Surgical Management of Group 2 Clasped Thumb Deformity and Hypoplastic Digits
Key Takeaway
Group 2 clasped thumb deformity is a complex congenital anomaly characterized by a deficient extensor mechanism and severe first web space contracture. Surgical correction is typically staged, beginning with web space release, followed by tendon transfer—most commonly utilizing the extensor indicis proprius (EIP) or flexor digitorum superficialis (FDS)—to restore thumb extension. This guide details the indications, biomechanics, and step-by-step operative techniques for optimal functional restoration.
Introduction to Congenital Clasped Thumb Deformities
Congenital clasped thumb is a complex pediatric hand deformity characterized by a thumb that is rigidly or passively flexed and adducted across the palm. This posture results from a profound biomechanical imbalance between the robust flexor-adductor mechanism and a deficient or entirely absent extensor-abductor mechanism.
The deformity is classically categorized into three distinct groups based on severity and anatomical involvement:
* Group 1: Supple clasped thumb with isolated deficiency of the extensor pollicis brevis (EPB) and/or extensor pollicis longus (EPL).
* Group 2: Complex clasped thumb featuring severe extensor deficiency combined with rigid adduction contracture of the first web space, often involving fascial, muscular, and cutaneous shortening.
* Group 3: Clasped thumb associated with generalized systemic syndromes, such as arthrogryposis multiplex congenita, featuring severe joint contractures and widespread soft tissue abnormalities.
This comprehensive guide focuses on the surgical management of Group 2 Clasped Thumb Deformity, which necessitates a meticulously staged reconstructive approach to restore both the first web space span and active thumb extension. Additionally, we will explore the pathoanatomy and genetic principles underlying hypoplastic hands and digits.
Pathoanatomy and Biomechanical Considerations
In a Group 2 clasped thumb, the primary pathoanatomic lesion is twofold. First, there is a structural contracture of the first web space. This is not merely a skin deficiency; it typically involves contracture of the adductor pollicis, the first dorsal interosseous fascia, and occasionally the carpometacarpal (CMC) joint capsule. Second, the extensor mechanism (EPL and EPB) is either severely hypoplastic, attenuated, or completely absent.
Biomechanically, the flexor pollicis longus (FPL) and the intrinsic thenar muscles operate unopposed. Over time, if left untreated, this dynamic imbalance leads to secondary skeletal deformities, including subluxation of the metacarpophalangeal (MCP) joint and progressive joint stiffness. Surgical intervention must address both the static contracture and the dynamic imbalance to achieve a functional, stable pinch and grasp.
Preoperative Evaluation and Surgical Strategy
Surgical correction of a Group 2 clasped thumb is rarely a single-stage procedure. Attempting to simultaneously release a severe web space contracture and perform a tendon transfer often compromises the vascularity of the skin flaps and places undue tension on the tendon repair. Therefore, a staged approach is the gold standard.
- Stage I: Release of the first web space contracture. This is typically achieved using deep tissue release (adductor fascia) combined with local tissue rearrangement, such as a four-flap Z-plasty, a dorsal rotational advancement flap, or occasionally a full-thickness skin graft.
- Stage II: Restoration of active thumb extension via tendon transfer. This stage is performed only after the web space has fully healed and supple passive abduction and extension have been achieved.
Clinical Pearl: Never proceed to Stage II tendon transfer if passive extension and abduction of the thumb are not fully achievable. A tendon transfer cannot overcome a fixed joint or soft-tissue contracture.
Stage II: Restoration of Thumb Extension (Neviaser Technique)
The workhorse for restoring thumb extension in a Group 2 clasped thumb is the transfer of the Extensor Indicis Proprius (EIP) to the extensor mechanism of the thumb, often referred to as the Neviaser transfer. The EIP is an ideal donor because its line of pull is highly synergistic with thumb extension, its excursion is appropriate, and its harvest leaves the index finger with independent extension via the extensor digitorum communis (EDC).
Indications
- Absent or severely hypoplastic EPB/EPL.
- Supple first web space (post-Stage I release).
- Adequate passive range of motion at the thumb CMC, MCP, and interphalangeal (IP) joints.
Step-by-Step Surgical Technique (EIP Transfer)
1. Patient Positioning and Preparation
The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The limb is exsanguinated, and the tourniquet is inflated to an age- and weight-appropriate pressure.
2. Donor Tendon Harvest (EIP)
* Make a short transverse incision at the dorsal base of the index metacarpal.
* Carefully dissect through the subcutaneous tissue to locate the extensor hood. Identify the EIP tendon, which consistently lies on the ulnar aspect of the EDC tendon to the index finger.
* Divide the EIP tendon at its distal confluence with the extensor hood. Repair the hood defect with fine absorbable sutures to prevent extensor lag of the index finger.
* Make a second short transverse incision over the dorsum of the wrist, directly in line with the EIP tendon.
* Gently withdraw the EIP tendon proximally into the wrist wound, ensuring there are no restrictive fascial bands tethering the muscle belly.
