

Question 51
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?



Explanation
24b The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided. Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg 1997;6:544-548.
References:
- Ada Jr, Miller ME: Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-180.
Question 52
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?

Explanation
High-level pitchers with symptomatic UCL tears require reconstruction, with autograft being the best studied graft selection. With concomitant ulnar nerve symptoms, a simultaneous ulnar nerve transposition provides good results. Ligament "repairs" and allograft reconstructions have not shown good long-term results. Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
References:
- Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete's elbow. Instr Course Lect 1999;48:383-391.
Question 53
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?



Explanation
25b The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
References:
- Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of "floating elbow" injuries in adult patients. J Orthop Trauma 1998;12:284-290.
Question 54
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?



Explanation
26b The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern. Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
References:
- King GJ, Faber KJ: Posttraumatic elbow stiffness. Orthop Clin North Am 2000;31:129-143.
Question 55
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O'Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
Throwing athletes with symptomatic internal rotation deficits often benefit from an intensive posterior capsular stretching program. Patients that fail to respond to nonsurgical management may benefit from an arthroscopic posterior capsular release. Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
References:
- Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 56
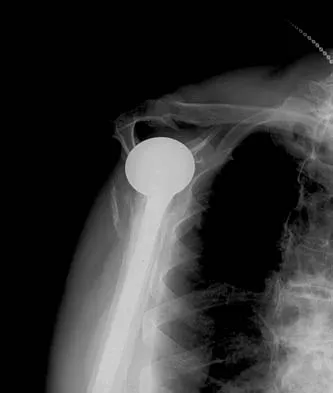
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?

Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
References:
- Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 57
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?


Explanation
The patient needs restrictions on his external rotation to allow healing of the subscapularis tendon repair. Limitation to 60 degrees is common if the tendon repair is robust and shows no evidence of tension on range-of-motion testing during the surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery. Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
References:
- Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 58
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?



Explanation
28b The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
References:
- Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 59
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?


Explanation
29b The patient has a nonunion of the proximal pole of the scaphoid. Acutely, this can be repaired with a screw alone, but as a nonunion the proximal pole has very poor healing potential. Vacularized bone grafts have been successful for these challenging nonunions, particularly in adolescents. A cast can be used for nondisplaced acute waist fractures, and corticocancellous grafts can be used for nonunions of the waist. Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.
References:
- Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.
Question 60
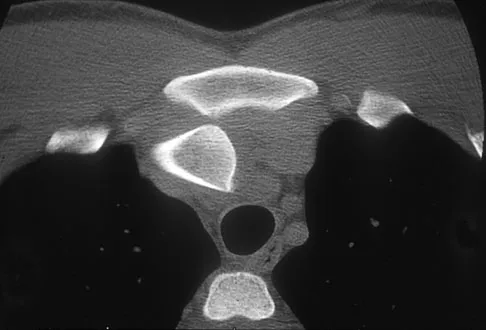
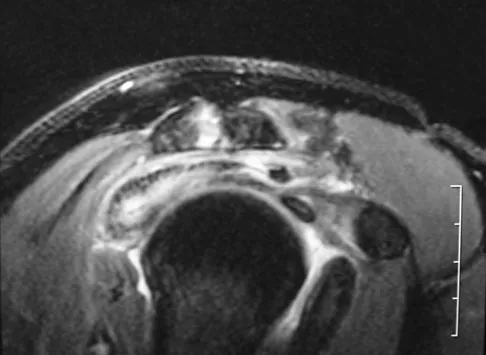
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?


