Comprehensive Surgical Anatomy & Biomechanics of the Shoulder Girdle
Key Takeaway
The shoulder girdle's surgical anatomy comprises the scapula, clavicle, and proximal humerus, forming four articulations. A deep understanding of its intricate osteology, biomechanics, and epidemiology is paramount for orthopedic surgeons. This knowledge enables accurate diagnosis of pathologies like rotator cuff tears, facilitating effective treatment and optimal surgical outcomes.
Comprehensive Shoulder Anatomy: Every Detail of the Shoulder
Introduction & Epidemiology
The shoulder girdle represents the most mobile and inherently unstable joint complex in the human body, facilitating a vast range of upper extremity functions. Its intricate design, involving three bony components (scapula, clavicle, proximal humerus) and four distinct articulations (glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic), necessitates a profound understanding of its anatomy and biomechanics for any orthopedic surgeon. Pathologies of the shoulder are exceedingly common, spanning traumatic injuries, degenerative conditions, and inflammatory processes. Fractures of the clavicle and proximal humerus are among the most frequent upper extremity fractures, particularly in specific age demographics. Rotator cuff tears represent a significant burden, with prevalence increasing with age, affecting a substantial portion of the population over 60. Glenohumeral instability, ranging from subluxation to recurrent dislocation, often impacts younger, active individuals. A meticulous grasp of the shoulder's structural and functional characteristics is paramount for accurate diagnosis, effective treatment planning, and optimal surgical outcomes.
Surgical Anatomy & Biomechanics
Osteology
The bony architecture of the shoulder girdle provides the framework for motion, muscle attachment, and articulation.
Scapula
The scapula, a flat, triangular bone, spans approximately the second through seventh ribs, serving as an attachment site for 17 muscles, a testament to its critical role in shoulder kinematics. Its intricate morphology includes the body, spine, acromion, coracoid process, and glenoid.
*
Scapular Body:
The body lies anteverted on the chest wall approximately 30 degrees relative to the coronal plane, a crucial orientation for glenohumeral articulation. The medial border provides attachment for the rhomboids and serratus anterior, while the lateral border is associated with the teres minor and long head of triceps. The supraspinous fossa and infraspinous fossa are origins for their respective rotator cuff muscles.
*
Glenoid:
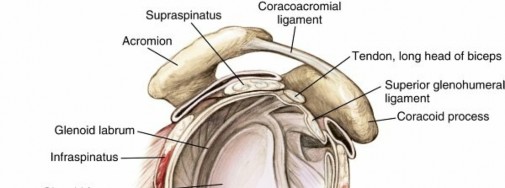
The glenoid fossa, a shallow, pear-shaped articular surface, articulates with the humeral head. It is typically retroverted approximately 5 degrees relative to the scapular body axis and superiorly tilted 5-7 degrees. The glenoid labrum, a fibrocartilaginous ring, deepens the socket by approximately 50%, enhancing glenohumeral stability and serving as an attachment point for the glenohumeral ligaments and the long head of the biceps tendon.
*
Acromion:
The acromion is a lateral projection of the scapular spine, forming the roof of the glenohumeral joint. Its morphology (Type I: flat, Type II: curved, Type III: hooked) has been implicated in subacromial impingement syndrome.
*
Os acromiale:
This condition represents an incomplete fusion of secondary ossification centers of the acromion, most commonly between the mesoacromion and metaacromion. While often asymptomatic, symptomatic os acromiale can mimic impingement and predispose to rotator cuff tears due to motion at the synchondrosis.
*

*
Coracoid Process:
This anterior projection from the superior border of the scapula is a vital attachment site for numerous soft tissue structures. Attachments to the coracoid include:
* The coracoacromial ligament, forming the superior aspect of the coracoacromial arch.
* The coracoclavicular ligaments (conoid [medial] and trapezoid [lateral]), critical for acromioclavicular joint stability.
* The conjoined tendon, comprising the short head of the biceps and the coracobrachialis.
* The pectoralis minor muscle.
*

*
Suprascapular Notch:
Located on the superior border of the scapula, medial to the coracoid process. The suprascapular artery passes superior to the superior transverse scapular ligament, while the suprascapular nerve passes inferior to the ligament, through the notch (mnemonic: “Army over Navy” for artery over nerve). This anatomical arrangement is crucial for understanding suprascapular nerve entrapment pathology.
*

*
Spinoglenoid Notch:
Located distal to the base of the scapular spine, at its junction with the glenoid neck. Both the suprascapular artery and nerve pass inferior to the inferior transverse scapular ligament through this notch. Entrapment here can lead to isolated infraspinatus atrophy.
Clavicle
The clavicle is the first bone in the body to ossify (at approximately 5 weeks’ gestation) and the last to fuse (medial epiphysis at 25 years of age). Its S-shape provides a strut connecting the upper extremity to the axial skeleton, protecting underlying neurovascular structures. Fracture of the clavicle is the most common musculoskeletal birth injury.
