Pelvic External Fixation: Principles, Techniques, and Clinical Protocols
Key Takeaway
Anterior pelvic external fixation is a critical intervention in damage control orthopedics, providing rapid pelvic ring stability and hemorrhage control. This guide details the biomechanics, indications, and step-by-step surgical techniques for both iliac crest and supraacetabular pin placement. It also covers the management of vertically unstable fractures, frame construction, and the transition to definitive internal fixation, ensuring optimal outcomes in polytraumatized patients.
INTRODUCTION TO PELVIC RING INJURIES AND DAMAGE CONTROL
High-energy pelvic ring disruptions present a formidable challenge to the orthopedic traumatologist, often accompanied by life-threatening hemorrhage and profound hemodynamic instability. In the acute phase of resuscitation, the application of an anterior pelvic external fixator is a highly versatile and life-saving intervention. Rooted in the principles of Damage Control Orthopedics (DCO), external fixation provides rapid, temporary pelvic stability, reduces pelvic volume to promote venous tamponade, and allows unhindered access to the abdomen and perineum for concurrent general surgical or urological procedures.
While primarily utilized as a provisional stabilization tool in the polytraumatized patient, pelvic external fixation can also serve as definitive fixation in highly selected fracture patterns (e.g., specific Anteroposterior Compression [APC] type II injuries) or as a critical adjunct to internal fixation. Mastery of the osseous corridors, biomechanical principles, and fluoroscopic anatomy is mandatory for safe and effective application.
INDICATIONS AND CONTRAINDICATIONS
Indications for Pelvic External Fixation
The decision to apply a pelvic external fixator is dictated by the patient's hemodynamic status and the specific mechanical instability of the pelvic ring. Primary indications include:
* Hemodynamic Instability: Acute management of "open book" (APC-II and APC-III) pelvic fractures in hypotensive patients, acting to close the symphyseal diastasis and reduce retroperitoneal volume.
* Provisional Stabilization: Temporary fixation of rotationally unstable pelvic fractures to facilitate nursing care, patient mobilization, and pain control while awaiting definitive internal fixation.
* Adjunctive Fixation: Used in combination with posterior pelvic ring internal fixation (e.g., sacroiliac screws) to neutralize anterior ring forces.
* Definitive Fixation: In select cases of purely rotationally unstable injuries (APC-II) where internal fixation is contraindicated due to severe soft tissue compromise (e.g., Morel-Lavallée lesions) or systemic patient factors.
Contraindications
Not all pelvic fractures are amenable to external fixation. Careful assessment of preoperative radiographs and computed tomography (CT) is essential to identify contraindications:
* Iliac Wing Fractures: Fractures propagating through the iliac wing compromise the osseous corridors required for pin purchase, leading to inadequate fixation and a high risk of pin cutout.
* Acetabular Fractures: Pin placement in the presence of an acetabular fracture risks intra-articular penetration, propagation of the fracture lines, or obstruction of future surgical approaches to the acetabulum.
* Severe Ilium Comminution: Lack of intact cortical bone negates the biomechanical stability of the Schanz pins.
Clinical Pearl: Always evaluate the soft tissue envelope. While external fixation avoids the extensive dissection of internal fixation, placing pins through grossly contaminated wounds or areas of established necrosis should be avoided to prevent deep pin-tract infections.
BIOMECHANICS OF PELVIC EXTERNAL FIXATION
The primary biomechanical goal of anterior pelvic external fixation is to counteract the deforming forces acting on the disrupted pelvic ring. In APC injuries, the external rotation of the hemipelvis is driven by the pull of the gluteus maximus and the external rotators of the hip.
By placing pins into the robust osseous corridors of the ilium and connecting them with an anterior frame, the surgeon creates a "tie-rod" effect. This construct effectively closes the anterior symphyseal diastasis, internally rotates the hemipelves, and tension-bands the posterior pelvic ligaments (if partially intact). The resulting reduction in pelvic volume is critical for increasing retroperitoneal pressure, which facilitates the tamponade of bleeding from the presacral venous plexus and cancellous bone surfaces.
SURGICAL ANATOMY AND OSSEOUS CORRIDORS
Successful pin placement relies on a profound understanding of the complex, three-dimensional anatomy of the innominate bone. There are two primary corridors utilized for pelvic external fixation: the Iliac Crest and the Supraacetabular corridor.
The Iliac Crest Corridor
The iliac crest provides a relatively superficial and accessible corridor. The optimal bone stock is located in the anterior third of the iliac crest, specifically within the gluteus medius pillar (the osseous condensation extending from the anterior superior iliac spine [ASIS] toward the sciatic notch). The corridor is narrow, bounded by the inner and outer cortical tables of the ilium.
The Supraacetabular Corridor
The supraacetabular corridor is biomechanically superior to the iliac crest. The starting point is the anterior inferior iliac spine (AIIS), and the corridor extends posteriorly and superiorly toward the posterior superior iliac spine (PSIS), passing directly above the acetabular dome and the greater sciatic notch. This dense cylinder of bone offers exceptional pin purchase and allows for the use of larger diameter pins.