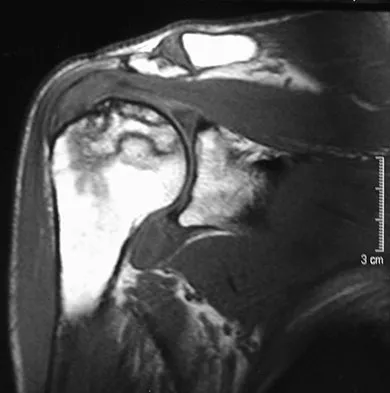
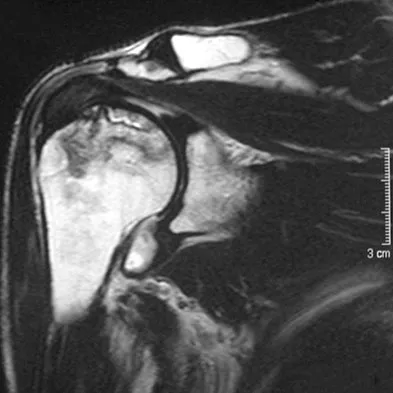
Explanation
30b 30c 30d The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient's history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis. Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
References:
- Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
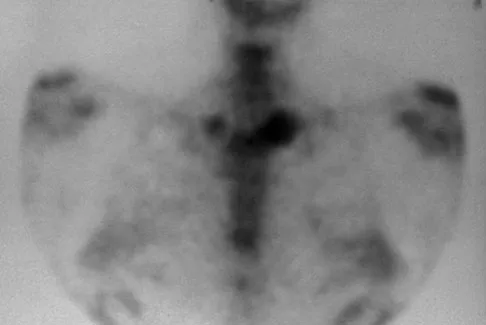
Question 61
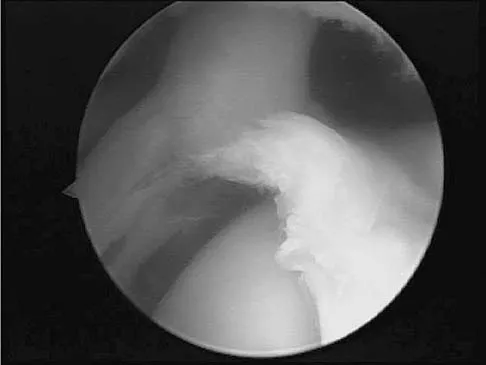
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?

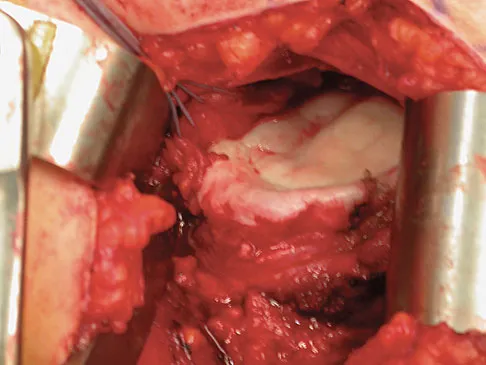
Explanation
31b The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future. Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
References:
- Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient. J Arthroplasty 2003;18:792-798.
Question 62
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?


Explanation
32b In an atrophic nonunion with a good soft-tissue envelope, adequate plating with cancellous bone graft can be used to span defects of up to 6 cm. Cortical graft from the fibula or iliac crest is not necessary. BMP-7 is a bone graft substitute and should not be used alone in this patient because the hardware is loose.
References:
- Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 63
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
References:
- Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 64
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. D'Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up. Am J Sports Med 2004;32:21-33. Levine WN, Clark AM Jr, D'Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 65
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
References:
- Kour AK, Looi KP, Phone MH, et al: Hand infections in patients with diabetes. Clin Orthop Relat Res 1996;331:238-244.
Question 66
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
Explanation
Through cadaveric study, Spencer and associates measured anterior and posterior translation of the sternoclavicular joint. The study demonstrated that the posterior sternoclavicular joint capsule is the most important structure for preventing both anterior and posterior translation of the sternoclavicular joint. Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
References:
- Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 67
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?

Explanation
34b The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
References:
- Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.
Question 68
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
References:
- Carlson JR, Simmons BP: Total wrist arthroplasty. J Am Acad Orthop Surg 1998;6:308-315.
Question 69
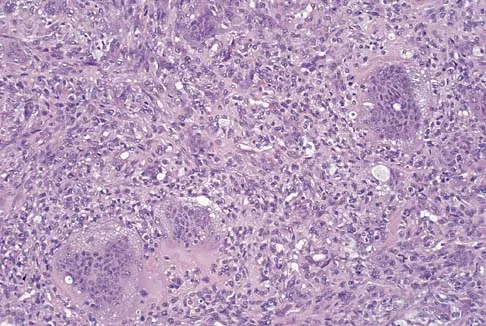
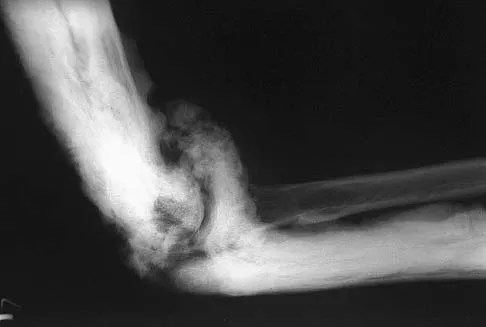
What is the most likely cause of the lesion shown in Figures 35a and 35b?