*
Articulations:
Medially, it articulates with the manubrium at the sternoclavicular joint; laterally, it articulates with the acromion at the acromioclavicular joint.
*
Muscle Attachments:
The clavicle provides origins for the deltoid and pectoralis major and insertions for the sternocleidomastoid and trapezius. The subclavian muscle attaches inferiorly.
*
Neurovascular Protection:
The clavicle overlies the subclavian artery and vein and the brachial plexus, making fractures with significant displacement a concern for neurovascular compromise, particularly with inferior displacement.
*

Proximal Humerus
The proximal humerus consists of the head, anatomical neck, surgical neck, greater tuberosity, lesser tuberosity, and bicipital groove.
*
Humeral Head:
The articular surface, covered with hyaline cartilage, typically has an inclination of approximately 130 degrees relative to the humeral shaft and 30 degrees of retroversion relative to the epicondylar axis.
*
Anatomical Neck:
Lies just distal to the articular margin of the humeral head.
*
Surgical Neck:
Located distal to the tuberosities, it is a common site for fractures due to its relative weakness. The axillary nerve and posterior circumflex humeral artery closely wrap around the surgical neck, making them vulnerable in fracture or surgical intervention.
*
Greater Tuberosity:
Contains three facets for the insertions of the supraspinatus (superior), infraspinatus (middle), and teres minor (inferior) rotator cuff tendons.
*
Lesser Tuberosity:
The insertion site for the subscapularis tendon.
*
Bicipital Groove (Intertubercular Sulcus):
Located between the greater and lesser tuberosities, it houses the long head of the biceps tendon, which is retained by the transverse humeral ligament.
*
Vascular Supply:
The arterial supply to the humeral head is primarily derived from the ascending branch of the anterior circumflex humeral artery (arcuate artery) and posteromedial vessels from the posterior circumflex humeral artery. Understanding these vessels is critical in the management of proximal humerus fractures to minimize the risk of avascular necrosis.
Arthrology
Glenohumeral (GH) Joint:
A true diarthrodial ball-and-socket joint, renowned for its extensive range of motion at the expense of inherent stability.
*
Capsule and Ligaments:
The joint capsule is relatively lax, particularly inferiorly (axillary recess), allowing for substantial motion. The glenohumeral ligaments (superior, middle, inferior) reinforce the anterior capsule and are crucial for static stability.
*
Superior Glenohumeral Ligament (SGHL):
Resists inferior translation and external rotation in adduction.
*
Middle Glenohumeral Ligament (MGHL):
Resists anterior translation and external rotation in 0-45 degrees of abduction.
*
Inferior Glenohumeral Ligament (IGHLC):
The most robust, consisting of an anterior band (ABIGHL), posterior band (PBIGHL), and an intervening axillary pouch. The ABIGHL is the primary restraint to anterior translation and external rotation in abducted positions (90 degrees). Lesions to the ABIGHL (Bankart lesion) are a hallmark of anterior instability. A HAGL (Humeral Avulsion of the Glenohumeral Ligament) lesion involves avulsion of the IGHLC from its humeral attachment.
*

*
Rotator Interval:
A triangular space between the supraspinatus and subscapularis tendons, superiorly bordered by the coracoid process. It contains the SGHL, MGHL, and the coracohumeral ligament (CHL), and provides passage for the long head of the biceps tendon. Its integrity is important for stability, especially against inferior subluxation in adduction.
Acromioclavicular (AC) Joint:
A planar synovial joint providing slight motion during shoulder girdle movement.
*
Ligaments:
Stabilized by the superior and inferior AC ligaments and, more importantly, by the coracoclavicular (CC) ligaments (conoid and trapezoid).
*
Conoid Ligament:
Medial and cone-shaped, resisting superior and posterior clavicular displacement.
*
Trapezoid Ligament:
Lateral and quadrilateral, resisting superior and anterior clavicular displacement.
* AC joint stability classification (Rockwood) relies heavily on the integrity of these ligaments.
*

Sternoclavicular (SC) Joint:
A saddle-type synovial joint, it is the only true articulation between the upper extremity and the axial skeleton.
*
Ligaments:
Reinforced by the anterior and posterior sternoclavicular ligaments, interclavicular ligament, and the costoclavicular ligament. An intra-articular disc enhances congruity and acts as a shock absorber.
*

Scapulothoracic Articulation: Not a true anatomical joint but a physiological articulation between the scapula and the posterior thoracic cage, separated by two muscle layers (subscapularis, serratus anterior). Crucial for scapulohumeral rhythm.
Myology
Rotator Cuff Muscles:
The dynamic stabilizers of the glenohumeral joint, comprising four muscles.
*
Supraspinatus:
Originates from the supraspinous fossa, inserts on the superior facet of the greater tuberosity. Initiates abduction. Innervated by the suprascapular nerve.
