Knee Biomechanics and Kinematics: A Comprehensive Surgical Guide
Key Takeaway
The knee joint functions as a complex ginglymus and trochoid articulation, relying on a sophisticated interplay of rocking and gliding motions. Understanding the mechanical and anatomical axes, the screw-home mechanism, and the synergistic antagonism of the cruciate and collateral ligaments is paramount. This foundational biomechanical knowledge dictates surgical decision-making in total knee arthroplasty, osteotomies, and complex ligamentous reconstructions, ensuring the restoration of the joint's instant center of rotation and long-term survivorship.
Introduction to Knee Biomechanics
A profound understanding of knee biomechanics is the cornerstone of successful orthopedic surgery, dictating the principles of joint reconstruction, ligamentous repair, and deformity correction. The knee is not a simple hinge; it is a highly sophisticated, multi-axial joint that must simultaneously provide rigid stability during the stance phase of gait and extensive mobility during the swing phase.
For the practicing orthopedic surgeon, resident, or fellow, mastering the mechanical and anatomical axes, the kinematics of the tibiofemoral articulation, and the complex interplay of the capsuloligamentous structures is non-negotiable. Failure to respect these biomechanical principles during procedures such as Total Knee Arthroplasty (TKA) or Anterior Cruciate Ligament (ACL) reconstruction inevitably leads to altered kinematics, accelerated polyethylene wear, graft failure, and suboptimal clinical outcomes.
Mechanical and Anatomical Axes of the Lower Extremity
The foundational principle of lower extremity alignment lies in the distinction between the anatomical and mechanical axes of the femur and tibia.
The anatomical axis of the femur is a line drawn down the center of the medullary canal. Conversely, the mechanical axis of the femur (the weight-bearing line) is a line traversing the center of the femoral head to the center of the knee joint (intercondylar notch).
Because of the proximal femoral offset and the femoral neck angle, the mechanical axis of the femur does not coincide with its anatomical axis. Instead, the anatomical axis forms an angle of 6 to 9 degrees of valgus relative to the mechanical axis.
Clinical Pearl: During Total Knee Arthroplasty, the distal femoral cut is typically made at 5 to 7 degrees of valgus relative to the intramedullary alignment rod (which approximates the anatomical axis) to ensure the joint line is perpendicular to the mechanical axis. Failure to accurately template this angle based on the patient's specific anatomy can lead to coronal malalignment.
In a normal, well-aligned lower extremity in the erect position, the mechanical axis of the entire lower limb (the Mikulicz line) passes from the center of the femoral head, through or just medial to the center of the knee joint, to the center of the ankle mortise. The transverse axis through the knee joint lies in or near the true horizontal plane. Significant deviations from this mechanical axis manifest as genu varum (bowlegged) or genu valgum (knock-kneed) deformities, which exponentially increase compartmental contact stresses and precipitate unicompartmental osteoarthritis.
Kinematics of the Tibiofemoral Joint
The knee possesses features characteristic of both a ginglymus (hinge joint) and a trochoid (pivot joint) articulation. It permits primary flexion and extension in the sagittal plane, coupled with a critical degree of internal and external rotation when the joint is flexed. Notably, no rotation is possible when the knee is in full, locked extension due to the tension of the posterior capsule and collateral ligaments.
The Roll-and-Glide Mechanism
Because of the stark disparity between the lengths of the articular surfaces of the femoral condyles (which are long and convex) and the tibial plateaus (which are relatively short and flat/concave), simple hinge motion is impossible. If the femur only rolled on the tibia, it would roll off the posterior edge of the tibial plateau during deep flexion.
To accommodate this, the complex flexion-extension motion is a combination of rocking (rolling) and gliding (sliding).
The transition from rocking to gliding is essential for maintaining joint congruency and maximizing the range of motion without posterior subluxation.
- Early Flexion (0 to 20 degrees): The motion is predominantly a rocking (rolling) motion. This rolling motion better meets the requirements for stability of the knee in the relatively extended position, allowing for rapid weight acceptance during the early stance phase of gait.
- Deep Flexion (>20 degrees): The motion transitions progressively to a predominantly gliding (sliding) type. As the joint "unwinds," this gliding motion permits more freedom for axial rotation. The ratio of rolling to gliding changes dynamically; in deep flexion, the motion is almost pure glide.
The Instant Center of Rotation
Because of the eccentricity (multi-radius nature) of the femoral condyles, the transverse axis of rotation is not fixed. It constantly changes position as the knee progresses from extension into flexion, creating an instant center of rotation.
Pioneering kinematic studies by Frankel, Burstein, and Brooks demonstrated that the instant center of rotation pathway is semi-circular in a normal knee. When ligaments are disrupted or menisci are torn, this pathway becomes erratic. Changes in the instant center of rotation are detectable kinematically and are directly responsible for abnormal surface velocities, increased shear forces, and the subsequent degenerative osteoarthritic conditions noted around the joint.