OPERATIVE TECHNIQUE: ILIAC CREST PIN PLACEMENT
Iliac crest pin placement is often favored in emergency department settings or when rapid application is required without extensive fluoroscopy, though fluoroscopic confirmation remains the standard of care.
Step-by-Step Procedure
- Positioning: The patient is positioned supine on a radiolucent trauma table. The entire abdomen, pelvis, and bilateral thighs are prepped and draped to allow for frame assembly and potential conversion to laparotomy.
- Incision: A 2 to 3 cm incision is made directly over the anterior third of the iliac crest, beginning approximately 2 cm posterior to the ASIS.
- Dissection: Blunt dissection is carried down through the subcutaneous tissue to the fascia. The fascia is incised, and the periosteum is elevated slightly to expose the bony crest.
- Pin Insertion: Ideally, two 5.0-mm Schanz pins are placed between the inner and outer iliac cortical tables. A drill guide must be used to protect the soft tissues. The pins are directed posteriorly and slightly inferiorly, aiming toward the thickest portion of the gluteus pillar.
- Emergency Department Variation: When a fixator is applied to a severely injured, hemodynamically unstable patient directly in the emergency department, the standard two-pin construct may be insufficient due to suboptimal conditions. In these critical scenarios, we recommend using three pins in each iliac wing to ensure accurate pin placement, maximize purchase, and prevent catastrophic frame failure during resuscitation.
- Fluoroscopic Confirmation: Placement must be confirmed on fluoroscopy. Obturator oblique and iliac oblique (Judet) views are utilized to ensure the pins are contained entirely within the medullary canal of the ilium and have not breached the inner or outer tables.
Surgical Warning: Penetration of the inner table risks injury to the iliacus muscle, retroperitoneal hematoma, or bowel injury. Penetration of the outer table compromises fixation strength and risks injury to the gluteal musculature.
OPERATIVE TECHNIQUE: SUPRAACETABULAR PIN PLACEMENT
Supraacetabular pin placement is the preferred technique for definitive or long-term temporary external fixation due to its superior biomechanical stability. However, it requires strict fluoroscopic guidance and a thorough understanding of pelvic anatomy.
Advantages and Disadvantages
- Advantages: Excellent, dense cortical pin purchase; biomechanically robust; pins are located lower on the torso, providing better clearance for abdominal surgery and ostomies.
- Disadvantages: Requires precise fluoroscopy; risk of intra-articular penetration; limited hip flexion in some patients due to pin impingement on the anterior thigh musculature; risk of injury to the Lateral Femoral Cutaneous Nerve (LFCN).
Step-by-Step Procedure
- Fluoroscopic Setup: Ensure the C-arm can freely obtain AP, Inlet, Outlet, Obturator Oblique, and Iliac Oblique views of the pelvis.
- Incision: A 1.5 to 2 cm longitudinal incision is made approximately 2 cm distal and 2 cm lateral to the ASIS.
- Dissection: Blunt dissection is performed using a hemostat to spread the tissues down to the AIIS. The dissection must carefully navigate between the sartorius and the tensor fasciae latae (TFL).
- Protecting the LFCN: The Lateral Femoral Cutaneous Nerve is highly variable but generally courses medial to the ASIS and over the sartorius. Meticulous blunt dissection and the use of tissue protection sleeves are mandatory to prevent iatrogenic nerve injury.
- Starting Point: A sharp trocar or drill is placed directly on the AIIS.
- Trajectory and Drilling: The trajectory is aimed toward the PSIS. Under fluoroscopic guidance:
- Obturator Oblique View: Confirms the starting point is superior to the hip joint (teardrop) and directs the pin above the greater sciatic notch.
- Iliac Oblique View: Ensures the pin remains between the inner and outer tables of the ilium.
- Pin Insertion: A 5.0-mm or 6.0-mm Schanz pin is inserted to a depth of 4 to 6 cm, ensuring robust purchase in the dense bone above the acetabulum.
FRAME CONSTRUCTION
Regardless of the pin placement technique, the construction of the external frame must balance mechanical stability with patient accessibility.
A simple, modular frame is highly desired. The standard construct involves connecting the pins on each side to a short vertical rod, and then connecting these vertical rods with one or two transverse bars.
* Abdominal Access: The transverse bars must be positioned with sufficient clearance (at least 2-3 fingerbreadths) above the abdomen to accommodate abdominal distension, facilitate laparotomy, and allow for nursing care.
* Reduction: Once the frame is loosely assembled, manual compression is applied to the greater trochanters to close the open-book deformity. The clamps are then sequentially tightened to lock the pelvis in the reduced position.
