Achilles Tendon Disorders: Comprehensive Surgical Management
Key Takeaway
Achilles tendon disorders present significant clinical challenges, requiring a nuanced understanding of biomechanics and vascular anatomy. Management ranges from eccentric strengthening and topical glyceryl trinitrate to complex surgical interventions. This guide details the pathophysiology, differential diagnosis, and step-by-step surgical techniques—including retrocalcaneal exostectomy and flexor hallucis longus transfer—for treating both insertional and noninsertional Achilles tendinopathy in the orthopedic patient.
ACHILLES TENDON DISORDERS: PATHOPHYSIOLOGY AND MANAGEMENT
Few conditions in the realm of foot and ankle surgery are as notoriously frustrating to treat—both conservatively and surgically—as Achilles tendon disorders. Achieving a successful clinical outcome demands an extreme degree of patience, meticulous surgical execution, and strict adherence to postoperative rehabilitation protocols on the part of both the surgeon and the patient.
Anatomy and Biomechanics
The Achilles tendon is the largest, thickest, and most powerful tendon in the human body. It is formed from the confluence of fibers from two distinct muscle units comprising the triceps surae:
* The Gastrocnemius Muscle: A biarticular muscle originating above the knee joint from the posterior aspect of the medial and lateral femoral condyles. It is most biomechanically effective in plantar flexion of the ankle when the knee is fully extended.
* The Soleus Muscle: A uniarticular muscle originating from the upper posterior tibia, fibula, and the intervening interosseous membrane. It is the primary plantar flexor of the ankle when the knee is flexed.
As the conjoined tendon courses distally through the superficial posterior compartment of the calf, its fibers undergo a complex 90-degree lateral rotation before inserting into the calcaneal tuberosity. Consequently, the gastrocnemius fibers insert laterally, while the soleus fibers insert medially. This spiral configuration allows for elongation and elastic recoil, storing kinetic energy during the gait cycle.
Vascularity and the "Watershed" Zone
Vascular supply to the Achilles tendon is derived from three primary sources:
1. Proximal: Musculotendinous arterial branches within the gastrocnemius-soleus complex.
2. Distal: Small interosseous vessels at the osteotendinous insertion into the calcaneus.
3. Extrinsic: The paratenon, a highly vascularized sheath enveloping the deep and superficial surfaces of the tendon.
Crucially, angiographic studies demonstrate a zone of relative avascularity—the "watershed area"—located 2 to 6 cm proximal to the calcaneal insertion. While this marginal blood supply is sufficient for low-demand physiological states, increased mechanical demand from repetitive microtrauma or overuse can outstrip the vascular supply. This ischemic environment precipitates mucoid degeneration, fibrosis, and ultimately, tendinosis. Once this degenerative cascade initiates, the poor local perfusion dictates a highly prolonged tissue recovery phase.
Classification and Risk Factors
Chronic Achilles tendon disorders are broadly classified based on anatomic location:
1. Insertional Tendinopathy: Occurs at the osteotendinous junction. It is frequently associated with a prominent posterosuperior calcaneal exostosis (Haglund deformity or "pump bump"), retrocalcaneal bursitis, and intratendinous calcification.
2. Noninsertional Tendinopathy: Occurs 2 to 6 cm proximal to the insertion within the watershed zone. It presents as tendinosis (intrasubstance degeneration) with or without peritendinitis (inflammation of the paratenon).
Clinical Pearl: Holmes and Lin identified significant systemic risk factors for Achilles tendinopathy. In both sexes, obesity and hypertension strongly correlate with tendinosis. In women, oral contraceptive use is a significant risk factor, whereas diabetes mellitus shows a statistical association primarily in men younger than 44 years.