Surgical Warning: In ligamentous reconstruction, non-anatomic tunnel placement fails to restore the native instant center of rotation. This results in graft stretching (if placed too far from the isometric point) or joint capture (loss of motion), ultimately leading to early graft failure and progressive chondral damage.
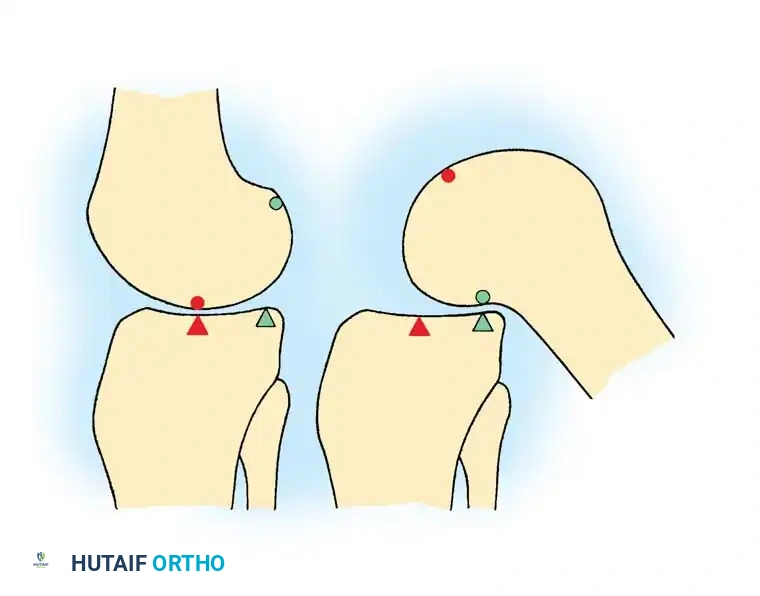
The Screw-Home Mechanism and Terminal Extension
The natural deflection outward of the tibia on the femur at the knee joint produces greater weight-bearing stresses on the lateral femoral condyle than on the medial condyle. However, the articular surface of the medial condyle is prolonged farther anteriorly than the lateral condyle. Consequently, the vertical axis of rotation falls in a plane near the medial condyle.
This anatomical asymmetry is the driving force behind the "screw-home" mechanism, an obligate rotation that locks the knee in terminal extension:
- Locking (Terminal Extension): As the knee comes into the fully extended position, the shorter lateral condylar articular surface is exhausted first. The femur must internally rotate (or the tibia externally rotates, depending on whether the foot is planted) until the remaining anterior articular surface on the medial condyle comes into contact. The posterior portion of the lateral condyle rotates forward laterally, locking the knee into a highly stable, energy-efficient extended position.
- Unlocking (Initiation of Flexion): When flexion is initiated, the popliteus muscle contracts, causing an "unscrewing" of the joint by externally rotating the femur on the tibia (or internally rotating the tibia on the femur).
This rotary movement responsible for screwing and unscrewing occurs around an axis passing near the medial condyle and is profoundly influenced by the tension and integrity of the Posterior Cruciate Ligament (PCL).
Ligamentous Interplay: Synergism and Antagonism
The stability of the knee is governed by a complex four-bar linkage system comprising the Anterior Cruciate Ligament (ACL), Posterior Cruciate Ligament (PCL), Medial Collateral Ligament (MCL), and Lateral Collateral Ligament (LCL).
As described by Müller (1983), in addition to their synergistic functions in providing multi-planar stability, the cruciate and collateral ligaments exercise a basic antagonistic function during axial rotation.
External Rotation
During external rotation of the tibia on the femur, the collateral ligaments (MCL and LCL) tighten. They inhibit excessive rotation by becoming crossed in space, acting as the primary secondary restraints to external rotatory forces.
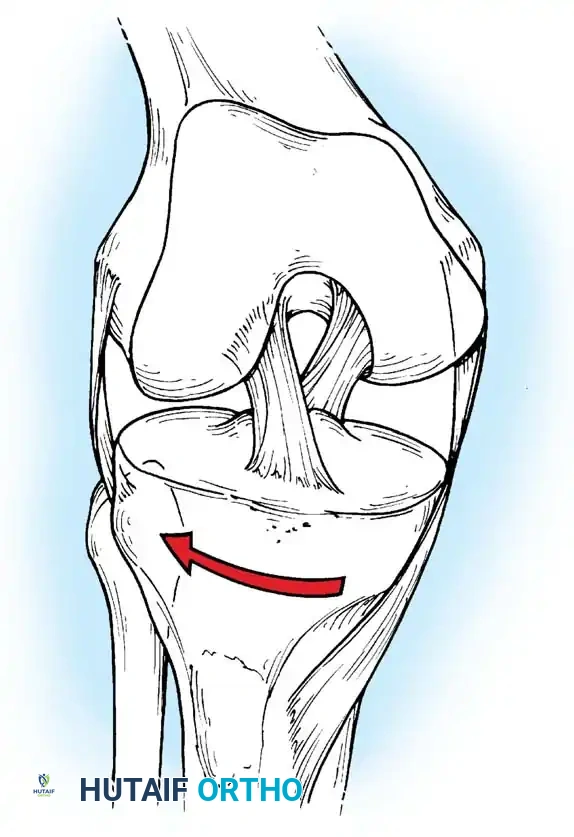
External rotation A: The collateral ligaments tighten and cross in space, limiting further external excursion.
