Surgical Management of Insertional and Noninsertional Achilles Tendinopathy: A Comprehensive Operative Guide
Key Takeaway
Surgical management of Achilles tendinopathy requires a precise understanding of pathoanatomy, distinguishing between insertional disease and noninsertional tendinosis. Operative intervention is indicated following six months of failed conservative therapy. Techniques range from retrocalcaneal bursectomy and calcaneal exostectomy to extensive tendon débridement and flexor hallucis longus (FHL) transfer, depending on the extent of tendon degeneration and the presence of gastrocsoleus contracture.
INTRODUCTION TO ACHILLES TENDINOPATHY
Achilles tendinopathy represents a spectrum of debilitating conditions that frequently challenge orthopedic surgeons, sports medicine physicians, and rehabilitation specialists. The pathology is broadly categorized anatomically into two distinct clinical entities: insertional Achilles tendon disease and chronic noninsertional Achilles tendinosis. Each presents with unique biomechanical derangements, pathoanatomy, and therapeutic requirements.
Insertional disease typically involves a triad of pathology at the enthesis: insertional tendinosis, retrocalcaneal bursitis, and a prominent posterosuperior calcaneal tuberosity (Haglund’s deformity). Conversely, noninsertional tendinosis occurs in the "watershed" region of the tendon—approximately 2 to 6 cm proximal to the calcaneal insertion—where relative hypovascularity predisposes the tissue to microtrauma, mucoid degeneration, and failed healing responses.
When conservative measures—such as eccentric loading protocols, orthoses, and judicious biologic injections—fail after a minimum of six months, surgical intervention becomes indicated. This guide provides an exhaustive, step-by-step masterclass on the operative management of both insertional and noninsertional Achilles tendinopathy, tailored for the postgraduate orthopedic surgeon.
PART I: DÉBRIDEMENT OF THE TENDON FOR INSERTIONAL ACHILLES TENDON DISEASE
Insertional Achilles tendinopathy is characterized by degenerative changes at the tendon-bone interface, often exacerbated by mechanical impingement from a Haglund’s deformity during ankle dorsiflexion. Surgical intervention aims to decompress the retrocalcaneal space, excise degenerative tendon tissue, and restore the mechanical integrity of the gastrocsoleus-calcaneal complex.
Preoperative Planning and Anesthesia
Thorough preoperative clinical and radiographic evaluation is mandatory. Weight-bearing lateral radiographs of the ankle are essential to assess the morphology of the calcaneal tuberosity (e.g., parallel pitch lines, Fowler-Philip angle) and to identify intratendinous calcifications or enthesophytes. Magnetic Resonance Imaging (MRI) is highly recommended to quantify the percentage of tendon degeneration, which directly dictates whether a primary repair is feasible or if a tendon transfer will be required.
Surgical Pearl: Anesthetic Considerations
Place the patient in the prone position after the adequate administration of a general anesthetic. If preoperative imaging and clinical assessment determine that a tendon transfer (e.g., Flexor Hallucis Longus) is not necessary, the procedure can be performed satisfactorily under regional anesthesia. A comprehensive local block must target the sural nerve, the tibial nerve, and the medial calcaneal nerve branches to ensure complete regional anesthesia and optimal postoperative pain control.
Surgical Approaches
The choice of surgical approach depends on the extent of the disease, the presence of central tendon calcifications, and the surgeon's preference regarding cosmetic and functional outcomes.
-
Lateral Longitudinal Approach:
Make a longitudinal incision approximately 1 cm lateral to the lateral border of the Achilles tendon. The incision should extend from 3 to 4 cm proximal to the superior calcaneal tuberosity down to 2 to 3 cm distal to the superior tuberosity of the calcaneus. This approach provides excellent visualization of the retrocalcaneal bursa and the lateral aspect of the Haglund’s prominence while avoiding the sural nerve, provided dissection remains strictly within the safe zone. -
Central Splitting Approach (Johnson et al.):
Alternatively, a central tendon-splitting approach can be utilized. As described by Johnson et al., this midline longitudinal incision directly bisects the Achilles tendon. It offers direct, unparalleled access to central intratendinous calcifications and the central aspect of the posterosuperior calcaneal prominence. Furthermore, it has been reported to yield superior cosmetic results and minimizes the risk of injury to the sural nerve laterally and the neurovascular bundle medially.
Operative Technique: Step-by-Step Débridement and Exostectomy
The following steps detail the standard operative sequence for retrocalcaneal decompression and tendon débridement.
-
Paratenon Dissection and Tendon Relaxation:
Carefully incise the paratenon in line with the skin incision. Preserve the paratenon flaps for meticulous closure, as this highly vascularized layer is critical for postoperative tendon healing and preventing skin adhesions. Plantar flex the ankle to relax the gastrocsoleus complex, reducing tension on the Achilles insertion. -
Exposure of the Retrocalcaneal Space:
Retract the Achilles tendon posteriorly (or retract the split halves medially and laterally if using the central approach). This maneuver exposes the inflamed retrocalcaneal bursa and the offending bony prominence of the posterosuperior calcaneus. -
Bursectomy and Calcaneal Exostectomy:
Aggressively excise the hypertrophic retrocalcaneal bursa using a rongeur. Once the bursa is cleared, the Haglund’s deformity is fully visualized. Use a ½-inch osteotome or an oscillating saw to resect the posterosuperior bony prominence.