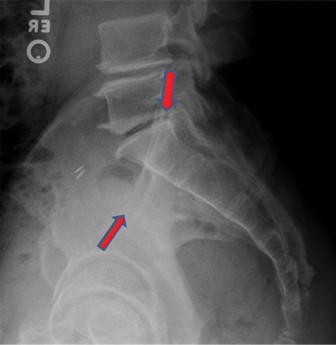
MANAGEMENT OF VERTICALLY UNSTABLE FRACTURES
Anterior external fixation alone is insufficient for vertically unstable pelvic fractures (e.g., APC-III, Vertical Shear injuries). These injuries involve complete disruption of both the anterior and posterior pelvic tension bands, leading to cranial migration of the hemipelvis driven by the powerful lumbar and abdominal musculature.
Vertically unstable fractures usually are treated with ipsilateral distal femoral skeletal traction in conjunction with the anterior external fixator.
* Traction Application: A heavy, threaded traction pin is placed from medial to lateral in the distal femur.
* Weight: Approximately 15 to 25 pounds of weight is applied to counteract the deforming muscular forces and restore leg length.
* Duration: Skeletal traction is maintained continuously until the patient is physiologically optimized and definitive internal fixation of the posterior ring can be safely performed.
TRANSITION TO DEFINITIVE INTERNAL FIXATION
While external fixation is a life-saving acute intervention, the gold standard for long-term functional recovery in unstable pelvic ring injuries is definitive internal fixation. Once the patient's physiologic parameters have normalized (typically days 3 to 10 post-injury), the external fixator is often removed and replaced with internal constructs.
Definitive internal fixation typically involves anterior symphyseal plating and posterior sacroiliac (SI) screw fixation. This provides superior biomechanical stability, allows for early mobilization, and eliminates the risks associated with prolonged external pin wear.
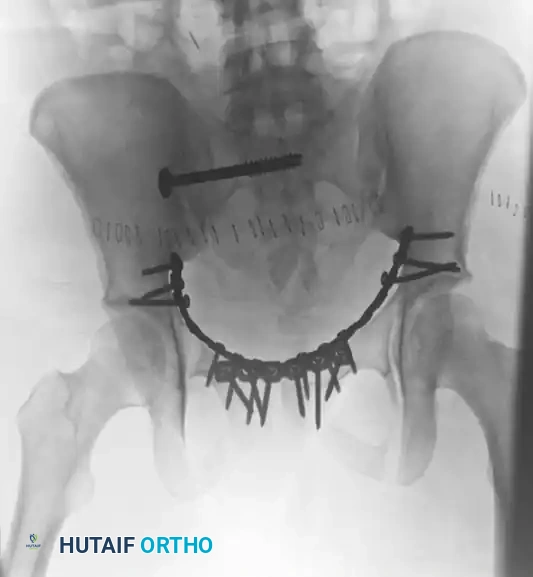
The following radiographic series demonstrates the successful transition to definitive internal fixation in a vertically unstable pelvic fracture, utilizing an anterior symphyseal plate and a posterior sacroiliac screw:
Postoperative Anteroposterior (AP) view demonstrating definitive internal fixation. Note the reduction of the symphysis pubis with a multi-hole plate and the stabilization of the posterior ring with an iliosacral screw.

Postoperative Inlet view. This projection critically evaluates the anterior-to-posterior translation of the pelvic ring and confirms that the sacroiliac screw is safely contained within the sacral vertebral body, avoiding the spinal canal anteriorly.

Postoperative Outlet view. This projection assesses the superior-to-inferior (vertical) displacement of the hemipelvis and confirms the extra-foraminal trajectory of the sacroiliac screw, ensuring the S1 and S2 nerve roots are protected.
POSTOPERATIVE PROTOCOLS AND COMPLICATIONS
Postoperative Care
- Pin Site Care: Meticulous pin site care is paramount. Protocols vary by institution, but daily cleaning with chlorhexidine or saline and the application of sterile, compressive dressings are standard to prevent pin-tract infections.
- Mobilization: If the external fixator is used as definitive fixation for a rotationally unstable (but vertically stable) injury, patients may be mobilized out of bed to a chair. Weight-bearing status is dictated by the specific fracture pattern, but is typically restricted (toe-touch or non-weight-bearing) on the affected side.
- Monitoring: Serial radiographs (AP, Inlet, Outlet) should be obtained weekly to monitor for loss of reduction or aseptic loosening of the pins.
Complications
- Pin-Tract Infection: The most common complication, occurring in up to 30-50% of patients. Superficial infections are managed with oral antibiotics and aggressive local care. Deep infections or osteomyelitis require pin removal and surgical debridement.
- Aseptic Loosening: Often a result of thermal necrosis during drilling or excessive mechanical stress on the frame. Loose pins lose their biomechanical efficacy and must be removed or revised.
- Neurological Injury: As noted, the LFCN is at high risk during supraacetabular pin placement. Injury results in meralgia paresthetica (numbness and dysesthesia over the anterolateral thigh).
- Loss of Reduction: External fixators are mechanically inferior to internal plates and screws. Gradual loss of reduction can occur, particularly in highly unstable patterns or non-compliant patients, necessitating close radiographic surveillance.
You Might Also Like