
- Volar dislocations with a rotatory component that are irreducible by closed means.
- Unicondylar fractures of the proximal phalanx head with instability or displacement.
Goals of Surgical Treatment:
- Stable, anatomic fixation: Achieving a concentric reduction of the PIP joint.
- Early range of motion: Crucial to enhance cartilage and soft tissue healing, promote joint remodeling, and minimize adhesions and contractures.
- Anatomic restoration of the congruous joint surface: While desirable, this is a secondary goal and does not supersede a concentric PIP reduction and the ability for early motion.
Surgical Warning:
These fractures carry a high risk of redisplacement. Patients must be thoroughly counseled about the possibility of repeat surgical treatment. The definitive method of fixation is often dictated by intraoperative findings.
Preoperative Planning: Setting the Stage for Success
Our preoperative planning is meticulous.
1. Radiographic Evaluation: Review all PA, true lateral, and oblique views. Mentally reconstruct the fracture pattern.
2. Templating: Although not always formal for small fragments, consider the size and location of the fracture. For larger fragments, plan potential screw trajectories and K-wire placements.
3. Fluoroscopy Setup: Essential. We'll need a C-arm positioned to allow for immediate, high-quality PA and true lateral views of the digit without repositioning the hand. This will guide our reduction and fixation.
Patient Positioning and Anesthesia
Let's get our patient positioned.
* Position: The patient is supine on the operating table.
* Hand Table: A radiolucent hand table is essential, allowing for unrestricted fluoroscopy.
* Tourniquet: A brachial tourniquet is placed on the upper arm. We'll inflate it to 250 mm Hg just before the incision to ensure a bloodless field, which is critical for visualizing small fragments and delicate neurovascular structures.
* Anesthesia: While a wrist or digital block can be used, an axillary block is preferred. This provides superior sensory anesthesia and, critically, motor relaxation of both flexors and extensors, which greatly aids in reduction and prevents muscle spasm during our delicate manipulations.
Surgical Approaches: Gaining Access
The choice of surgical approach is dictated by the fracture pattern, fragment location, and the direction of dislocation. We have three main options:
1. Volar (Bruner) Approach
This is the workhorse for volar lip fractures of the middle phalanx base and dorsal dislocations. It provides excellent access to the volar plate and the fracture fragment.
Intraoperative Execution: Volar Approach
-
Incision: Identify the neurovascular bundles, fellows. We'll make a Bruner zigzag incision on the volar aspect of the digit. Start just proximal to the PIP joint crease, zig-zag across the joint, and extend distally. This design avoids scar contracture across the flexion crease.

FIG 5 • The Bruner zigzag incision, a common volar approach, carefully designed to avoid flexion contractures across the PIP joint crease.
-
Skin Flap Elevation: Carefully elevate the skin flaps. Remember, the digital neurovascular bundles run along the sides of the digit, immediately volar to the collateral ligaments. Use fine dissecting scissors or a scalpel to meticulously elevate the flaps, staying superficial to the underlying flexor tendon sheath.
-
Flexor Sheath Incision: Once the skin flaps are elevated, you'll see the flexor tendon sheath. We'll make a longitudinal incision in the flexor tendon sheath, typically between A2 and A4 pulleys, or directly over the fracture site. Avoid damaging the critical A2 and A4 pulleys, as this can lead to bowstringing of the flexor tendons.
-
Neurovascular Bundle Protection: Retract the flexor tendons to expose the volar plate. Identify and protect the neurovascular bundles, which lie on either side of the flexor sheath, deep to the skin and superficial to the collateral ligaments. Use small vessel loops or fine retractors to gently protect them.
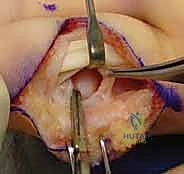
FIG 6 • Dissection through the flexor tendon sheath to expose the volar plate, ensuring careful protection of the digital neurovascular bundles.
-
Volar Plate Elevation/Arthrotomy: The volar plate is often avulsed with the fracture fragment. If it's intact, we'll perform a transverse or longitudinal incision in the volar plate to gain access to the joint. If the fragment is large, the volar plate is often attached to it. Carefully elevate the volar plate and its attached fragment from the proximal phalanx head, hinging it distally. This provides excellent exposure of the articular surface of the proximal phalanx and the middle phalanx base.