*
Infraspinatus:
Originates from the infraspinous fossa, inserts on the middle facet of the greater tuberosity. External rotation. Innervated by the suprascapular nerve.
*
Teres Minor:
Originates from the lateral border of the scapula, inserts on the inferior facet of the greater tuberosity. External rotation. Innervated by the axillary nerve.
*
Subscapularis:
Originates from the subscapular fossa, inserts on the lesser tuberosity. Internal rotation. Innervated by the upper and lower subscapular nerves.
* The combined action of the rotator cuff muscles depresses and compresses the humeral head into the glenoid, countering the superior pull of the deltoid, thus facilitating smooth glenohumeral motion.
*

Deltoid:
The primary mover of the shoulder, comprising three distinct heads.
*
Origin:
Lateral third of the clavicle (anterior), acromion (middle), and scapular spine (posterior).
*
Insertion:
Deltoid tuberosity on the lateral aspect of the humerus.
*
Actions:
Anterior (flexion, internal rotation), Middle (abduction), Posterior (extension, external rotation).
*
Innervation:
Axillary nerve. The deltoid-splitting approach commonly used in shoulder surgery must respect the axillary nerve, which runs approximately 5-7 cm distal to the acromial tip.
Biceps Brachii:
*
Long Head:
Originates from the supraglenoid tubercle, courses through the joint capsule and bicipital groove, and distally combines with the short head.
*
Short Head:
Originates from the coracoid process (conjoined tendon).
*
Actions:
Flexion of the elbow, supination of the forearm; also contributes to shoulder flexion.
Other Significant Muscles:
*
Pectoralis Major:
Clavicular and sternal heads, inserts on the lateral lip of the bicipital groove. Adduction, internal rotation, flexion.
*
Latissimus Dorsi and Teres Major:
Insert into the floor of the bicipital groove. Adduction, internal rotation, extension.
*
Trapezius:
Elevates, retracts, depresses, and rotates the scapula. Innervated by the accessory nerve (CN XI).
*
Serratus Anterior:
Originates from the first eight ribs, inserts on the medial border of the scapula. Protracts and rotates the scapula, preventing "winging." Innervated by the long thoracic nerve.
*
Rhomboids (Major and Minor):
Retract and elevate the scapula.
*
Levator Scapulae:
Elevates the scapula.
Neurovascular Anatomy
Nerves:
*
Brachial Plexus:
Formed by ventral rami of C5-T1, it gives rise to all major nerves of the upper extremity.
*
Axillary Nerve (C5, C6):
Originates from the posterior cord. Travels through the quadrangular space (bounded by teres minor superiorly, teres major inferiorly, long head of triceps medially, surgical neck of humerus laterally), innervating the deltoid and teres minor. Vulnerable during anterior shoulder dislocation and proximal humerus fractures.
*
Suprascapular Nerve (C5, C6):
From the upper trunk. Passes through the suprascapular notch ("Army over Navy") and then the spinoglenoid notch. Innervates supraspinatus and infraspinatus.
*
Long Thoracic Nerve (C5, C6, C7):
Originates directly from nerve roots. Runs on the superficial aspect of the serratus anterior. Injury causes scapular winging.
*
Musculocutaneous Nerve (C5, C6, C7):
From the lateral cord. Pierces the coracobrachialis, innervates biceps and coracobrachialis.
*
Upper and Lower Subscapular Nerves (C5, C6):
Innervate the subscapularis. The lower subscapular nerve also innervates the teres major.
*
Medial and Lateral Pectoral Nerves (C5-T1):
Innervate pectoralis major and minor.
*
Dorsal Scapular Nerve (C5):
Innervates rhomboids and levator scapulae.
*
Thoracodorsal Nerve (C6, C7, C8):
From the posterior cord. Innervates latissimus dorsi.
Arteries:
*
Subclavian Artery:
Becomes the axillary artery after passing the lateral border of the first rib.
*
Axillary Artery:
Gives off several branches relevant to the shoulder:
*
Thoracoacromial Artery:
Supplies the deltoid, pectoralis, acromion, and clavicle. The acromial branch of the thoracoacromial artery runs on the medial aspect of the coracoacromial ligament.
*
Anterior and Posterior Circumflex Humeral Arteries:
Encircle the surgical neck of the humerus. The anterior branch ascends to supply the humeral head (arcuate artery), vital for head viability. The posterior branch, larger, travels with the axillary nerve through the quadrangular space.
*
Subscapular Artery:
Gives rise to the circumflex scapular artery (through triangular space) and the thoracodorsal artery (supplying latissimus dorsi).
Biomechanics
The shoulder’s exceptional range of motion is achieved through a delicate balance between mobility and stability, facilitated by a complex interplay of passive stabilizers (capsule, ligaments, labrum) and active stabilizers (rotator cuff, deltoid, periscapular muscles).