Neutral Rotation
In a state of neutral rotation, the capsuloligamentous structures are balanced. None of the four primary ligaments (ACL, PCL, MCL, LCL) is under unusual or asymmetric tension, allowing for optimal load distribution across the medial and lateral compartments.
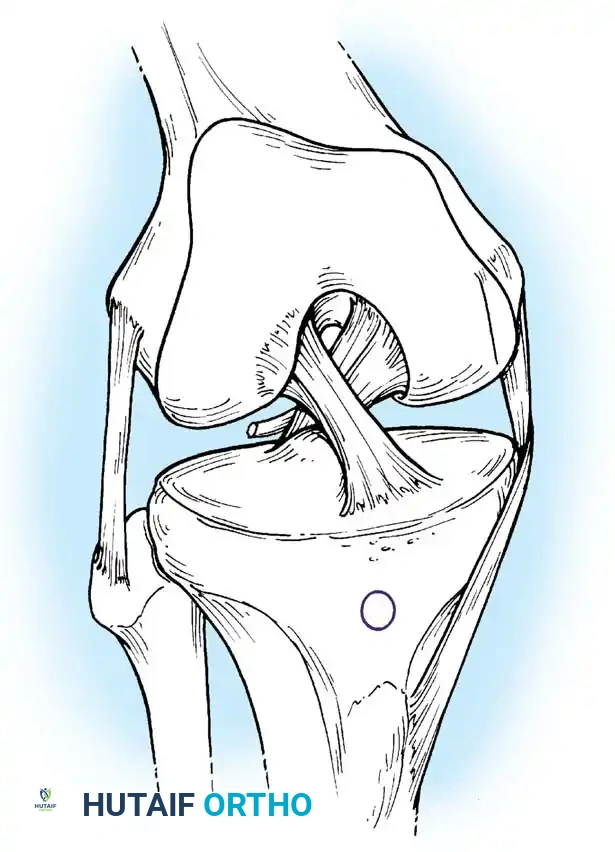
Neutral rotation B: Balanced tension across the cruciate and collateral ligaments.
Internal Rotation
During internal rotation of the tibia on the femur, the collateral ligaments become more vertical and relatively lax. Conversely, the cruciate ligaments (ACL and PCL) become coiled around each other and come under strong tension, acting as the primary checkreins to excessive internal rotation.
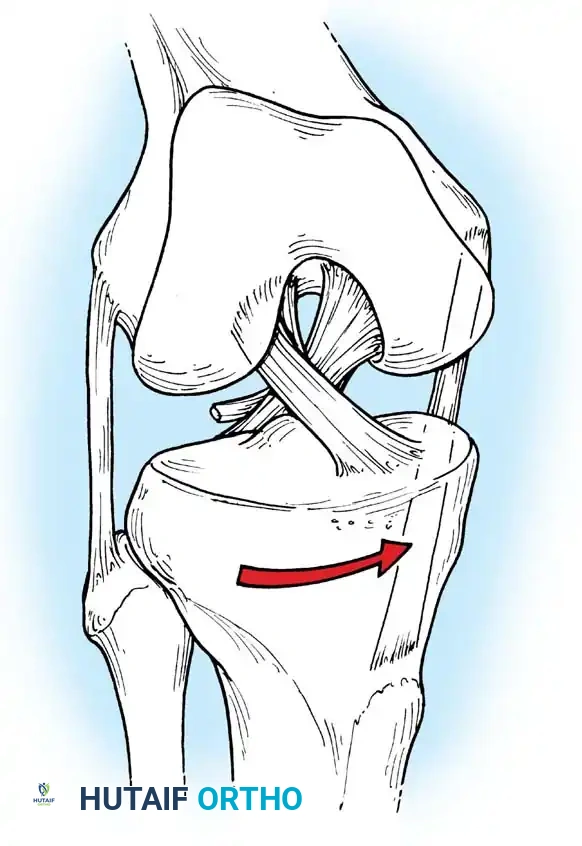
Internal rotation C: The cruciate ligaments coil and tighten, while the collateral ligaments become vertical and lax.