Explanation
35b The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
References:
- Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.
Question 70
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases, the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
References:
- Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 71
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
References:
- Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 72
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?

Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
References:
- Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 73
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
Essex-Lopresti injuries affect axial stability of the forearm. Injury to the interosseous membrane or the triangular fibrocartilage complex can result in proximal migration of the radius. Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
References:
- Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 74
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
In patients with radial nerve injuries with closed humeral fractures, it has been reported that 85% to 95% spontaneously recover. Based on this premise, most surgeons favor expectant management of these injuries. Even if there is no evidence of recovery at 6 weeks, repeat electromyography at 12 weeks is advocated. If there is no clinical or electromyographic signs of recovery at 6 months, exploration is recommended. If the nerve is in continuity at the time of exploration, nerve action potentials are useful in helping determine the need for neurolysis, excision, and grafting, or if excision and repair is the best option. Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
References:
- Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 75
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
References:
- Resch H, Povacz P, Ritter E, et al: Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon. J Bone Joint Surg Am 2000;82:372-382.
Finish Exam?
You cannot change answers after submitting.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-upper-extremity-2026-mcqs-exam-prep-3-3781
01
Chapter 1
108 min
100 Orthopedic MCQs: Trauma, Spine, Pediatrics & More | Comprehensive ABOS Review
02
Chapter 2
103 min
100 Orthopedic MCQs: Trauma, Spine, Peds, Adult Recon, & Sports Med Board Review
03
Chapter 3
101 min
100 Orthopedic MCQs: Trauma, Spine, Sports & Arthroplasty | Comprehensive ABOS Board Review
04
Chapter 4
106 min
100 Orthopedic MCQs: Trauma, Spine, Hand, Peds & Sports Med | Comprehensive ABOS Review
05
Chapter 5
105 min
100 Orthopedic MCQs: Trauma, Spine, Sports & Arthroplasty | Comprehensive ABOS Review
06
Chapter 6
114 min
100 Orthopedic MCQs: Trauma, Spine, Sports, Joints & Peds | Comprehensive ABOS Board Review
07
Chapter 7
104 min
100 Orthopedic MCQs: Trauma, Spine, Sports, Arthroplasty & Peds | Comprehensive ABOS Review
08
Chapter 8
101 min
100 Orthopedic MCQs: Trauma, Spine, Pediatrics & Adult Recon | Comprehensive ABOS Board Review
09
Chapter 9
107 min
100 Orthopedic MCQs: Trauma, Spine, Pediatrics, Sports Med & Basic Science | ABOS Board Review
10
Chapter 10
7 min
Upper Extremity Orthopedic MCQs (Set 6): Shoulder, Elbow & Wrist Trauma | ABOS Review
11
Chapter 11