DIFFERENTIAL DIAGNOSIS
A meticulous clinical examination is required to differentiate Achilles tendinopathy from other posterior ankle pathologies. The differential diagnosis includes:
* Posterior tibial tendinitis or tendinosis
* Flexor hallucis longus (FHL) tendinitis (often seen in dancers)
* Peroneal tendinopathy
* Posterior ankle impingement syndrome (with or without a symptomatic os trigonum or enlarged trigonal process)
* Posterior subtalar or tibiotalar arthritis
* Sciatica or S1 radiculopathy
* Exertional compartment syndrome of the deep posterior calf
* Tarsal tunnel syndrome
Systemic Considerations: Achilles enthesopathy may be the initial manifestation of systemic inflammatory arthritides. While seropositive conditions like rheumatoid arthritis or systemic lupus erythematosus can be culprits, seronegative spondyloarthropathies—such as Reiter syndrome (reactive arthritis), ankylosing spondylitis, and psoriatic arthritis—are far more commonly associated with bilateral or recalcitrant insertional Achilles pain.
NONOPERATIVE MANAGEMENT
The difficulty in managing Achilles tendinopathy nonsurgically has spawned a myriad of treatment modalities. A 2001 Cochrane Database Systematic Review by McLauchlan and Handoll found no single nonsurgical strategy to be universally superior; however, modern evidence supports a multimodal approach.
Evidence-Based Conservative Modalities
- Eccentric Loading Programs: The cornerstone of nonoperative treatment. An eccentric strengthening program for the gastrocnemius-soleus complex (e.g., the Alfredson protocol), combined with aggressive stretching, stimulates collagen realignment and tendon hypertrophy.
- Orthoses and Immobilization: The use of an ankle-foot orthosis (AFO) night splint helps prevent overnight equinus contracture. In acute flares, a brief period of immobilization in a short leg walking cast or controlled ankle motion (CAM) boot is highly effective.
- Topical Glyceryl Trinitrate (GTN): Hunte, Lloyd-Smith, and Paoloni et al. demonstrated that topical GTN patches significantly outperform placebos in managing noninsertional Achilles tendinosis at 12 to 24 weeks. Nitric oxide release is theorized to stimulate fibroblast proliferation and collagen synthesis. This is a routine adjunct in modern conservative protocols.
- Extracorporeal Shock Wave Therapy (ESWT): The literature remains contradictory. Furia concluded that ESWT is effective for chronic insertional tendinopathy (noting that local field block anesthesia may blunt its efficacy), whereas Costa et al. found no support for its use. It remains an option for refractory cases before surgery.
- Injections: Corticosteroid injections into the tendon substance are strictly contraindicated due to the high risk of iatrogenic rupture. Sclerosing injections (e.g., polidocanol) targeting neovascularization have shown promise in European studies, but widespread validation remains elusive.
Despite aggressive conservative management, approximately 35% of patients will fail to obtain relief and will require surgical intervention. Maffulli et al. noted that surgical outcomes for chronic Achilles tendinopathy are generally less satisfactory in sedentary individuals compared to age-matched athletic cohorts.
INSERTIONAL ACHILLES TENDINITIS
Insertional tendinitis is a complex triad characterized by:
1. Haglund Deformity: A prominent exostosis on the posterosuperior aspect of the calcaneal tuberosity.
2. Retrocalcaneal Bursitis: Inflammation of the bursa that normally lubricates the space between the anterior aspect of the Achilles tendon and the calcaneus.
3. Intratendinous Degeneration: Inflammatory or degenerative changes within the tendon insertion, frequently accompanied by dystrophic ossification or calcific spurring.
Clinical Diagnosis
Patients rarely report an acute traumatic event. The presentation is typically a slow, insidious onset of pain and gradual enlargement at the tendon insertion. Hallmark symptoms include progressive difficulty wearing closed-back shoes due to direct pressure, and severe "start-up" pain upon arising in the morning or after periods of rest.