🚨 Surgical Pitfall: Inadequate Bone Resection
The most common error in this procedure is not resecting enough bone. Failure to adequately decompress the retrocalcaneal space leads to persistent mechanical impingement and recurrent symptoms. A generous, oblique resection of the posterosuperior tuberosity must be accomplished, ensuring that no bony impingement occurs even in maximum ankle dorsiflexion.
-
Tendon Débridement:
If necessary, elevate the Achilles tendon from its insertion for approximately 1 cm to access the deep, anterior fibers. Meticulously excise any diseased, mucoid, or necrotic segments of the tendon. All osteophytes and calcific deposits within the central aspect of the tendon must be completely removed to prevent persistent pain. -
Management of Gastrocsoleus Contracture:
After thorough débridement of the tendon, excision of the retrocalcaneal bursa, and resection of the Haglund deformity, assess the resting tension of the ankle. If a substantial preoperative gastrocsoleus contracture is still present (evidenced by an inability to achieve neutral dorsiflexion with the knee extended), an Achilles tendon lengthening or gastrocnemius recession may be indicated. - Technique: Perform the lengthening in the coronal plane and repair it with interrupted nonabsorbable polyethylene sutures.
-
Indication Note: This lengthening is performed primarily in more elderly, sedentary patients with severe, chronic insertional calcaneal tendinitis where contracture is a primary pain generator.
-
Alternative: Complete Detachment and Reattachment:
In cases of severe, diffuse insertional calcification where >50% of the tendon must be debrided, complete detachment of the Achilles tendon may be required. Following complete exostectomy and débridement, perform a V-Y lengthening of the proximal aponeurosis if length is lost. Reattach the healthy tendon to the calcaneal footprint using robust suture anchors in a double-row configuration to maximize the footprint contact area and biomechanical strength.
Postoperative Care Protocol
Successful outcomes rely heavily on strict adherence to a phased postoperative rehabilitation protocol to protect the repair while preventing stiffness.
- Weeks 0–3: A non–weight-bearing (NWB) short leg cast is applied in the operating room with the ankle in slight plantar flexion (10° to 20°) to minimize tension on the repair.
- Weeks 3–6: The patient is transitioned to a weight-bearing (WB) cast or a rigid controlled ankle motion (CAM) boot locked in slight plantar flexion. Weight-bearing is advanced as tolerated.
- Weeks 6–12: At the end of 6 weeks, a prefabricated walking boot is applied with progressive reduction of heel wedges to slowly stretch the tendon to neutral. The patient may begin active and passive range-of-motion (ROM) exercises and gentle, progressive calf strengthening.
- Months 3+: At 3 months, the boot is discontinued. A silicone heel lift is used in standard footwear to reduce peak insertional forces, and the patient is allowed to return gradually to previous activities and sports based on functional testing.
PART II: CHRONIC NONINSERTIONAL ACHILLES TENDINOSIS
Noninsertional Achilles disorders occur proximal to the calcaneal insertion and are driven by repetitive microtrauma in a zone of relative hypovascularity. The pathology is characterized by a failed healing response, angiofibroblastic hyperplasia, and mucoid degeneration rather than acute inflammatory infiltrates.
Classification and Clinical Evaluation
Noninsertional disorders are clinically and histologically divided into three distinct types:
- Peritendinitis: Involves inflammation primarily of the paratenon and peritendinous structures. The tendon substance itself remains normal.
- Peritendinitis with Tendinosis: Involves both inflammation of the paratenon and underlying degenerative changes within the Achilles tendon substance.
- Tendinosis: Typically asymptomatic in its early stages, this involves intrasubstance swelling, mucoid degeneration, and collagen disorganization without significant paratenon inflammation.
Clinical Examination:
Clinical examination is highly useful in differentiating between these disorders.
* Chronic Tendinosis: Presents as a relatively nontender condition involving a palpable, bulbous nodularity within the tendon substance. Crucially, this nodule moves proximally and distally with passive flexion and extension of the ankle.
* Peritendinitis: May or may not involve underlying tendinosis, but the hallmark is that the area of maximal tenderness remains static; it does not move with ankle flexion and extension, as the inflammation is localized to the surrounding paratenon sheath.

Figure 82-73: Bulbous nodularity in a patient with chronic noninsertional Achilles tendinosis. Note the localized fusiform swelling characteristic of intrasubstance mucoid degeneration.
Imaging and Preoperative Counseling
While the diagnosis is primarily clinical, imaging plays a critical role in surgical planning.
* Radiographs: Chronic degenerative tendinosis may produce dystrophic calcification that is visible on lateral standing radiographs.