FIG 7 • Elevation of the volar plate and its attached fracture fragment, providing clear visualization of the articular surfaces for reduction.
- Fracture Reduction: With the joint exposed, we can directly visualize the fracture. Gently manipulate the middle phalanx to reduce the dislocation. Use a small dental pick or a Freer elevator to reduce the articular fracture fragment back into its anatomic position on the middle phalanx base. Ensure perfect articular congruence.
Fixation Techniques (Volar Approach)
A. K-wire Fixation:
* Indications: Small, single fragments, or for temporary stabilization.
* Technique:
* Once the fragment is anatomically reduced, hold it securely with fine forceps.
* Drill under direct visualization and fluoroscopic guidance. Insert one or two 0.028-inch or 0.035-inch K-wires obliquely across the fracture fragment into the main body of the middle phalanx. Ensure the K-wires are entirely intraosseous and do not penetrate the articular surface or impede joint motion.
* Pearl: Start the K-wire just distal to the fracture line, angling proximally into the middle phalanx. This gives better purchase.
* Check stability and range of motion. If stable, cut the K-wires flush with the bone or bend them and bury them sub-dermally.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">

FIG 8 • Fracture reduction and initial K-wire fixation of the volar fragment, ensuring precise alignment.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">

FIG 9 • Additional K-wire fixation to further stabilize the reduced volar articular fragment.
B. Mini-Fragment Screw Fixation:
* Indications: Larger, single, non-comminuted volar lip fragments (typically >2mm thickness) that allow for adequate screw purchase. Provides more rigid fixation than K-wires.
* Technique:
* Reduce the fragment anatomically. Hold it firmly.
* Using a 1.0mm or 1.3mm drill bit, pre-drill a glide hole in the fragment and a threaded hole in the middle phalanx shaft.
* Measure the screw length.
* Insert a 1.0mm or 1.3mm cortical screw (headless compression screws are excellent here) to achieve interfragmentary compression.
* Pearl: Ensure the screw head is countersunk to avoid soft tissue irritation. Avoid overtightening, which can strip the bone.
* Check stability and range of motion.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">

FIG 10 • Application of a mini-fragment screw for rigid internal fixation of the volar articular fragment.
C. Cerclage Wire Fixation:
* Indications: Small, comminuted fragments where screw purchase is difficult, or as an adjunct to K-wires.
* Technique:
* Reduce the fragment.
* Drill two small holes (e.g., 0.028 K-wire size) through the main middle phalanx bone, just proximal to the fracture.
* Pass a 24-gauge cerclage wire through these holes and around the fracture fragment, securing it in place.
* Twist the wire ends tightly, cut, and bury the twist.
2. Dorsal (Chamay) Approach
Used for dorsal pilon fractures or central slip avulsions.
Intraoperative Execution: Dorsal Approach
-
Incision: A dorsal midline longitudinal incision, or a curved incision, centered over the PIP joint. This provides direct access to the extensor mechanism.

FIG 11 • A dorsal midline longitudinal incision, typically used for dorsal approaches to the PIP joint.
-
Skin Flap Elevation: Elevate skin flaps carefully.
-
Extensor Mechanism Dissection: Incise the extensor mechanism longitudinally, either splitting the central slip or making a U-shaped flap with its apex pointing proximally. If splitting the central slip, retract the lateral bands gently to expose the joint. If creating a flap, ensure adequate length for repair.
- Pitfall: Be extremely cautious not to damage the lateral bands or the central slip's insertion.