On physical examination, direct palpation elicits exquisite tenderness over the retrocalcaneal bursa (just anterior to the tendon insertion) or centrally over the tendon itself. In severe cases, the tendon appears boggy, thickened, and clinically prominent. A significant equinus contracture of the gastrocnemius-soleus complex is frequently observed, particularly with the knee extended (Silfverskiöld test).
Radiographic Evaluation
Standard weight-bearing radiographs of the foot and ankle are mandatory. A standing lateral view of the heel is critical for evaluating the presence of intratendinous calcific spurs, the morphology of the posterosuperior calcaneal tuberosity (Haglund prominence), and the Fowler-Philip angle. Magnetic Resonance Imaging (MRI) or high-resolution ultrasound is highly recommended for surgical planning to quantify the percentage of tendon degeneration.
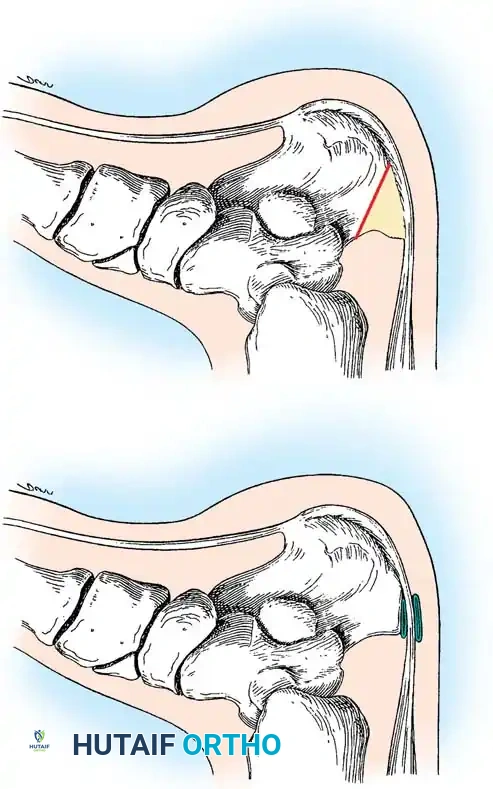
Fig. 85-47 A, Calcaneus with retrocalcaneal and superficial Achilles tendon bursae before ostectomy. B, Large portion of calcaneus needs to be removed or symptoms will recur. (From Frey C, Pfeffer GB: Surgical management of Haglund’s deformity.)
Surgical Decision Making: The 50% Rule
When conservative measures fail, surgical debridement is indicated. A critical intraoperative question is: How much tendon can be safely detached and resected before the risk of catastrophic rupture becomes unacceptable?
Anatomical studies by Kolodziej, Glisson, and Nunley mapped the Achilles insertion, finding an average height of 19.8 mm, a proximal width of 23.8 mm, and a distal width of 32.1 mm. Biomechanical testing revealed that up to 50% of the tendon insertion can be safely resected and detached from superior to inferior without compromising structural integrity. Calder and Saxby confirmed that if ≤50% of the tendon is resected, aggressive postoperative mobilization with immediate weight-bearing in a cast or boot is safe and effective. If >50% requires resection, tendon augmentation (e.g., FHL transfer) is mandatory.
SURGICAL TECHNIQUE 85-18: Retrocalcaneal Exostectomy and Tendon Debridement
The following technique utilizes a lateral approach, which avoids the medial neurovascular bundle and provides excellent access to the Haglund prominence. Alternatively, if MRI demonstrates primarily central intratendinous calcification, a midline posterior incision with a central tendon-splitting approach (as described by McGarvey et al. and Johnson et al.) is highly effective.
🔪 Surgical Technique 85-18: Step-by-Step
1. Positioning and Anesthesia
* Place the patient in the prone position after the administration of general or regional anesthesia.
* If a tendon transfer is not anticipated, local anesthesia with intravenous sedation can be utilized. Ensure a comprehensive block of the sural nerve, tibial nerve, and medial calcaneal nerve branches.