*
Scapulohumeral Rhythm:
The coordinated movement between the glenohumeral joint and the scapulothoracic articulation. For every 3 degrees of abduction, 2 degrees occur at the GH joint and 1 degree at the ST articulation, especially after the initial 30 degrees. This rhythm optimally positions the glenoid for humeral head articulation and maintains muscle length-tension relationships.
*
Force Couples:
Crucial for efficient motion and stability.
*
Deltoid-Rotator Cuff Force Couple:
The deltoid provides an upward translation force on the humeral head. The rotator cuff muscles (especially subscapularis, infraspinatus, teres minor) provide a compressive force and a downward translation vector, centering the humeral head in the glenoid during abduction.
*
Scapular Force Couples:
Upper trapezius, serratus anterior, and lower trapezius work synergistically to upwardly rotate and stabilize the scapula during arm elevation.
*
Coracoacromial Ligament:
Contributes to anterosuperior stability, particularly in rotator cuff deficiency. Its preservation with irreparable cuff tears is advocated to prevent anterosuperior escape of the humeral head.
Indications & Contraindications
Surgical intervention in the shoulder is typically considered after failed conservative management or for conditions with clear surgical superiority.
Operative Indications
-
Trauma:
- Displaced clavicle fractures (especially midshaft, >2cm shortening, Z-fragment, skin tenting, neurovascular compromise).
- Displaced proximal humerus fractures (Neer 2-, 3-, 4-part fractures, head-splitting fractures, fracture-dislocations).
- Displaced scapular fractures (glenoid, neck, acromion affecting RC function).
- Acromioclavicular joint dislocations (Rockwood Type III-VI, symptomatic Type II).
- Sternoclavicular joint dislocations (posterior dislocations due to mediastinal compression).
-
Rotator Cuff Pathology:
- Full-thickness rotator cuff tears (acute, symptomatic chronic, symptomatic partial-thickness >50%).
- Massive irreparable rotator cuff tears (indicated for superior capsule reconstruction, reverse total shoulder arthroplasty, or palliative measures).
-
Glenohumeral Instability:
- Recurrent anterior, posterior, or multidirectional instability unresponsive to rehabilitation.
- Significant bony defects (e.g., glenoid bone loss >20-25%, large Hill-Sachs lesions) or specific lesions (Bankart, HAGL).
-
Degenerative Conditions:
- Symptomatic glenohumeral osteoarthritis (primary, post-traumatic, cuff tear arthropathy) unresponsive to non-operative treatment.
- Symptomatic acromioclavicular joint arthritis.
-
Biceps Pathology:
- Symptomatic superior labrum anterior-posterior (SLAP) tears (Type II, IV).
- Refractory biceps tendinopathy or subluxation.
-
Other:
- Refractory subacromial impingement syndrome.
- Adhesive capsulitis unresponsive to manipulation under anesthesia.
- Tumors involving the shoulder girdle.
Contraindications
-
Absolute:
- Active infection (local or systemic).
- Severe, uncorrectable medical comorbidities precluding anesthesia or surgical tolerance.
- Skeletally immature patients for certain procedures (e.g., arthroplasty).
-
Relative:
- Uncontrolled diabetes, hypertension, or other systemic diseases.
- Non-compliance with rehabilitation protocols.
- Poor soft tissue envelope or skin conditions precluding safe incision.
- Significant smoking history (increases complication rates).
- Advanced age with significant functional limitations, where surgical risk outweighs potential benefit.
Operative vs. Non-Operative Indications
| Condition | Operative Indications | Non-Operative Indications |
|---|---|---|
| Clavicle Fracture | Displaced midshaft fracture (>2cm shortening, Z-fragment, neurovascular compromise, open fracture), lateral clavicle fracture (Type II), medial clavicle fracture (posterior displacement). | Non-displaced/minimally displaced midshaft fractures, non-displaced lateral (Type I, III, IV) and medial clavicle fractures. |
| Proximal Humerus Fracture | Displaced 2-, 3-, 4-part fractures (surgical neck, tuberosity displacement >5mm, angulation >45 degrees), head-splitting fractures, fracture-dislocations (especially if irreducible). High-demand younger patients. | Non-displaced or minimally displaced fractures, stable 2-part surgical neck fractures in elderly, low-demand patients. |
| Rotator Cuff Tear | Symptomatic full-thickness tears (acute traumatic, chronic progressive), symptomatic partial-thickness tears (>50% tendon involvement, failed non-operative management), symptomatic retracted tears in younger, active patients. | Asymptomatic tears, small partial-thickness tears (<50% involvement), symptomatic tears responding to physical therapy, NSAIDs, injections. Low-demand elderly patients with chronic tears. |
| Glenohumeral Instability | Recurrent dislocations/subluxations unresponsive to rehabilitation, significant glenoid bone loss (>20-25%), large Hill-Sachs lesions (engaging), Bankart lesions, HAGL lesions, failed prior stabilization. | First-time dislocation (depending on age and risk factors), subluxation responding to physical therapy, isolated labral pathology without significant instability. |