29 min
Upper Extremity Orthopedic MCQs (Set 4): Shoulder, Elbow & Wrist Trauma | ABOS & OITE Board Review
12
Chapter 12
26 min
Anatomy Board Review MCQs (Set 4): Peripheral Nerves, Major Joints, & Muscle Anatomy | USMLE & ABOS Prep
13
Chapter 13
33 min
Pediatric Orthopedic MCQs (Set 4): DDH, SCFE, & Scoliosis for ABOS/OITE Exams
14
Chapter 14
31 min
Orthopedic Trauma Board Review MCQs (Set 2): Femoral & Tibial Fractures, Shoulder Dislocations
15
Chapter 15
32 min
AAOS Foot & Ankle MCQs (Set 4): Ankle Fractures & Hindfoot Deformities | Board Review
16
Chapter 16
29 min
AAOS & ABOS Orthopedic MCQs (Set 2): Foot & Ankle Trauma | Board Exam Prep
17
Chapter 17
28 min
AAOS Foot & Ankle MCQs (Set 1): Trauma & Degenerative Disorders | ABOS Review
18
Chapter 18
26 min
AAOS & ABOS Ortho MCQs (Set 5): Upper Extremity Trauma & Rotator Cuff | 2005 Board Prep
19
Chapter 19
30 min
AAOS & ABOS Upper Extremity MCQs (Set 4): Shoulder, Elbow, Wrist, Hand & Nerve Review | 2025-2026 Boards
20
Chapter 20
31 min
AAOS Orthopedic MCQs (Set 3): Shoulder, Elbow & Wrist Trauma | 2005 Board Review
21
Chapter 21
31 min
Upper Extremity Orthopedic MCQs (Set 2): Shoulder, Elbow, Wrist & Hand | ABOS & AAOS Board Review
22
Chapter 22
29 min
AAOS Orthopedic MCQs (Set 1): Upper Extremity Trauma & Sports Injuries | Board Review
23
Chapter 23
25 min
AAOS & ABOS Basic Science MCQs (Set 4): Bone Biology, Biomechanics & Physiology | Orthopedic Board Prep
24
Chapter 24
28 min
AAOS Basic Science MCQs (Set 3): Bone & Cartilage Biology, Ortho Biomechanics | ABOS Exam Prep
25
Chapter 25
27 min
AAOS Basic Science MCQs (Set 2): Bone Healing & Orthopedic Biomechanics | ABOS, OITE Prep
26
Chapter 26
27 min
AAOS Basic Science MCQs (Set 1): Bone Physiology, Biomechanics & Pharmacology | Ortho Board Review
27
Chapter 27
26 min
Anatomy Board Review MCQs (Set 4): Peripheral Nerve & Musculoskeletal Systems | AAOS ABOS OITE
28
Chapter 28
26 min
AAOS & ABOS Anatomy MCQs (Set 3): Musculoskeletal & Skeletal System Questions | Board Review
29
Chapter 29
26 min
AAOS & ABOS Anatomy MCQs (Set 1): Upper Limb, Lower Limb & Spine | 2025 Board Prep
30
Chapter 30
31 min
AAOS Sports Medicine MCQs (Set 4): Knee Ligament & Shoulder Instability | ABOS Board Review
31
Chapter 31
32 min
AAOS/ABOS Sports Medicine MCQs (Set 3): Knee, Shoulder & Ankle Trauma | OITE & Board Review
32
Chapter 32
30 min
AAOS Sports Medicine MCQs (Set 2): Knee Ligament & Rotator Cuff Injuries | Board Review
33
Chapter 33
32 min
AAOS & ABOS Sports Medicine MCQs (Set 1): Knee, Shoulder & Concussion | Board Review
34
Chapter 34
37 min
Pediatric Orthopedic MCQs (Set 4): Hip, Spine & Trauma | ABOS OITE 2004 Review
35
Chapter 35
33 min
AAOS Pediatric Orthopedic MCQs (Set 3): Scoliosis, DDH & Fractures | 2004 Board Review
36
Chapter 36
28 min
AAOS & ABOS Board Review (Set 4): Proximal Femur Fractures & Hip Dislocations MCQs
37
Chapter 37
29 min
AAOS Hip MCQs (Set 3): Femoral Neck Fractures & Arthroplasty | ABOS Board Review
38
Chapter 38
29 min
AAOS & ABOS Orthopedic MCQs (Set 2): Hip Fractures & Arthroplasty | Board Prep
39
Chapter 39
29 min
AAOS Orthopedic MCQs (Set 1): Hip Fractures & Arthroplasty | ABOS Board Review 2004
40
Chapter 40
34 min
AAOS & ABOS Shoulder Board Review MCQs (Set 4): Rotator Cuff, Instability & Proximal Humerus