* Apply a thigh tourniquet to ensure a bloodless surgical field. Place a bump under the distal tibia to allow the ankle to rest in a neutral to slightly plantar-flexed position.
2. Surgical Approach
* Make a longitudinal incision approximately 1 cm lateral to the lateral border of the Achilles tendon.
* Extend the incision from 3 to 4 cm proximal to the superior calcaneal tuberosity down to 2 to 3 cm distal to the superior tuberosity.
* Carefully dissect through the subcutaneous tissues, taking great care to identify and protect the sural nerve, which crosses the lateral border of the Achilles tendon proximally.
* Incise the paratenon longitudinally. Plantar flex the ankle to relieve tension on the tendon.
3. Exposure of the Pathology
* Retract the Achilles tendon posteriorly and medially. This maneuver exposes the inflamed retrocalcaneal bursa and the offending posterosuperior bony prominence (Haglund deformity).
* If the tendon is broadly attached over the exostosis, sharply elevate the anterior fibers of the Achilles tendon off the superior aspect of the calcaneus. Do not detach more than 50% of the medial-to-lateral width unless planning an augmentation.
4. Resection and Debridement
* Excise the hypertrophic retrocalcaneal bursa entirely using a rongeur.
* Utilize a 1/2-inch osteotome or an oscillating microsaw to resect the posterosuperior calcaneal prominence.
Surgical Pitfall: The most common cause of surgical failure is inadequate bone resection. A generous ostectomy must be performed. The resection should angle from posterosuperior to anteroinferior to ensure no impingement occurs when the ankle is maximally dorsiflexed.
* Debride the Achilles tendon. Excise any grossly degenerated, fibrotic, or mucinous segments. Remove all intratendinous osteophytes and calcifications.
5. Tendon Repair and Lengthening
* If a significant portion of the tendon was detached (but <50%), reattach it to the calcaneal footprint using suture anchors loaded with high-tensile nonabsorbable suture.
* Achilles Tendon Lengthening: If a substantial preoperative gastrocnemius-soleus contracture remains after debridement, a lengthening procedure is indicated. Perform a fractional lengthening of the gastrocnemius aponeurosis (Strayer or Baumann procedure) or a percutaneous triple hemisection (Hoke technique) in the coronal plane. Repair any paratenon defects with interrupted nonabsorbable polyethylene or absorbable sutures to prevent adhesions.
* Note: Lengthening is primarily reserved for elderly, sedentary patients with severe insertional Achilles tendinitis and rigid equinus.
6. Closure
* Thoroughly irrigate the wound.
* Close the paratenon meticulously, followed by subcutaneous tissue and skin. A layered closure is critical to prevent wound breakdown, a devastating complication in this avascular region.
Postoperative Rehabilitation (Technique 85-18)
- Weeks 0-3: The patient is placed in a non-weight-bearing (NWB) short leg cast in 10 to 15 degrees of plantar flexion to remove tension from the repair.
- Weeks 3-6: Transition to a weight-bearing cast or a rigid CAM boot with heel wedges. Progressive weight-bearing is initiated.
- Weeks 6-12: The cast is removed, and a prefabricated walking boot is utilized. The patient begins formal physical therapy focusing on active and passive range of motion (ROM) and gentle isometric calf strengthening.
- Month 3: Transition to regular footwear with a silicone heel lift. Eccentric strengthening is advanced. Return to high-impact sports is typically delayed until 6 to 9 months postoperatively.
ADVANCED RECONSTRUCTION: FLEXOR HALLUCIS LONGUS (FHL) TRANSFER
For patients with severe, end-stage insertional tendinopathy where >50% of the Achilles insertion requires debridement, isolated repair is insufficient. In these cases, augmentation with a Flexor Hallucis Longus (FHL) tendon transfer is the gold standard, particularly in elderly or obese patients.