| Glenohumeral Osteoarthritis | Severe, refractory pain and functional limitation, failed extensive non-operative management, significant radiographic changes (joint space narrowing, osteophytes, subchondral sclerosis/cysts). | Mild to moderate symptoms, early radiographic changes, managed with NSAIDs, activity modification, physical therapy, intra-articular injections. |
| Acromioclavicular (AC) Joint Injury | Rockwood Type III-VI (Type III often controversial; depends on patient demand and symptoms), symptomatic Type II if chronic pain/instability, distal clavicle osteolysis unresponsive to conservative care. | Rockwood Type I & II injuries, asymptomatic Type III, symptomatic Type III that responds to conservative management. |
| Biceps Tendon Pathology | Symptomatic SLAP tears (Type II, IV), chronic refractory biceps tendinopathy or instability of long head of biceps (often with rotator cuff pathology), Popeye deformity in younger, active patients (for tenodesis). | Type I SLAP tears, asymptomatic biceps tendinopathy, proximal biceps rupture in low-demand or elderly patients (often managed non-operatively). |
| Adhesive Capsulitis | Refractory stiffness and pain despite physical therapy, medication, and injections. Patients failing 3-6 months of conservative management considered for manipulation under anesthesia +/- arthroscopic capsular release. | Primary treatment: physical therapy, NSAIDs, oral corticosteroids, intra-articular injections (corticosteroids, distension). |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to optimize surgical outcomes and minimize complications.
Pre-Operative Planning
- Clinical Assessment: Comprehensive history focusing on mechanism of injury, pain characteristics, functional limitations, and prior treatments. Detailed physical examination, including range of motion, strength testing, stability assessment, and neurovascular status.
-
Imaging Review:
- Radiographs: AP, scapular Y, and axillary views are standard. Specific views like trauma series, Zanca view (AC joint), or Stryker notch view (Hill-Sachs) may be indicated.
- MRI: Essential for soft tissue evaluation (rotator cuff, labrum, capsule, biceps tendon, cartilage).
- CT Scan: Crucial for complex fractures (proximal humerus, scapula), glenoid bone loss assessment (instability), and pre-operative templating for arthroplasty. 3D reconstructions are invaluable.
-

- Surgical Strategy: Define the approach, required instrumentation, fixation implants, and potential contingencies. For arthroplasty, templating is performed using radiographs and CT to determine component size, version, and inclination.
- Anesthesia Consultation: Assess patient's medical fitness, discuss pain management strategies (e.g., interscalene block), and potential risks.
- Antibiotic Prophylaxis: Administer pre-operatively according to institutional guidelines.
Patient Positioning
The two primary positions for shoulder surgery are beach chair and lateral decubitus.
-
Beach Chair Position:
- Setup: Patient is semi-recumbent (30-70 degrees of trunk elevation). Head supported in a headrest (e.g., "donut") with attention to cervical lordosis and adequate padding to prevent pressure injuries. Torso strapped securely to the table. Operative arm is free-draped or placed on an arm board. Non-operative arm padded and tucked or placed on an arm board.
- Advantages: Allows for easy conversion to open surgery if needed, provides a familiar anatomical orientation for surgeons, and allows for both anterior and posterior access. Reduced risk of traction-related brachial plexopathy.
- Disadvantages: Risk of cerebral hypoperfusion (especially in hypotensive patients), potential for airway issues if head is flexed excessively, increased venous pooling in lower extremities.
- Neurovascular Precautions: Ensure head and neck are neutral to prevent brachial plexus stretch. Confirm blood pressure monitoring (often at the brain level) is adequate.
-

-
Lateral Decubitus Position:
- Setup: Patient lies on their side with the non-operative arm abducted and suspended overhead on an arm rest. The operative shoulder is elevated using a beanbag positioner. The operative arm is placed in a traction device, often with a sterile stockinette and finger traps, providing controlled longitudinal traction and variable abduction/flexion. Axillary roll positioned under the non-operative axilla to prevent neurovascular compression. Head and neck neutral.
- Advantages: Excellent visualization of posterior and inferior aspects of the glenohumeral joint, gravity aids in fluid egress from the joint, allows for traction to facilitate glenohumeral distraction.
- Disadvantages: Risk of brachial plexus injury from excessive traction, potential for injury to the non-operative arm, more complex setup for open conversion.
- Neurovascular Precautions: Limit traction weight (<10-15 lbs for extended periods), ensure axillary roll is correctly placed, periodically check radial pulse and monitor nerve function.
Detailed Surgical Approach / Technique
Surgical approaches to the shoulder are dictated by the pathology and required exposure. Here, we outline general principles and common approaches for illustrative procedures.
Arthroscopic Rotator Cuff Repair (Example: Supraspinatus Repair)
Patient Positioning:
Beach chair or lateral decubitus.
Portals:
1.
