Adductor Longus Tenotomy: An Intraoperative Masterclass for Chronic Groin Pain

Key Takeaway
This masterclass details adductor longus tenotomy for chronic groin pain in athletes. We cover essential surgical anatomy, meticulous preoperative planning, and a step-by-step intraoperative guide, emphasizing precise technique and nerve protection. Fellows will learn to navigate common pitfalls, manage complications, and guide patients through a structured postoperative rehabilitation program for optimal recovery and return to sport.
Comprehensive Introduction and Patho-Epidemiology
Chronic adductor-related groin pain represents one of the most recalcitrant and diagnostically challenging pathologies encountered in sports medicine and orthopaedic surgery. While acute adductor strains—typically occurring at the musculotendinous junction—are almost universally managed with non-operative protocols, chronic pain presenting as an isolated enthesopathy or in conjunction with athletic pubalgia can become profoundly debilitating. This condition frequently sidelines high-level athletes for extended periods, leading to significant frustration for both the patient and the treating clinician. When conservative measures such as targeted physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid or platelet-rich plasma (PRP) injections fail to provide durable relief, operative intervention via an adductor longus tenotomy becomes a highly effective, definitive solution.
The epidemiology of this condition is heavily skewed towards athletes participating in sports that demand powerful, ballistic movements, rapid changes of direction, and extreme ranges of hip motion. Soccer, ice hockey, rugby, fencing, and martial arts are the classic paradigms. In these activities, the athlete frequently transitions from trunk rotation with hip extension and abduction to sudden, explosive anterior trunk rotation coupled with hip flexion and adduction. A quintessential example is the biomechanics of a soccer player's in-step kick or the explosive stride of a hockey player. These kinetic chain actions generate immense shear forces across the anterior pelvic ring, specifically stressing the dynamic stabilizers of the pubic symphysis, primarily the lower abdominal musculature and the hip adductor complex.
The Pathogenesis of Adductor Enthesopathy
The pathogenesis of chronic adductor strains is complex, multifactorial, and deeply intertwined with the concept of the "sports hernia" or core muscle injury. It is now widely understood that the adductor longus does not function in isolation; rather, its proximal tendinous origin blends seamlessly with the distal insertion of the rectus abdominis over the anterior pubic symphysis, forming a contiguous aponeurotic plate. Chronic microtrauma to this region, driven by the repetitive eccentric loading inherent in multidirectional sports, leads to a degenerative cascade. This manifests histologically as angiofibroblastic hyperplasia, mucoid degeneration, and a disorganized collagen matrix at the enthesis—a true tendinosis rather than an acute inflammatory tendinitis.
Furthermore, many of these conditions are acute-on-chronic presentations. An athlete may harbor asymptomatic degenerative changes at the adductor origin for years before a specific, forceful eccentric contraction precipitates a partial tearing of the compromised tendon. While underlying pelvic instability—often termed "osteitis pubis"—has historically been implicated in the etiology of chronic groin pain, it remains difficult to definitively prove as a primary causative factor versus a secondary radiographic finding resulting from altered pelvic biomechanics. The primary objective of the adductor longus tenotomy is to surgically release this diseased, tensioned tissue, thereby altering the local biomechanical environment, alleviating traction on the highly innervated periosteum of the pubic tubercle, and allowing the muscle to heal in a functionally lengthened state.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the medial thigh and anterior pelvic anatomy is absolutely critical for the safe and effective execution of an adductor longus tenotomy. The adductor longus is a large, fan-shaped muscle that serves as the most anterior and superficial structure within the medial compartment of the thigh. Its origin is the pivotal landmark for our surgical approach: it arises via a strong, flat tendon from the anteromedial aspect of the superior pubic ramus, precisely inferior to the pubic tubercle and the pubic symphysis. From this proximal attachment, the muscle belly courses distally, laterally, and posteriorly to insert onto the middle third of the linea aspera of the posterior femur, blending with the medial intermuscular septum.