Rationale for FHL Transfer
The FHL is the ideal transfer candidate because it is an in-phase synergist to the triceps surae, possesses a parallel axis of contractile pull, and is anatomically adjacent to the Achilles. Furthermore, the highly vascular FHL muscle belly brings a robust new blood supply to the avascular watershed zone of the Achilles, promoting biologic healing.
Surgical Considerations for FHL Transfer
- Debridement: The entire diseased section of the Achilles tendon is excised. If the entire insertion is compromised, it is completely detached and debrided.
- Harvest: The FHL is harvested. While a single-incision posterior harvest yields sufficient length for most weaves, a double-incision technique (adding a medial midfoot incision) provides maximum length.
- Fixation: The harvested FHL tendon is passed through a bone tunnel drilled into the calcaneal tuberosity and secured with an interference screw or tied over a bone bridge.
- Weave: The proximal stump of the FHL is then woven through the remaining native Achilles tendon (Pulvertaft weave) to retain the resting tension and power of the gastrocnemius-soleus complex.
Outcomes: Morbidity from FHL harvest (e.g., weakness of great toe flexion) is clinically insignificant for most patients, as demonstrated by Coull et al. Martin et al. reported a 95% decrease in pain and an 86% patient satisfaction rate following FHL transfer for severe Achilles tendinopathy. While isokinetic strength deficits are measurable, functional strength is excellent, with nearly all patients able to perform a single-leg heel raise postoperatively.
CHRONIC NONINSERTIONAL ACHILLES TENDINOSIS
Noninsertional disorders occur in the watershed zone and require a different diagnostic and therapeutic approach. Puddu et al. classified these into three distinct entities:
1. Peritendinitis: Inflammation strictly confined to the paratenon and peritendinous structures. The tendon substance is normal.
2. Peritendinitis with Tendinosis: Inflammation of the paratenon combined with intrasubstance degenerative changes.
3. Tendinosis: Pure intrasubstance mucoid degeneration. This is often asymptomatic until a critical threshold is reached, presenting as a painless, palpable nodule.
Clinical Examination Pearls
Differentiating between peritendinitis and tendinosis is achieved through the Royal London Hospital Test:
* In tendinosis, the palpable bulbous nodularity is located within the tendon substance. When the patient actively dorsiflexes and plantar flexes the ankle, the nodule moves with the tendon.
* In peritendinitis, the inflammation is in the surrounding sheath. The area of maximal tenderness remains stationary during ankle range of motion.
Surgical Management of Noninsertional Tendinosis
Surgical intervention is indicated after 6 months of failed conservative therapy. MRI is invaluable for preoperative counseling; if >50% of the tendon cross-section demonstrates severe mucinous degeneration, the patient must be consented for a possible FHL transfer.
The surgical approach involves a longitudinal incision over the medial border of the tendon (avoiding the laterally based sural nerve). The paratenon is stripped (paratenonectomy) to denervate the pain fibers and remove fibrotic adhesions. Multiple longitudinal tenotomies are performed parallel to the tendon fibers. This technique excises the degenerative, fibrotic nodules and stimulates a localized inflammatory healing response, promoting neovascularization and the influx of pluripotent fibroblasts to remodel the tendon. Postoperative rehabilitation mirrors that of insertional debridement, with a heavy emphasis on early, protected range of motion to prevent paratenon adhesions.
📚 Medical References
- Achilles tendon disorders with fl exor hallucis longus tendon transfer/augmentation, Foot Ankle Int 21:1004, 2000.
- Wong MW, Ng VW: Modifi ed fl exor hallucis longus transfer for Achilles insertional rupture in elderly patients, Clin Orthop 431:201, 2005.
- Woolnough J: Tennis heel, Med J Aust 2:857, 1954.
- Yodlowski ML, Scheller AD Jr, Minos L: Surgical treatment of Achilles tendinitis by decompression of the retrocalcaneal bursa and the superior calcaneal tuberosity, Am J Sports Med 30:318, 2002.
You Might Also Like