Posterior Portal (Standard):
1-2 cm inferior and 1 cm medial to the posterior-lateral corner of the acromion. This is the primary viewing portal.
2.
Anterior Portal:
Established under direct visualization from the posterior portal, typically anterior to the biceps tendon, slightly lateral to the coracoid. Used for instrumentation.
3.
Lateral Portals (Working Portals):
Created 3-5 cm lateral to the acromial edge, typically in line with the anterior, middle, and posterior deltoid fibers. Used for anchor placement and suture management.
*

Technique:
1.
Diagnostic Arthroscopy:
Systematically evaluate the glenohumeral joint (biceps tendon, labrum, glenoid, humeral head, capsule, cartilage). Assess the rotator cuff tear size, retraction, and tissue quality.
2.
Bursectomy and Debridement:
Remove inflamed subacromial bursa and debride frayed rotator cuff tissue to facilitate visualization and promote healing.
3.
Acromioplasty (if indicated):
Resect osteophytes and undersurface bone from the acromion to create space for the cuff.
4.
Cuff Mobilization:
Release adhesions and assess tear pattern. Ensure adequate mobilization to achieve tension-free repair.
5.
Footprint Preparation:
Debride the greater tuberosity footprint to bleeding cancellous bone using a burr, creating a raw bed for tendon-to-bone healing.
6.
Anchor Placement:
Place suture anchors (bioabsorbable or titanium) into the prepared footprint on the greater tuberosity.
*
Single Row:
Anchors placed laterally, sutures passed through the tendon and tied.
*
Double Row:
Medial row anchors compress the tendon to the footprint, and a lateral row of anchors or transosseous sutures compress the tendon more broadly.
*
Suture Bridge:
Medial row sutures are passed through the tendon, then tied to lateral row anchors, creating a broad compression zone.
7.
Suture Management and Knot Tying:
Pass sutures through the tendon in appropriate configurations (e.g., simple, mattress, modified Mason-Allen) and tie using arthroscopic knot-tying techniques, ensuring secure approximation of the tendon to the bone.
8.
Final Assessment:
Confirm stable repair, inspect for any remaining loose bodies or pathology.
Open Reduction Internal Fixation (ORIF) of Proximal Humerus Fracture (Example: Deltopectoral Approach)
Patient Positioning:
Beach chair position.
Approach:
Deltopectoral interval.
1.
Incision:
A longitudinal incision from the coracoid process inferiorly, extending 8-12 cm distally along the deltopectoral groove.
2.
Interval Dissection:
Identify the cephalic vein in the deltopectoral groove. It is typically retracted laterally with the deltoid, but can be retracted medially with the pectoralis major for better exposure.
3.
Deep Dissection:
Retract the deltoid laterally and the pectoralis major medially. The clavipectoral fascia is incised. The coracobrachialis and short head of the biceps are retracted medially.
4.
Exposure of Humeral Head:
Identify and protect the neurovascular structures. The axillary nerve enters the deltoid approximately 5-7 cm distal to the acromial edge and must be protected during retraction and plate application. The anterior circumflex humeral artery runs deep in this interval.
5.
Hematoma Evacuation:
Carefully evacuate fracture hematoma to visualize fracture fragments.
6.
Reduction:
Restore anatomical alignment of the humeral head, tuberosities, and shaft. Provisional fixation with K-wires or reduction clamps. Avoid excessive stripping of periosteum to preserve blood supply.
7.
Plate Application:
A precontoured locking plate (e.g., PHILOS plate) is typically used. Position the plate on the lateral aspect of the humerus, ensuring proper height relative to the rotator cuff insertion.
8.
Screw Fixation:
Insert locking screws into the humeral head and cortical screws into the shaft. Ensure screws do not violate the articular surface; confirm with intraoperative fluoroscopy.
9.
Rotator Cuff Suture (if indicated):
For tuberosity fractures, non-absorbable sutures can be passed through the rotator cuff tendons and into the plate to enhance stability.
10.
Closure:
Close in layers, ensuring meticulous hemostasis.
Latarjet Procedure for Glenohumeral Instability (Coracoid Transfer)
Patient Positioning:
Beach chair position.
Approach:
Deltopectoral interval.
1.
Incision and Deltopectoral Dissection:
As described for ORIF, expose the coracoid process.
2.
Coracoid Osteotomy:
Isolate the coracoid process. Identify and protect the musculocutaneous nerve, which typically enters the conjoined tendon 2-5 cm distal to the coracoid tip. Perform an osteotomy of the coracoid process approximately 1.5 cm from its tip, ensuring the conjoined tendon remains attached to the transferred bone block.
3.
Subscapularis Split:
Split the subscapularis tendon longitudinally in line with its fibers, typically between its upper 2/3 and lower 1/3, creating access to the anterior glenoid.
4.
Glenoid Preparation:
Identify the anterior glenoid rim. Debride the capsule and labrum from the anterior glenoid neck to prepare a bleeding surface for coracoid block apposition.