3. Recipient Site Preparation
* Make a bayonet-shaped incision over the dorsoulnar aspect of the thumb, centered precisely over the metacarpophalangeal (MCP) joint.

- Carefully elevate the skin flaps, taking extreme caution to identify and protect the dorsal sensory branches of the radial nerve.
- Identify the remnants of the extensor pollicis longus (EPL) tendon, if present, and retract it to one side.
- Expose the base of the proximal phalanx.
4. Creation of the Osseous Tunnel
* Using a fine drill or a specialized tendon passer, create a transverse osseous tunnel through the base of the proximal phalanx.
* The tunnel must be directed from the ulnar aspect to the radial aspect.
Surgical Warning: In pediatric patients, it is critical to place this osseous tunnel strictly distal to the proximal phalangeal epiphysis to avoid iatrogenic physeal arrest and subsequent growth deformity.
5. Tendon Routing and Fixation
* Create a wide, unrestricted subcutaneous tunnel from the dorsal wrist incision to the bayonet incision at the base of the thumb.
* Reroute the EIP tendon subcutaneously through this path. Ensure the line of pull is direct and free of kinks.
* Pass the distal end of the EIP tendon through the prepared osseous tunnel in the proximal phalanx.
- Loop the tendon back onto itself. Apply appropriate tension—the thumb should rest in full extension and slight abduction with the wrist in neutral.
- Suture the tendon securely to itself using a non-absorbable, braided suture (e.g., 3-0 or 4-0 polyester) using a Pulvertaft weave or a robust side-to-side anastomosis.
6. Joint Fixation and Closure
* To protect the tendon transfer during the initial healing phase, fix the thumb MCP and IP joints in full extension using a longitudinally placed smooth Kirschner wire (K-wire).
* Deflate the tourniquet, achieve meticulous hemostasis, and close all incisions in a routine fashion using fine absorbable sutures for the skin.
* Apply a sterile dressing and a well-padded long-arm plaster splint, immobilizing the thumb in extension and wide abduction, and the wrist in slight extension.
Alternative Tendon Transfers: FDS or Brachioradialis
In cases where the EPL is entirely absent, severely deficient, or if the EIP is unavailable or inadequate, alternative donor muscles must be utilized. The two primary alternatives are the Flexor Digitorum Superficialis (FDS) of the ring finger or the Brachioradialis (BR) extended with a palmaris longus tendon graft.
Flexor Digitorum Superficialis (FDS) Transfer
The FDS transfer provides excellent strength and excursion. The critical biomechanical step in this transfer is routing the tendon to provide the correct vector for thumb extension and abduction.
Surgical Steps for FDS Transfer:
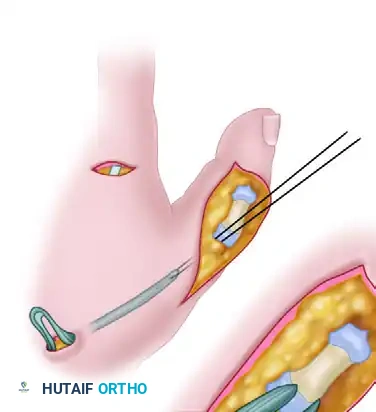
1. Harvest: Make a transverse incision at the palmar base of the ring finger. Identify the FDS tendon and release it just proximal to Camper's chiasm, preserving the FDP.
2. Proximal Delivery: Make a short longitudinal incision over the palmar aspect of the wrist, just proximal to the distal wrist flexion crease. Identify the ring FDS tendon and deliver it into this proximal wound.
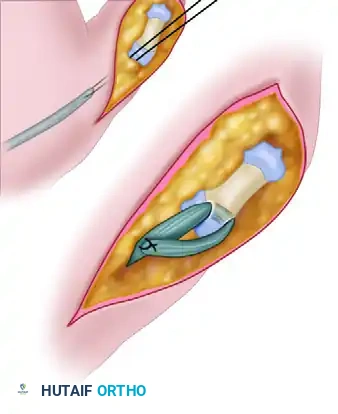
3. Routing: This is the most critical step. Reroute the FDS tendon subcutaneously around the radial border of the wrist. It must be passed deep to the abductor pollicis longus (APL) tendon. The APL acts as a biological pulley, preventing dorsal bowstringing and ensuring the transfer vector promotes both extension and abduction.
4. Distal Fixation: Suture the transferred FDS into the remnants of the EPL at the level of the distal phalanx. If no distal tendon remnant exists to accept the transfer, elevate a robust periosteal flap on the dorsal base of the distal phalanx and anchor the tendon directly to the bone using suture anchors or transosseous sutures.
Postoperative Care and Rehabilitation Protocol
The success of a tendon transfer in pediatric congenital hand surgery relies heavily on strict adherence to postoperative immobilization protocols. The repaired tissues require prolonged protection to prevent attenuation or rupture.