FIG 12 • Dissection of the extensor mechanism, retracting the lateral bands to expose the dorsal aspect of the PIP joint.
- Fracture Reduction: Visualize the fracture fragments. Reduce them anatomically using picks or elevators.
Fixation Techniques (Dorsal Approach)
-
K-wire Fixation: For small dorsal fragments or for dorsal block pinning.
- Dorsal Block Pinning: For unstable dorsal dislocations without significant comminution, where the joint is stable in some flexion.
- Reduce the PIP joint.
- Flex the joint to the angle where it is stable (e.g., 20-30 degrees).
- Insert a 0.035-inch K-wire from the dorsal aspect of the middle phalanx, across the PIP joint, and into the proximal phalanx. The K-wire should act as a dorsal block, preventing hyperextension and redislocation, but allowing full flexion.
- Check fluoroscopically in both PA and lateral views. The wire should be dorsal to the center of rotation.

- Dorsal Block Pinning: For unstable dorsal dislocations without significant comminution, where the joint is stable in some flexion.
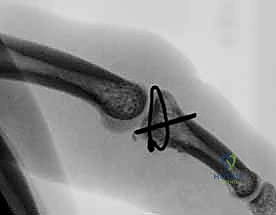
FIG 13 • K-wire fixation across the PIP joint for dorsal block pinning, preventing hyperextension while allowing flexion.
- Mini-Fragment Screws: For larger dorsal fragments or unicondylar fractures. Similar technique to volar screw fixation.
3. Mid-Axial Approach
This approach is less common for fracture-dislocations but can be used for specific unicondylar fractures or when collateral ligament repair/reconstruction is needed. It provides direct access to the collateral ligaments and side of the joint.
Intraoperative Execution: Mid-Axial Approach
- Incision: A longitudinal incision along the mid-axial line of the digit, avoiding the neurovascular bundle which is just volar to this line.
- Dissection: Carefully incise the skin and subcutaneous tissue. Identify and retract the neurovascular bundle volarly.
- Joint Exposure: Incise the accessory collateral ligament and joint capsule to expose the joint.
Salvage Procedures: When Primary ORIF is Insufficient
Sometimes, due to significant bone loss or comminution, a stable reduction is unobtainable with standard ORIF. In these cases, we have salvage options:
1. Volar Plate Arthroplasty
This technique is indicated for dorsal fracture-dislocations with significant (e.g., >50%) articular surface involvement or extensive comminution of the middle phalanx base. It restores the volar buttress and resurfaces the damaged articular surface.
Intraoperative Execution: Volar Plate Arthroplasty
- **
Additional Intraoperative Imaging & Surgical Steps







REFERENCES
-
Agee JM. Unstable fracture dislocations of the proximal interphalangeal joint. Treatment with the force couple splint. Clin Orthop Relat Res 1987;214:101–112.
-
Blazar PE, Steinberg DR. Fractures of the proximal interphalangeal joint. J Am Acad Orthop Surg 2000;8:383–390.
-
Bruner JM. Surgical exposure of the flexor tendons in the hand. Ann R Coll Surg Engl 1973;53:84–94.
-
Chamay A. A distally based dorsal and triangular tendinous flap for direct access to proximal interphalangeal joint. Ann Chir Main 1988;7:179–183.
-
Deitch MA, Kiefhaber TR, Stern PJ. Dorsal fracture dislocations of the proximal interphalangeal joint: surgical complications and longterm results. J Hand Surg Am 1999;24:914–923.
-
Eaton RG, Malerich MM. Volar plate arthroplasty for the proximal interphalangeal joint: A review of ten years’ experience. J Hand Surg Am 1980;5:260–268.
-
Elson RA. Rupture of the central slip of the extensor hood of the finger. A test for early diagnosis. J Bone Joint Surg Br 1986;68B:229–231.
-
Freeland AE, Benoist LA. Open reduction and internal fixation method for fractures at the proximal interphalangeal joint. Hand Clin 1994;10:239–250.
-
Glickel SZ, Barron OA. Proximal interphalangeal joint fracture dislocations. Hand Clinics 2000;16:333–344.
-
Green A, Akelman E, et al. Acute open reduction and rigid internal fixation of proximal interphalangeal joint fracture dislocation. J Hand Surg Am 1992;17:512–517.
-
Hamilton SC, Stern PJ, Fassler PR, et al. Mini-screw fixation of proximal interphalangeal joint dorsal fracture-dislocations. J Hand Surg Am 2006;31:1349–1354.

You Might Also Like