5.
Coracoid Transfer:
Position the transferred coracoid block flush against the anterior aspect of the glenoid neck. The undersurface of the coracoid faces the glenoid, with the conjoined tendon positioned inferomedially.
6.
Fixation:
Secure the coracoid block to the glenoid neck, typically with two cancellous screws. Ensure precise positioning and compression. The transferred conjoined tendon also contributes to stability by acting as an inferior "sling."
7.
Capsular Closure:
Close the capsule and subscapularis tendon over the transferred coracoid block, creating a robust anterior repair.
8.
Layered Closure:
Standard layered closure.
Complications & Management
Complications associated with shoulder surgery can range from minor issues to devastating outcomes, underscoring the importance of meticulous technique and vigilant post-operative care.
General Surgical Complications
-
Infection:
Superficial wound infection (cellulitis) or deep prosthetic joint infection (PJI) / osteomyelitis.
- Incidence: PJI 0.5-2% in arthroplasty; lower in arthroscopy.
- Management: Superficial infections: oral antibiotics. Deep infections: surgical debridement and irrigation (DAIR), prolonged IV antibiotics, possible 2-stage revision arthroplasty.
-
Neurovascular Injury:
Damage to brachial plexus, axillary nerve, musculocutaneous nerve, suprascapular nerve, or vascular structures.
- Incidence: Nerve injury 1-5% (transient neurapraxia more common).
- Management: Protection during surgery (meticulous dissection, careful retraction), intraoperative nerve monitoring. Post-op: observation for neurapraxia, electrodiagnostic studies, nerve repair/grafting if transection.
-
Bleeding/Hematoma:
Can lead to increased pain, swelling, and risk of infection.
- Incidence: Variable, often minor.
- Management: Meticulous hemostasis intraoperatively, drains if indicated. Evacuation for large, symptomatic hematomas.
-
Stiffness/Arthrofibrosis:
Restricted range of motion.
- Incidence: Up to 20% in some series.
- Management: Aggressive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions.
-
Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: Low in shoulder surgery, but potentially fatal.
- Management: Prophylaxis (mechanical, chemical if high risk), early mobilization.
Procedure-Specific Complications
| Complication | Incidence | Salvage Strategy / Management |
|---|---|---|
| Rotator Cuff Reteard | 10-30% | Revision rotator cuff repair (if reparable), superior capsule reconstruction, latissimus dorsi transfer, reverse total shoulder arthroplasty (for massive irreparable tears with pseudoparalysis). |
| Recurrent Instability (post-stabilization) | 5-15% (arthroscopic Bankart) | Revision stabilization (arthroscopic or open), Latarjet procedure (for bone loss), capsular shift, revision arthroscopy with emphasis on bony augmentation or deeper capsular plication. |
| Nonunion/Malunion (fracture fixation) | 5-15% (proximal humerus) | Revision ORIF with bone grafting, conversion to hemiarthroplasty or total shoulder arthroplasty (for proximal humerus nonunion with significant deformity and symptoms), corrective osteotomy. |
| Avascular Necrosis (AVN) of Humeral Head (post-fracture/ORIF) | 5-20% (especially 3-4 part fractures) | Hemiarthroplasty or total shoulder arthroplasty (standard or reverse), depending on patient age, cuff integrity, and glenoid status. |
| Hardware Complications (e.g., screw cutout, plate impingement) | Variable (5-20%) | Hardware removal, revision fixation, conversion to arthroplasty, management of subsequent rotator cuff tears. |
| Glenoid Erosion/Loosening (arthroplasty) | 10-20% (anatomic TSA) | Revision total shoulder arthroplasty (often to reverse TSA), glenoid bone grafting, or accepting progression (for mild, asymptomatic cases). |
| Scapular Notching (reverse TSA) | Up to 70% | Lateralizing glenoid baseplate, inferior glenosphere overhang; if symptomatic, soft tissue release, rarely revision. |
| Frozen Shoulder (post-surgery) | 5-10% | Aggressive physical therapy, intra-articular steroid injection, manipulation under anesthesia, arthroscopic capsular release. |
| Painful Arc Syndrome / Impingement (post-AC joint surgery) | Variable | Non-operative management, subacromial decompression (if secondary impingement), hardware removal (if irritating), revision AC joint reconstruction. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgery itself for achieving optimal functional outcomes. Protocols are tailored to the specific procedure, patient factors (age, tissue quality, co-morbidities), and surgeon preference, but generally follow a phased approach.
General Principles
- Pain Management: Multimodal approach including nerve blocks, oral analgesics, and cryotherapy.
- Protection of Repair: Initial immobilization with sling/brace to protect surgical repair.
- Progressive Mobilization: Gradually advance range of motion (ROM) and strengthening, respecting tissue healing timelines.
- Patient Education: Emphasize adherence to protocol and precautions.
