Double Mini-Incision Fasciotomy for Chronic Exertional Compartment Syndrome
Key Takeaway
The double mini-incision fasciotomy is a minimally invasive surgical technique for treating chronic exertional anterior compartment syndrome. By utilizing two 2-cm vertical incisions spaced 15 cm apart, surgeons can achieve complete fascial release while minimizing soft tissue morbidity. This approach avoids tourniquet use, protects the superficial peroneal nerve, and facilitates rapid postoperative rehabilitation, allowing athletes to return to sports within three to four weeks.
Introduction to Chronic Exertional Compartment Syndrome (CECS)
Chronic exertional compartment syndrome (CECS) is a debilitating, exercise-induced neuromuscular condition characterized by reversible ischemia within a closed fibro-osseous space. Most commonly affecting the anterior compartment of the lower leg, CECS is highly prevalent among endurance athletes, military personnel, and individuals engaged in repetitive, high-impact lower extremity activities.
The underlying pathophysiology is driven by the inelasticity of the crural fascia. During strenuous exercise, skeletal muscle volume can increase by up to 20% due to physiological hyperemia and interstitial edema. In a patient with a non-compliant fascial envelope, this volume expansion leads to a pathological rise in intracompartmental pressure (ICP). When ICP exceeds capillary perfusion pressure, a transient ischemic cascade ensues, resulting in severe pain, muscle cramping, and transient neurological deficits such as paresthesia or foot drop.
While conservative measures (e.g., activity modification, orthotics, physical therapy) are often trialed, surgical decompression remains the definitive treatment for refractory cases. The double mini-incision fasciotomy, popularized by Mouhsine et al., represents a significant evolution in the surgical management of anterior CECS. By utilizing two strategically placed 2-cm incisions, this technique provides the direct visualization necessary for a complete fascial release while mitigating the extensive soft tissue morbidity, scarring, and prolonged recovery associated with traditional open, extensile fasciotomies.
Surgical Anatomy and Biomechanics
A profound understanding of the lower extremity compartmental anatomy is mandatory to perform a safe and effective mini-incision fasciotomy.
The Anterior Compartment
The anterior compartment of the leg is bounded medially by the lateral surface of the tibia, laterally by the anterior intermuscular septum, posteriorly by the interosseous membrane, and anteriorly by the unyielding crural fascia.
It contains four primary muscles:
* Tibialis Anterior (TA): The primary dorsiflexor of the ankle.
* Extensor Hallucis Longus (EHL): Extends the great toe and assists in ankle dorsiflexion.
* Extensor Digitorum Longus (EDL): Extends the lesser toes.
* Peroneus Tertius: Assists in dorsiflexion and eversion.
The neurovascular bundle of the anterior compartment consists of the deep peroneal nerve and the anterior tibial artery and vein, which run deeply along the interosseous membrane.
The Superficial Peroneal Nerve (SPN)
The most critical anatomical landmark during this procedure is the superficial peroneal nerve. The SPN courses through the lateral compartment before piercing the crural fascia to become subcutaneous. This fascial penetration typically occurs 10 to 12 cm proximal to the tip of the lateral malleolus—precisely in the vicinity of the distal mini-incision. Iatrogenic injury to the SPN or its branches (the medial and intermediate dorsal cutaneous nerves) can result in painful neuromas and permanent sensory deficits over the dorsum of the foot.
Surgical Warning: The anatomical exit point of the superficial peroneal nerve is highly variable. In approximately 15% of patients, the nerve may exit the fascia more proximally, or branch prior to piercing the fascia. Meticulous blunt dissection and direct visualization at the distal incision site are non-negotiable to prevent iatrogenic transection.
Indications and Preoperative Evaluation
Clinical Presentation
Patients typically present with a classic triad:
1. Aching, burning, or cramping pain in the anterolateral leg that occurs at a specific distance, duration, or intensity of exercise.
2. Relief of symptoms shortly after cessation of the offending activity.
3. Occasional transient neurological symptoms, such as numbness over the first web space (deep peroneal nerve distribution) or transient foot drop during peak exertion.
Diagnostic Criteria
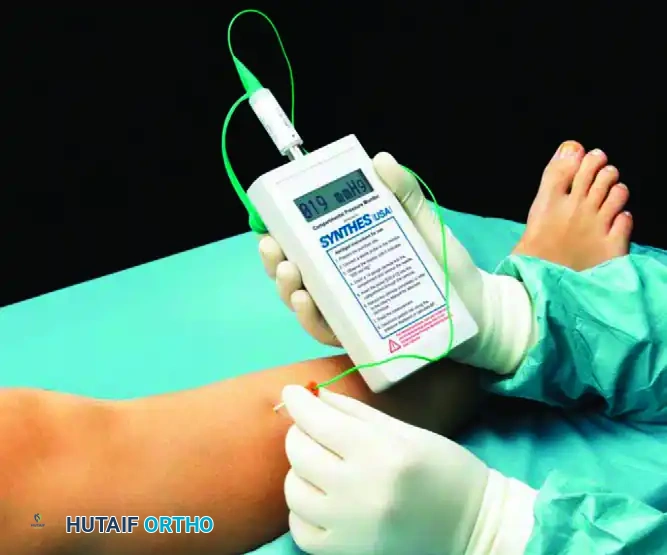
The gold standard for diagnosing CECS is dynamic intracompartmental pressure (ICP) monitoring. The modified Pedowitz criteria are widely accepted for confirming the diagnosis. One or more of the following pressure readings in the anterior compartment are diagnostic:
* Pre-exercise (Resting) Pressure: $\ge$ 15 mm Hg
* 1-Minute Post-exercise Pressure: $\ge$ 30 mm Hg
* 5-Minute Post-exercise Pressure: $\ge$ 20 mm Hg
Indications for Surgery
- Confirmed diagnosis of anterior CECS via dynamic ICP testing.