The Pubic Aponeurosis and Muscular Anomalies
The proximal anatomy is complicated by its intimate relationship with the abdominal wall. The anterior fibers of the adductor longus tendon interdigitate with the fascial expansions of the rectus abdominis and the external oblique aponeurosis. This structural continuity means that tension generated by the abdominal musculature is directly transmitted to the adductor origin, and vice versa. This biomechanical antagonism across the pubic symphysis is the primary driver of the "cleft sign" seen on MRI. Additionally, surgeons must be acutely aware of anatomical variants at the origin. A frequent and surgically relevant anomaly is the presence of direct muscular fibers forming the most lateral 5 to 11 millimeters of the anterior origin, bypassing the main tendinous structure. Failure to identify and transect these lateral muscular bands during a tenotomy will result in an incomplete release and persistent postoperative pain.
Neurovascular Relationships of the Medial Compartment
The neurovascular topography of the adductor compartment dictates the safety margins of the surgical dissection. The primary structure at risk during this procedure is the obturator nerve. Arising from the lumbar plexus (ventral rami of L2-L4), the obturator nerve descends through the psoas major, courses along the lateral pelvic wall, and exits the pelvis via the obturator canal. Upon exiting, it promptly divides into an anterior and a posterior branch, separated by the adductor brevis muscle.
The anterior division is of paramount concern during an adductor longus tenotomy. It descends anterior to the adductor brevis and posterior (deep) to the pectineus and adductor longus muscles. It provides motor innervation to the adductor longus, adductor brevis, and gracilis, and terminates as a cutaneous branch supplying the medial thigh. When performing the tenotomy, the surgeon must maintain the dissection plane strictly proximal and superficial. By executing the tenotomy approximately 1 to 1.5 centimeters distal to the pubic origin, and carefully placing a retractor deep to the adductor longus tendon but superficial to the adductor brevis, the anterior division of the obturator nerve is reliably protected. Vascularly, while the main femoral vessels are safely located lateral and superior to the operative field within the femoral triangle, the adductor compartment is richly supplied by branches of the obturator artery and the medial circumflex femoral artery. Meticulous hemostasis is required to prevent postoperative hematoma, which can lead to significant morbidity and delayed rehabilitation.
Exhaustive Indications and Contraindications
The decision to proceed with an adductor longus tenotomy must be predicated on a rigorous, systematic diagnostic workup. Because chronic groin pain frequently presents with a broad and overlapping differential diagnosis, isolated adductor enthesopathy must be definitively confirmed, and concomitant pathologies must be either ruled out or addressed concurrently. The hallmark clinical presentation includes insidious onset groin pain that is sharply exacerbated by resisted adduction and passive abduction. Patients will reliably demonstrate focal, exquisite tenderness to direct palpation over the adductor longus origin at the pubic tubercle.
The "Squeeze Test" is a critical provocative maneuver. It is performed with the patient supine, hips and knees flexed to 45 and 90 degrees respectively, while the patient forcefully adducts against the examiner's fist or a sphygmomanometer placed between the knees. A positive test elicits sharp pain at the pubic origin, often accompanied by a discernible strength deficit compared to the contralateral side. We grade this strength loss as mild, moderate, or severe. Surgical intervention is indicated when these clinical signs persist despite a minimum of 3 to 6 months of dedicated, high-quality non-operative management, including core stabilization exercises, eccentric adductor strengthening, and appropriate biologic or corticosteroid injections.