41
Chapter 41
33 min
ABOS Shoulder MCQs (Set 3): Rotator Cuff & Glenoid Instability | OITE & Board Prep
42
Chapter 42
32 min
AAOS Shoulder Board Review MCQs (Set 2): Rotator Cuff, Instability & Proximal Humerus Fractures
43
Chapter 43
32 min
AAOS Shoulder MCQs (Set 1): Rotator Cuff, Instability & Humerus Fractures | ABOS Board Prep
44
Chapter 44
25 min
AAOS Basic Science MCQs (Set 4): Bone Healing, Cartilage Biology & Biomechanics | ABOS Exam Prep
45
Chapter 45
25 min
AAOS Basic Science Orthopedic MCQs (Set 3): Bone Metabolism, Biomechanics & Cartilage Biology | Board Review
46
Chapter 46
26 min
AAOS Basic Science MCQs (Set 2): Bone Physiology & Biomechanics | 2002 Board Review
47
Chapter 47
25 min
AAOS Basic Science MCQs (Set 1, 2002): Biomechanics, Bone Healing & Anatomy for ABOS & OITE
48
Chapter 48
27 min
AAOS Orthopedic Anatomy MCQs (Set 4): Upper Extremity & Pelvic Hip Review
49
Chapter 49
26 min
AAOS Orthopedic Anatomy MCQs (Set 3): Musculoskeletal & Skeletal System | ABOS Board Prep
50
Chapter 50
25 min
AAOS & ABOS Anatomy MCQs (Set 2): Musculoskeletal, Neuro, & Regional Topography for Board Review
51
Chapter 51
26 min
Orthopedic Anatomy MCQs (Set 1): Spine, Upper & Lower Limb | AAOS ABOS 2002 Review
52
Chapter 52
32 min
AAOS & ABOS Sports Medicine MCQs (Set 4): Knee Ligament & Meniscal Injuries | Board Review
53
Chapter 53
31 min
AAOS Sports Medicine MCQs (Set 3): Knee & Shoulder Ligament Trauma | OITE & ABOS Review
54
Chapter 54
33 min
AAOS Sports Medicine MCQs (Set 2): Knee & Shoulder Injuries | ABOS Board Review
55
Chapter 55
33 min
AAOS & ABOS Sports Medicine MCQs (Set 1): Knee, Shoulder & Ankle Injuries | Board Review
56
Chapter 56
35 min
AAOS Pediatric Orthopedics MCQs (Set 4): DDH, SCFE & Supracondylar Humerus | Board Review
57
Chapter 57
36 min
Pediatric Orthopedic MCQs (Set 3): Fractures, DDH & Scoliosis | AAOS & ABOS Review
58
Chapter 58
35 min
AAOS Pediatrics Board Review MCQs (Set 2): DDH, Fractures & Scoliosis | ABOS 2001
59
Chapter 59
28 min
Orthopedic Hip MCQs (Set 4): Femoral Neck Fractures, THA Complications & FAI | AAOS & ABOS Review
60
Chapter 60
27 min
AAOS & ABOS Hip MCQs (Set 3): Anatomy, Pathology & Trauma | OITE Board Prep
61
Chapter 61
34 min
AAOS & ABOS Hip Board Review MCQs (Set 2): Fractures, Arthroplasty, & Pathology
62
Chapter 62
28 min
AAOS/ABOS Hip MCQs (Set 1): Anatomy, Trauma & Arthroplasty | Board Prep
63
Chapter 63
34 min
AAOS, ABOS, SMLE Orthopedic Trauma MCQs (Set 4): Tibial Plateau, Pilon, & Polytrauma Management
64
Chapter 64
37 min
AAOS Orthopedic MCQs (Set 3): Long Bone Fractures & Joint Dislocations | 2026 Board Review
65
Chapter 65
34 min
AAOS & ABOS Orthopedic Trauma MCQs (Set 2): Tibial Plateau, Distal Radius Fractures & Polytrauma | 2000 Board Review
66
Chapter 66
35 min
Orthopedic Trauma MCQs (Set 1): Femur, Tibia Fractures & Polytrauma | AAOS ABOS OITE Review
67
Chapter 67
28 min
AAOS & ABOS Spine Surgery MCQs (Set 4): Vertebral Fractures & Adult Deformity | 2000 Board Review
68
Chapter 68
31 min
AAOS Spine Surgery MCQs (Set 3): Degenerative Spine, Trauma & Deformity | ABOS & OITE Review
69
Chapter 69
33 min
AAOS Spine Surgery MCQs (Set 2): Lumbar Stenosis & Thoracolumbar Fractures | Board Review
70
Chapter 70
30 min