- Weeks 0 to 6: The patient remains in the initial postoperative long-arm cast or rigid plaster splint. The transarticular K-wire remains in place to mechanically offload the tendon repair.
- Week 6: The patient is taken to the clinic (or operating room, depending on age and compliance) for K-wire removal. The incisions are inspected.
- Weeks 6 to 14 (Months 1.5 to 3.5): Following K-wire removal, the hand is immediately placed back into a rigid plaster or fiberglass cast for an additional 2 months. This prolonged immobilization is necessary because pediatric patients cannot reliably comply with protective movement protocols.
- Months 3.5 to 7.5: The rigid cast is transitioned to a custom-molded, removable thermoplastic thumb spica splint. This support must be worn continuously (except for hygiene and supervised therapy) for approximately 4 additional months.
- After 7.5 Months: Unrestricted activity is gradually allowed, guided by occupational therapy to encourage active use of the newly transferred tendon in daily grasp and pinch activities.
Hypoplastic Hands and Digits
Moving beyond isolated tendon deficiencies, pediatric orthopedic surgeons frequently encounter broader developmental anomalies categorized as hypoplastic hands or digits.
Definition and Classification
Hypoplastic hands or digits are defined as anatomical parts in which embryological development is defective, arrested, or incomplete. While elements of hypoplasia (such as underdevelopment of skin, nerves, or vessels) are seen in almost all congenital hand deformities (e.g., syndactyly, radial clubhand), the specific term "hypoplasia" in this context is best reserved for fingers and hands exhibiting a relatively symmetrical deficiency of the part without severe associated angular deformity.
Epidemiology
Based on the landmark Iowa series of congenital hand anomalies:
* Hypoplasia of the entire hand: Accounts for approximately 0.8% of all congenital hand deformities.
* Brachydactyly (Short Fingers): Accounts for 5.2% of deformities, making it a relatively common presentation in the pediatric hand clinic.
Anatomical Variations
- Brachyphalangia (or Brachymesophalangia): This is the most common hypoplastic bony segment. It involves the shortening or underdevelopment of the middle phalanx. It usually occurs as an isolated anomaly but can be associated with similar shortening in the toes.
- Brachymetacarpia (Short Metacarpal): This condition involves a shortened metacarpal bone. It is extremely rare to diagnose in infancy or early childhood. Because the metacarpal physes close later, this discrepancy usually does not become clinically obvious until after the adolescent growth spurt, presenting as a "dropped knuckle" (often the 4th or 5th ray).
Genetics and Inheritance
Brachydactyly holds a unique place in the history of medical genetics; it was the very first example of Mendelian inheritance demonstrated in humans.
- Inheritance Pattern: Shortening of the fingers is classically considered an autosomal dominant trait.
- Transmission Risk: If an individual with autosomal dominant brachydactyly marries an individual without the anomaly, their offspring have a 50% chance of inheriting the condition.
- Sporadic Cases: While familial inheritance is common, sporadic de novo mutations do occur frequently, and in many isolated cases, no specific causative environmental or genetic factor can be definitively identified.
Syndromic Associations
While brachyphalangia frequently occurs as an isolated, benign cosmetic difference requiring no surgical intervention, shortening of the middle phalanges is a hallmark feature in numerous complex malformation syndromes. A thorough pediatric and genetic evaluation is mandatory when hypoplastic digits are accompanied by other systemic findings.
Notable syndromic associations include:
* Poland Syndrome: Characterized by unilateral symbrachydactyly (short, webbed fingers) associated with ipsilateral absence or hypoplasia of the sternocostal head of the pectoralis major muscle.
* Holt-Oram Syndrome: An autosomal dominant condition featuring upper limb anomalies (ranging from hypoplastic thumbs to severe radial longitudinal deficiency) paired with congenital heart defects (most commonly atrial septal defects).
* Treacher Collins Syndrome: A mandibulofacial dysostosis that can occasionally present with minor distal limb hypoplasia.
* Cornelia de Lange Syndrome: Characterized by severe developmental delay, distinct facial features, and upper limb reduction defects ranging from brachydactyly to oligodactyly.
* Silver-Russell Syndrome: Presents with intrauterine growth restriction, hemihypertrophy, and clinodactyly/brachydactyly of the fifth digit.
* Bloom Syndrome: A rare chromosomal instability disorder featuring pre- and postnatal growth deficiency, sun-sensitive skin changes, and mild limb hypoplasias.
Clinical Management of Hypoplastic Digits
Unlike the Group 2 clasped thumb, which requires aggressive surgical reconstruction to prevent severe functional deficit, isolated hypoplastic digits (brachydactyly) rarely require surgical lengthening or reconstruction. The functional impairment is usually minimal, and the risks of complex bone lengthening (distraction osteogenesis) or microvascular toe-to-hand transfers outweigh the cosmetic benefits. Surgery is generally reserved for cases where hypoplasia is combined with syndactyly (requiring web space release) or severe thumb hypoplasia (requiring pollicization to restore opposition).
You Might Also Like