Differential Diagnosis and Exclusion Criteria
Before scheduling surgery, the orthopaedic surgeon must exhaustively exclude other etiologies of groin pain. The most common pitfall in adductor surgery is the failure to recognize a co-existing athletic pubalgia (sports hernia) or intra-articular hip pathology. If an athlete presents with concomitant lower abdominal pain, pain with a resisted sit-up, or a dilated superficial inguinal ring, a general surgery consultation is mandatory, as an isolated adductor tenotomy will fail to resolve the symptoms. Similarly, femoroacetabular impingement (FAI) and acetabular labral tears must be ruled out via specialized physical exam maneuvers (FADIR, FABER) and advanced imaging. Performing a tenotomy on a patient whose primary pain generator is an intra-articular hip lesion is a catastrophic diagnostic error.
| Category | Specific Criteria |
|---|---|
| Primary Indications | - Chronic, isolated adductor longus enthesopathy confirmed by MRI. - Failure of >3-6 months of comprehensive conservative management. - Focal tenderness at the adductor longus origin. - Positive, painful Squeeze Test with associated weakness. - Unacceptable decline in athletic performance due to pain. |
| Absolute Contraindications | - Active local or systemic infection. - Primary intra-articular hip pathology (e.g., severe osteoarthritis, symptomatic FAI) without addressing the hip first. - Isolated athletic pubalgia (sports hernia) without adductor involvement. - Inguinal or femoral hernia (requires general surgery intervention). |
| Relative Contraindications | - Significant psychiatric overlay or unrealistic postoperative expectations. - Severe, generalized pelvic floor dysfunction. - History of complex regional pain syndrome (CRPS) in the lower extremity. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for an adductor longus tenotomy is heavily reliant on advanced imaging to confirm the clinical diagnosis and map the precise extent of the pathology. Magnetic Resonance Imaging (MRI) of the pelvis without contrast is the gold standard modality. The imaging protocol must include fluid-sensitive sequences (T2-weighted STIR or fat-suppressed T2) in the axial, coronal, and sagittal planes, specifically tailored to the pubic symphysis.
The surgeon should meticulously review the MRI for several key pathologic hallmarks. Primary among these is high T2 signal intensity at the adductor longus musculotendinous junction or within the proximal tendon itself, indicative of tendinosis or partial tearing. Furthermore, the presence of a "secondary cleft sign"—a linear area of high T2 signal extending from the symphyseal joint into the adductor origin—is highly specific for microtearing of the rectus abdominis/adductor longus aponeurotic plate. Associated pubic bone marrow edema (osteitis pubis) is frequently observed; while not a primary diagnosis in this context, it serves as a strong corroborating indicator of chronic, abnormal stress across the anterior pelvic ring due to adductor pathology.
Patient Positioning and Operating Room Setup
Proper patient positioning is critical for optimal exposure, ease of dissection, and protection of neurovascular structures. The procedure is typically performed under general anesthesia, though regional anesthesia (spinal or epidural) combined with monitored anesthesia care (MAC) is a viable alternative depending on patient physiology and anesthesiologist preference.
- Table and Patient Orientation: The patient is placed strictly supine on a standard radiolucent operating table.
- Operative Extremity Positioning: The operative lower extremity is manipulated into a "frog-leg" or modified figure-of-four position. Specifically, the hip is flexed to approximately 45 degrees, abducted to 45 degrees, and maximally externally rotated.
- Biomechanical Rationale: This specific positioning is non-negotiable. It places the adductor longus muscle under maximal physiological stretch, rendering its proximal tendinous origin highly prominent, taut, and easily palpable beneath the subcutaneous fat. This tension facilitates precise incision placement and significantly eases the blunt dissection required to isolate the tendon from the underlying adductor brevis.
- Support and Draping: The limb is supported in this position using a padded leg holder, a customized foam ramp, or by a dedicated surgical assistant. Only the ipsilateral groin, hemipelvis, and medial thigh are prepped and draped in a standard sterile fashion. The draping should allow for dynamic manipulation of the leg during the procedure if necessary to adjust tension on the adductor complex.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an open adductor longus tenotomy demands meticulous tissue handling, precise plane identification, and a thorough respect for the regional neurovascular anatomy. The procedure is designed to completely release the tension on the diseased enthesis while minimizing collateral soft tissue trauma.