* MRI: Magnetic Resonance Imaging is the gold standard for evaluating the extent of intrasubstance degenerative changes. It is indispensable for preoperative counseling.
Surgical Pearl: The 50% Rule
If MRI reveals that substantially more than 50% of the tendon cross-sectional area shows severe degenerative changes, primary débridement and tubularization will likely fail due to insufficient remaining healthy collagen. In these cases, a detailed discussion with the patient regarding the necessity of a tendon transfer (e.g., FHL transfer) must be conducted preoperatively.
Conservative Management and the Role of Biologics
Conservative measures must be exhausted before considering surgical intervention. A strict, compliant trial of nonoperative management should be attempted for no less than 6 months. The cornerstone of conservative treatment is a heavy-load eccentric strengthening program (e.g., the Alfredson protocol), which stimulates collagen remodeling and improves tendon tensile strength.
The Controversy of Biologic Injections:
There has been considerable interest in alternative injection therapies designed to address the pathological neovascularity associated with tendinosis (e.g., high-volume image-guided injections or sclerosing agents) or to introduce growth factors via platelet-rich plasma (PRP) concentrates into the diseased portion of the tendon.
Although the biological principles of delivering autologous growth factors seem sound, the clinical studies remain inconclusive. In a landmark randomized controlled trial, de Vos et al. demonstrated that a platelet-rich plasma injection did not result in statistically significant improvement in pain and activity scores when compared to a saline placebo injection. These results strongly indicate that the clinical effectiveness observed in these cohorts is driven primarily by the concurrent eccentric strengthening rehabilitation rather than any apparent additional benefit of the platelet-rich plasma injection itself.
Surgical Intervention: Débridement and Tendon Transfer
When conservative management fails, or in patients presenting with extensive disease on clinical examination and MRI, surgical intervention is warranted.
1. Simple Débridement and Tubularization:
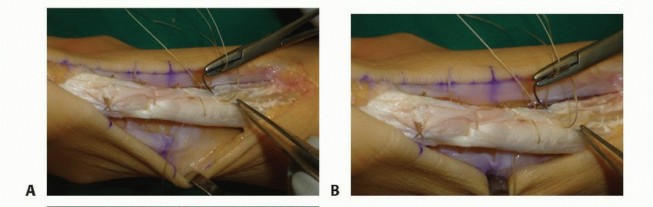
For localized tendinosis involving less than 50% of the tendon, a longitudinal tenotomy is performed. The degenerative, fibrotic, and mucoid tissue is sharply excised. The remaining healthy tendon is then tubularized using absorbable sutures to restore a cylindrical morphology, and the paratenon is meticulously closed to prevent adhesions.
2. Flexor Hallucis Longus (FHL) Transfer:
Patients with extensive disease (>50% tendon involvement on MRI), older patients with poor tissue quality, or those for whom previous surgical treatment has failed are prime candidates for a flexor hallucis longus (FHL) transfer.
Rationale for FHL Transfer: The FHL is the procedure of choice in this group—as opposed to complete detachment and primary repair—due to its robust vascular muscle belly, which brings a new blood supply to the hypovascular watershed region. Furthermore, the FHL is an "in-phase" muscle that fires synergistically with the gastrocsoleus complex during the push-off phase of gait, making neuromuscular re-education seamless. Its axis of pull is directly aligned with the Achilles, providing excellent biomechanical substitution.
Clinical Evidence: The efficacy of FHL transfer in severe Achilles tendinopathy is well-documented. Martin et al. reported highly successful outcomes in a cohort of older, challenging patients. In their study, they noted significantly decreased pain and improved functional scores in 42 of 44 patients (average age 58 years) who were treated with complete excision of the diseased Achilles tendon and reconstruction via transfer of the flexor hallucis longus tendon.
FHL Transfer Technique Overview:
* The FHL tendon is harvested either via a single-incision posterior approach (harvesting at the level of the fibro-osseous tunnel of the posterior talus) or a double-incision technique (with a second medial midfoot incision for maximum length).
* The diseased Achilles tendon is aggressively debrided or completely excised.
* A bone tunnel is drilled into the superior calcaneal tuberosity, anterior to the Achilles footprint.
* The FHL tendon is routed through the bone tunnel and secured using a bioabsorbable interference screw, ensuring the ankle is held in slight plantar flexion to set the appropriate resting tension.
* The remaining native Achilles stump is sutured to the FHL tendon to augment the repair and utilize the FHL muscle belly for local vascularization.
Conclusion
The surgical management of Achilles tendinopathy demands a nuanced understanding of the underlying pathoanatomy. Insertional disease requires aggressive bony decompression and retrocalcaneal bursectomy, with careful attention to avoiding the under-resection of the Haglund's deformity. Noninsertional tendinosis requires a careful assessment of tendon viability; while localized disease responds well to simple débridement, extensive degeneration necessitates the robust biomechanical and biological augmentation provided by an FHL transfer. Strict adherence to phased postoperative rehabilitation is universally required to optimize functional outcomes and return patients to their desired activity levels.
You Might Also Like