AAOS Spine Surgery MCQs (Set 1): Degenerative, Trauma & Deformity | ABOS Board Review 2024
71
Chapter 71
26 min
ABOS Foot & Ankle MCQs (Set 4): Ankle Fractures & Diabetic Foot | OITE & SMLE Review
72
Chapter 72
31 min
AAOS Orthopedic MCQs (Set 3): Foot & Ankle Trauma & Pathology | ABOS Board Prep
73
Chapter 73
30 min
AAOS & ABOS Foot & Ankle Board Review MCQs (Set 2): Ankle Fractures, Lisfranc, Diabetic Foot
74
Chapter 74
27 min
AAOS Foot & Ankle MCQs (Set 1): Fractures, Deformities & Sports Injuries | Board Prep
75
Chapter 75
34 min
AAOS Shoulder MCQs (Set 4): Rotator Cuff, Instability & Fractures | Board Review
76
Chapter 76
33 min
Shoulder Orthopedics MCQs (Set 3): Rotator Cuff, Instability & Proximal Humerus | ABOS Board Review
77
Chapter 77
32 min
ABOS Shoulder MCQs (Set 2): Rotator Cuff, Instability & Fractures | Board Review
78
Chapter 78
32 min
Shoulder Orthopedic MCQs (Set 1): Rotator Cuff & Instability | AAOS & ABOS Board Review
79
Chapter 79
25 min
Orthopedic Basic Science MCQs (Set 4): Biomechanics, Bone Physiology & Biomaterials | AAOS, ABOS Review
80
Chapter 80
25 min
AAOS & ABOS Basic Science MCQs (Set 3): Orthopedic Biomechanics & Bone Physiology | OITE Review
81
Chapter 81
26 min
AAOS & ABOS Basic Science MCQs (Set 2): Biomechanics, Anatomy & Bone Healing
82
Chapter 82
25 min
AAOS & ABOS Orthopedic Basic Science MCQs (Set 1): Anatomy, Biomechanics & Bone Biology | OITE Prep
83
Chapter 83
27 min
AAOS Orthopedic Anatomy Board Review (Set 4): Hip & Pelvic Girdle MCQs | ABOS, SMLE
84
Chapter 84
26 min
Orthopedic Anatomy MCQs (Set 3): Bone Structure, Joint Kinematics & Ligaments | ABOS & AAOS Review
85
Chapter 85
25 min
Anatomy Board Review (Set 2): Musculoskeletal & Neurovascular MCQs | AAOS, ABOS Prep
86
Chapter 86
26 min
Orthopedic Anatomy MCQs (Set 1): Shoulder, Knee, Spine | AAOS & ABOS Exam Prep
87
Chapter 87
30 min
AAOS/ABOS Orthopedic Trauma MCQs (Part 4): Lower Extremity & Polytrauma Management | 2026 Board Review
88
Chapter 88
29 min
Orthopedic Trauma MCQs (Part 3): Upper & Lower Extremity Fractures | AAOS & ABOS 2026 Review
89
Chapter 89
30 min
Orthopedic Trauma MCQs (Part 2): Fracture Management & Emergency Injuries | AAOS, ABOS 2026 Review
90
Chapter 90
32 min
Orthopedic Trauma 2026 MCQs (Part 1): Fracture Management & Emergency Orthopedics | Board Review
91
Chapter 91
32 min
Orthopedic Spine 2026 MCQs (Part 4): Deformity, Trauma & Degenerative Conditions | AAOS & ABOS Board Review
92
Chapter 92
32 min
AAOS & ABOS Orthopedic Spine MCQs (Part 3): Cervical Myelopathy, Lumbar Stenosis | 2026 Board Prep
93
Chapter 93
34 min
ABOS Orthopedic Spine MCQs (Set 2): Degenerative Lumbar & Cervical Trauma | 2026 Board Review
94
Chapter 94
30 min
AAOS Orthopedic Spine MCQs (Part 1): Spinal Trauma & Degenerative Conditions | 2026 Board Review
95
Chapter 95
31 min
Orthopedic Foot & Ankle MCQs (Part 4): ABOS & AAOS Board Review 2026
96
Chapter 96
31 min
AAOS Orthopedic Foot & Ankle MCQs (Set 3): Ankle Trauma & Deformities | 2026 Board Review
97
Chapter 97
32 min
Orthopedic Foot & Ankle 2026 MCQs: Board Review Questions & Answers (Part 2)
98
Chapter 98
33 min
Orthopedic Foot & Ankle 2026 MCQs: Board Review Questions & Answers (Part 1)
99
Chapter 99
6 min
Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 6)
100
Chapter 100
24 min