Incision Planning and Superficial Dissection
With the patient properly positioned and the adductor longus under tension, the surgeon begins by palpating the pubic tubercle. Moving immediately inferior and lateral to the tubercle, the firm, cord-like structure of the adductor longus origin is identified. A transverse or slightly oblique incision, measuring approximately 3 to 4 centimeters in length, is marked. This incision is placed roughly 1 to 2 centimeters inferior and parallel to the inguinal crease, centered directly over the palpable tendinous mass.
Following the skin incision with a #10 scalpel, superficial hemostasis is immediately achieved using bipolar electrocautery. The dissection proceeds through the subcutaneous fat and Scarpa's fascia. Small, self-retaining retractors (such as Weitlaner retractors) are placed to maintain exposure. The surgeon then encounters the deep investing fascia of the medial thigh compartment. Using a #15 blade or fine-tipped electrocautery, this fascial layer is incised longitudinally, parallel to the orientation of the adductor longus muscle fibers, directly exposing the pearlescent, proximal tendon.

Tendon Isolation and Protection of Deep Structures
Once the deep fascia is breached, blunt dissection becomes the primary technique. Using a combination of Metzenbaum scissors and a gloved index finger, the surgeon sweeps away the overlying loose areolar tissue to clearly define the medial and lateral borders of the adductor longus tendon. It is imperative at this stage to recall the anatomical anomaly discussed previously: the surgeon must actively search for and isolate the lateral muscular fibers that frequently bypass the main tendon to insert directly onto the pubis.
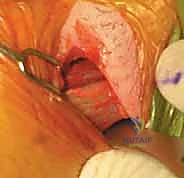
The most critical step of the procedure is the development of the plane between the adductor longus and the underlying adductor brevis. Using a blunt right-angle clamp or a smooth dissector, the surgeon carefully passes the instrument deep (posterior) to the adductor longus tendon, sweeping from medial to lateral. This maneuver elevates the tendon away from the adductor brevis. Once this plane is established, a blunt retractor—such as a small Army-Navy or a blunt Hohmann retractor—is placed beneath the adductor longus. This retractor serves a dual purpose: it places the tendon under isolated tension for the cut, and it acts as an impenetrable physical barrier, protecting the anterior division of the obturator nerve that lies draped across the anterior surface of the adductor brevis.

Executing the Tenotomy and Closure
With the tendon isolated and deep structures protected, the tenotomy is performed. The transection is made approximately 1 to 1.5 centimeters distal to the pubic attachment. Using bipolar electrocautery or a heavy Mayo scissor, the surgeon systematically divides the tendon from superficial to deep, and from medial to lateral. As the fibers are cut, the surgeon will visually and palpably appreciate the immediate retraction of the distal muscle belly.
After the primary tendinous cut, the surgeon must manually palpate the entire release site, sweeping a finger laterally to ensure all anomalous muscular bands have been completely transected. The release must be absolute; any tethering fibers left intact will compromise the clinical outcome. Once complete release is verified, meticulous hemostasis of the cut tendon edges and the underlying muscle bed is achieved.
Historically, some authors advocated for suturing the distal stump of the transected tendon to the overlying deep fascia to prevent excessive retraction or cosmetic deformity. However, contemporary high-volume practice has demonstrated this step to be unnecessary. The muscle naturally retracts and establishes a new, tension-free equilibrium without significant loss of functional adduction strength or visible contour defects. The wound is copiously irrigated with sterile saline. Closure is performed in layers: the deep investing fascia is reapproximated with interrupted 2-0 absorbable sutures (e.g., Vicryl) to eliminate dead space, the subcutaneous layer is closed with 3-0 absorbable sutures, and the skin is closed with a running subcuticular stitch or surgical glue.