Range of Motion and Physiologic Laxity
A thorough clinical examination requires an understanding of normal physiologic limits to accurately diagnose pathologic laxity.
- Sagittal Plane (Flexion/Extension): Normal flexion ranges from 0 to 140 degrees. However, 5 to 10 degrees of physiologic hyperextension is often possible, particularly in ligamentously lax individuals.
- Axial Plane (Rotation): With the knee flexed to 90 degrees, passive rotation of the tibia on the femur can be demonstrated up to 25 or 30 degrees. The extent of internal rotation always exceeds that of external rotation. No rotation is possible with the knee fully extended.
- Translational Laxity: Sagittal displacement (anterior-posterior translation) of the tibia on the fixed femur is detectable when the knee is flexed. Under normal conditions, the extent of this excursion should not exceed 3 to 5 mm.
- Coronal Plane (Varus/Valgus): When the knee is extended, lateral (abduction-adduction) motion occurs to a very limited extent, varying with individual characteristics but strictly not exceeding 6 to 8 degrees. In the hyperextended position, no lateral motion should be present. In the flexed position, more lateral motion is possible but should never exceed 15 degrees.
Alterations in the vertical and transverse axes occur with disruptions of the knee joint. For example, when the medial structures (MCL, posteromedial corner) are disrupted, the vertical axis of rotation shifts laterally, leading to anteromedial rotatory instability (AMRI).
Surgical Implications and Operative Applications
Total Knee Arthroplasty (TKA)
The primary goal of TKA is to restore the mechanical axis to neutral (0 degrees) while balancing the soft tissue envelope to recreate normal kinematics.
- Gap Balancing: The surgeon must ensure that the flexion gap (determined by the posterior femoral cut and the tension of the collateral ligaments in flexion) equals the extension gap (determined by the distal femoral cut and the posterior capsule/collaterals in extension).
- Implant Design: Cruciate-Retaining (CR) implants rely on an intact PCL to facilitate the physiologic roll-and-glide mechanism and femoral rollback during deep flexion. Posterior-Stabilized (PS) implants utilize a cam-and-post mechanism to mechanically substitute for the PCL, forcing femoral rollback and preventing anterior tibial translation in flexion.
- Joint Line Restoration: Elevating the joint line alters the instant center of rotation, leading to mid-flexion instability and patella baja kinematics, which significantly increases patellofemoral contact forces and anterior knee pain.
Ligamentous Reconstruction
When reconstructing the ACL or PCL, the surgeon must respect the antagonistic and synergistic functions of the ligaments.
- Tunnel Placement: The femoral and tibial tunnels must be placed at the anatomic footprints to restore the native kinematics. An ACL graft placed too vertically (a common error with transtibial drilling techniques) fails to control rotational instability, even if it eliminates anterior tibial translation (a negative Lachman test but a positive pivot-shift test).
- Tensioning: The graft must be tensioned at the appropriate degree of flexion (typically 20-30 degrees for the ACL, and 90 degrees for the PCL) to avoid over-constraining the joint and altering the screw-home mechanism.
Corrective Osteotomies
High Tibial Osteotomy (HTO) and Distal Femoral Osteotomy (DFO) are utilized to mechanically unload a diseased compartment by shifting the mechanical axis.
- Medial Compartment OA: A medial opening-wedge HTO is performed to shift the mechanical axis laterally, typically targeting a point 62% across the tibial plateau (Fujisawa point) to slightly overcorrect into valgus, thereby unloading the medial articular cartilage and preserving the native joint kinematics.
Postoperative Rehabilitation Protocols
Rehabilitation following knee surgery must be meticulously phased to protect surgical repairs while restoring normal biomechanics.
- Phase I (0-2 Weeks) - Protection and Early Motion: Focus on restoring terminal extension to re-engage the screw-home mechanism. Passive and active-assisted flexion is initiated to prevent capsular adhesions, respecting the 0-20 degree rocking phase.
- Phase II (2-6 Weeks) - Kinematic Restoration: Gradual restoration of deep flexion (the gliding phase). In ligamentous reconstructions, closed kinetic chain exercises (e.g., leg presses) are preferred over open kinetic chain exercises to minimize shear forces across the graft and utilize the co-contraction of the hamstrings and quadriceps for dynamic stability.
- Phase III (6-12+ Weeks) - Rotational and Proprioceptive Recovery: Introduction of rotational torque and pivoting movements. This phase relies heavily on the healed synergistic/antagonistic interplay of the cruciates and collaterals. Proprioceptive training ensures dynamic muscular control over the instant center of rotation during high-demand activities.
By strictly adhering to these biomechanical principles, the orthopedic surgeon ensures not only the structural integrity of the repair but the functional restoration of the knee's complex, multi-axial kinematics.
📚 Medical References
You Might Also Like