Phased Rehabilitation Approach
Phase I: Protection (0-6 weeks post-op)
*
Goals:
Protect surgical repair, minimize pain and inflammation, prevent stiffness (without compromising repair).
*
Immobilization:
Sling or brace (e.g., abduction sling for rotator cuff repair) worn continuously, removed only for hygiene and exercises.
*
Motion:
*
Passive Range of Motion (PROM):
Pendulum exercises, gentle external rotation (0-30 degrees depending on repair), passive elevation (0-90 degrees depending on repair/fracture stability), performed with assistance or by therapist.
*
Elbow, Wrist, Hand AROM:
Encourage to prevent stiffness.
*
Strengthening:
None for the operative shoulder. Isometric scapular squeezes (avoiding glenohumeral motion).
*
Precautions:
Avoid active lifting, reaching, weight-bearing on the affected arm. Avoid active internal rotation past neutral for subscapularis repairs.
Phase II: Early Motion & Controlled Active Motion (6-12 weeks post-op)
*
Goals:
Gradually restore active ROM, initiate light strengthening, normalize scapular mechanics.
*
Immobilization:
Wean off sling typically by 6 weeks.
*
Motion:
*
Active-Assistive Range of Motion (AAROM):
Using contralateral limb or pulley system to increase ROM.
*
Active Range of Motion (AROM):
Progressively increase AROM in all planes as pain allows and repair integrity permits.
*
Strengthening:
*
Isometric Exercises:
Progress to gentle isometrics for rotator cuff and deltoid.
*
Light Resistance Exercises:
Begin with elastic bands or light weights for periscapular muscles (scapular retraction, depression), external/internal rotators, deltoid.
*
Precautions:
Avoid heavy lifting, sudden movements, pushing/pulling, excessive overhead activity.
Phase III: Progressive Strengthening & Return to Activity (12-24+ weeks post-op)
*
Goals:
Restore full strength, power, endurance, and sport-specific function.
*
Motion:
Achieve full, pain-free AROM.
*
Strengthening:
*
Progressive Resistance Exercises:
Increase intensity and resistance for all shoulder girdle muscles.
*
Neuromuscular Control:
Proprioceptive exercises, dynamic stability drills.
*
Plyometrics:
For overhead athletes, introduce sport-specific plyometric training.
*
Functional Training:
Gradually incorporate activities of daily living and work- or sport-specific movements.
*
Return to Activity:
Gradual return to light activity at 4-6 months, full activity/sport-specific drills 6-12 months, depending on the procedure and individual progress. Objective strength and functional testing should guide return to play.
Summary of Key Literature / Guidelines
The field of orthopedic shoulder surgery is continuously evolving, driven by ongoing research and refinement of techniques. Key literature and guidelines provide evidence-based recommendations for diagnosis and management.
- Rotator Cuff Repair: Numerous studies have focused on optimizing repair techniques (single vs. double row, suture bridge), biologics (PRP, stem cells), and rehabilitation protocols. The landmark systematic reviews by Mazzocca et al. (2007) and Levine et al. (2014) have influenced decision-making regarding repair constructs. AAOS Clinical Practice Guidelines provide evidence-based recommendations on rotator cuff tear evaluation and treatment.
- Glenohumeral Instability: The ITR (Instability Tendon Reconstruction) score and ISIS (Instability Severity Index Score) are important clinical tools for predicting failure rates after arthroscopic Bankart repair, guiding decisions towards open stabilization or bony augmentation (e.g., Latarjet). The work of Burkhart (2004) emphasized the concept of "glenoid track" and its implications for Hill-Sachs engagement.
- Proximal Humerus Fractures: Consensus remains challenging for complex fractures. The Neer classification is widely used, though its interobserver reliability is debated. Studies like PROximal Fracture of the Humerus: A Multi-Centre Evaluation (PROFHER) trial (2015) have provided robust evidence on non-operative versus operative management for displaced proximal humerus fractures in the elderly, suggesting non-operative treatment often yields similar outcomes to surgery. However, operative management remains crucial for specific fracture patterns and younger, active patients.
- Shoulder Arthroplasty: Advances in implant design and surgical technique for total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (rTSA) have significantly improved outcomes for glenohumeral arthritis. Frankel et al. (2008) described the optimal glenoid position in rTSA to minimize scapular notching. Long-term registries and meta-analyses provide data on implant longevity, complication rates, and functional improvements.
- AC Joint Injuries: The Rockwood classification remains the standard. Debate continues regarding the optimal management of Rockwood Type III injuries, with recent evidence favoring conservative management in many cases, especially for low-demand patients. Surgical techniques for high-grade injuries (Type IV-VI) emphasize anatomical reduction and robust stabilization of the coracoclavicular ligaments.
Continuous engagement with the current literature and adherence to evidence-based guidelines are paramount for orthopedic surgeons managing shoulder pathologies, ensuring the highest standard of care for our patients.
Clinical & Radiographic Imaging



You Might Also Like