Complications, Incidence Rates, and Salvage Management
While the adductor longus tenotomy is generally considered a safe and highly successful procedure when performed for the correct indications, it is not without potential complications. A thorough understanding of these risks and their management is essential for the operating surgeon. The overall complication rate is relatively low, but the consequences of technical errors or misdiagnoses can be severe, leading to prolonged disability for the athlete.
The most feared intraoperative complication is iatrogenic injury to the anterior division of the obturator nerve. This typically occurs due to overly aggressive deep dissection, failure to properly identify the plane between the adductor longus and brevis, or the blind use of electrocautery deep to the tendon. Nerve injury manifests postoperatively as profound weakness in hip adduction and sensory deficits or neuropathic pain over the medial aspect of the thigh. Postoperative hematoma is the most common early complication, resulting from inadequate hemostasis of the highly vascular adductor muscle bed. A large hematoma can cause significant pain, delay rehabilitation, and increase the risk of superficial or deep surgical site infection.
Managing the Failed Tenotomy
The most prevalent "complication" in adductor surgery is actually persistent or recurrent groin pain due to an incorrect initial diagnosis or failure to address concomitant pathology. If a patient undergoes an isolated adductor tenotomy but has an unrecognized, co-existing athletic pubalgia (sports hernia), their pain will predictably persist or worsen as they attempt to return to sport. In these scenarios, a comprehensive re-evaluation is required, often necessitating a secondary procedure by a general surgeon to reinforce the posterior inguinal wall or repair the rectus abdominis insertion. Heterotopic ossification (HO) at the tenotomy site is a rare but documented complication that can cause localized pain and restricted range of motion, potentially requiring surgical excision if conservative management with NSAIDs and physical therapy fails.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Obturator Nerve Injury | < 1% | Strict adherence to the superficial dissection plane; mandatory use of a protective retractor deep to the adductor longus tendon. | Immediate intraoperative microsurgical repair if transected. Postoperative neuropathic pain managed with Gabapentin/Pregabalin; EMG at 6 weeks if deficit persists. |
| Postoperative Hematoma | 2 - 5% | Meticulous bipolar hemostasis of the cut tendon edges and muscle bed prior to closure; avoidance of early aggressive stretching. | Observation for small hematomas. Surgical evacuation and washout if expanding, causing skin compromise, or signs of infection. |
| Persistent Groin Pain | 5 - 15% | Exhaustive preoperative workup to exclude FAI, labral tears, and specifically, concomitant athletic pubalgia. | Multidisciplinary re-evaluation. MRI to check for incomplete release or missed sports hernia. May require secondary pelvic floor/inguinal wall repair. |
| Heterotopic Ossification | < 2% | Minimal tissue trauma; copious irrigation to remove bone dust/debris (though less relevant in soft tissue tenotomy). | NSAIDs (Indomethacin) for early inflammatory phase. Surgical excision only if mature (usually >6-12 months) and mechanically symptomatic. |
Phased Post-Operative Rehabilitation Protocols
The success of an adductor longus tenotomy is inextricably linked to a structured, phased, and highly disciplined postoperative rehabilitation program. The primary goal of rehabilitation is to allow the surgical site to heal without excessive scar tissue formation, while progressively restoring full, pain-free range of motion, core stability, and ultimately, sport-specific explosive power. Rehabilitation is generally divided into three distinct phases, though progression must be criteria-based rather than strictly time-based.
Phase I: Protection and Early Mobilization (Weeks 0-2)
The immediate postoperative phase prioritizes wound healing, pain control, and the prevention of deep vein thrombosis (DVT) and muscle atrophy. Patients are typically allowed to weight-bear as tolerated with the assistance of crutches for the first few days, transitioning to full unassisted weight-bearing by the end of week one as pain allows.
During this phase, aggressive stretching of the adductor complex is strictly prohibited to prevent hematoma formation and disruption of the healing tissue bed. Physical therapy focuses on gentle, pain-free passive and active-assisted range of motion of the hip, emphasizing flexion, extension, and internal rotation. Isometric contractions of the quadriceps, hamstrings, and gluteal muscles are initiated immediately. Modalities such as cryotherapy and transcutaneous electrical nerve stimulation (TENS) are utilized to manage postoperative discomfort and reduce local edema.
Phase II: Core Integration and Progressive Strengthening (Weeks 2-6)
As the acute inflammatory phase subsides and the surgical site stabilizes, the focus shifts to restoring functional strength and integrating the adductor complex with the core musculature. This phase is critical, as the underlying biomechanical deficits that led to the initial injury must be corrected.
Patients begin progressive concentric and eccentric strengthening of the hip abductors, extensors, and external rotators. Adductor strengthening is introduced cautiously, starting with submaximal isometrics and slowly progressing to light concentric resistance using bands or cables. Crucially, intensive core stabilization exercises are incorporated, focusing on the transverse abdominis, obliques, and lumbar multifidi. The goal is to restore the dynamic stability of the pelvic ring. Cardiovascular conditioning is maintained using low-impact modalities such as a stationary bicycle or aquatic therapy, provided the surgical incisions are fully healed.
Phase III: Return to Sport and Plyometrics (Weeks 6-12+)
The final phase of rehabilitation bridges the gap between clinical recovery and athletic performance. Progression into Phase III requires full, pain-free range of motion, symmetrical hip strength (specifically adductor/abductor ratios), and an absence of pain with provocative testing.
This phase introduces advanced, sport-specific drills. Linear running is initiated and progressively advanced to multidirectional agility drills, cutting, and pivoting. Plyometric exercises, such as lateral bounding and box jumps, are incorporated to re-train the stretch-shortening cycle of the adductor musculature. For soccer players, kicking progressions begin with short, controlled passes and advance to maximal effort in-step drives. A successful return to play (RTP) is typically achieved between 8 to 12 weeks postoperatively, though this timeline can vary based on the athlete's specific sport and pre-injury conditioning level.
Summary of Landmark Literature and Clinical Guidelines
The management of chronic groin pain has evolved significantly over the past two decades, moving from a poorly understood "black box" of diagnoses to a highly specific, anatomically based treatment paradigm. This evolution is heavily reflected in the contemporary orthopaedic and sports medicine literature. A pivotal moment in standardizing the approach to this pathology was the Doha agreement meeting on terminology and definitions in groin pain in athletes. This consensus statement was instrumental in classifying groin pain into defined clinical entities: adductor-related, iliopsoas-related, inguinal-related, and pubic-related groin pain. This classification system is now the foundation for clinical diagnosis and research, ensuring that surgical interventions like the adductor tenotomy are applied to the correct patient population.
The literature robustly supports the efficacy of adductor longus tenotomy for isolated, recalcitrant adductor enthesopathy. Landmark studies by authors such as Meyers, who extensively mapped the anatomy of the pubic aponeurosis and core muscle injuries, have highlighted the biomechanical rationale for releasing the adductor longus to decompress the anterior pelvis. Systematic reviews, including those by Machotka et al., have consistently demonstrated high return-to-play rates following tenotomy, often exceeding 85-90% in elite athlete cohorts.
However, the literature also serves as a cautionary tale regarding isolated tenotomies in the presence of complex pelvic pathology. Recent clinical guidelines emphasize that while the tenotomy is highly effective for isolated adductor pain, its success rate drops precipitously if a concomitant weakness of the posterior inguinal wall (sports hernia) is ignored. Therefore, the current standard of care, as dictated by the latest sports medicine literature, demands a multidisciplinary approach. High-level evidence suggests that athletes presenting with combined adductor and inguinal-related pain achieve the best outcomes through a concurrent surgical approach, combining an adductor tenotomy with a laparoscopic or open pelvic floor repair, thereby addressing the entire biomechanical spectrum of the core muscle injury.