- Failure of non-operative management (minimum of 3 to 6 months).
- Unwillingness or inability of the patient to permanently modify or abandon the inciting athletic or occupational activities.
Preoperative Planning and Patient Positioning
Anesthesia
The procedure can be performed under general anesthesia, regional anesthesia (spinal or epidural), or a peripheral nerve block (e.g., popliteal block). Local anesthesia with intravenous sedation is also a viable option for highly compliant patients, given the minimally invasive nature of the technique.
Positioning and Preparation
- The patient is placed in the supine position on a standard radiolucent operating table.
- A small bump or sandbag may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the anterolateral aspect of the leg into a direct vertical orientation.
- The entire lower extremity is prepped and draped in a standard sterile fashion from the mid-thigh to the toes.
- Tourniquet Avoidance: As explicitly described by Mouhsine et al., this procedure is performed without the use of a tourniquet.
Clinical Pearl: Avoiding a tourniquet serves multiple critical purposes. First, it prevents tourniquet-induced ischemia, which can exacerbate postoperative pain and delay immediate active range of motion. Second, it allows the surgeon to identify and achieve meticulous hemostasis of any perforating vessels encountered during the fascial release, significantly reducing the risk of postoperative hematoma—a primary cause of delayed healing and recurrent scarring.
Surgical Technique: Step-by-Step
The double mini-incision technique relies on the creation of a mobile subcutaneous window, allowing the surgeon to visualize the entire length of the anterior compartment fascia through two small portals.
Step 1: Incision Marking and Placement
Identify and mark the anatomical landmarks: the tibial crest, the fibular head, and the lateral malleolus. The anterior compartment lies between the tibial crest and the fibular shaft.
Make two vertical 2-cm skin incisions directly over the anterior compartment. These incisions should be spaced approximately 15 cm apart.
* The proximal incision is placed in the proximal third of the leg, approximately 4 to 5 cm distal to the tibial tubercle.
* The distal incision is placed in the distal third of the leg, approximately 10 to 12 cm proximal to the lateral malleolus.
Figure 1: Preoperative marking and placement of the two vertical 2-cm skin incisions over the anterior compartment, spaced 15 cm apart.
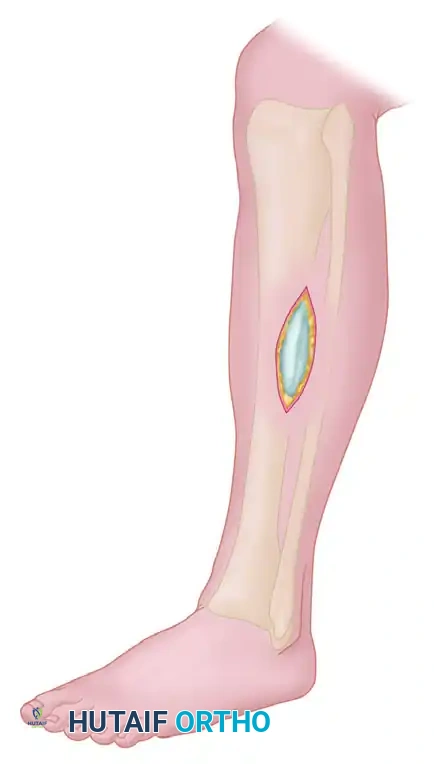
Step 2: Subcutaneous Flap Development
Once the skin is incised, carefully dissect through the subcutaneous fat to identify the glistening white crural fascia.
Using blunt dissection—typically with Metzenbaum scissors, a blunt periosteal elevator, or the surgeon's gloved finger—develop a subcutaneous flap. You must tunnel between the proximal and distal incisions, elevating the bridge of skin and subcutaneous tissue off the underlying deep fascia.
Figure 2: Development of the subcutaneous flap. Blunt dissection is utilized to separate the subcutaneous tissue from the deep fascia, creating a mobile bridge.
Use small Langenbeck or Senn retractors to mobilize this subcutaneous flap. This mobilization is the crux of the "mini-open" technique, as it allows the skin window to be shifted proximally, distally, medially, and laterally, granting a surprisingly expansive clear view of the deep fascia.
Step 3: Nerve Identification and Fascial Release
Attention is first directed to the distal incision.
1. Identify the anterior intermuscular septum, which separates the anterior and lateral compartments.
2. Carefully locate the superficial peroneal nerve as it exits the deep fascia (typically 10 to 12 cm proximal to the lateral malleolus). Protect the nerve with a blunt retractor.
3. Once the nerve is safely isolated, incise the anterior compartment fascia longitudinally.
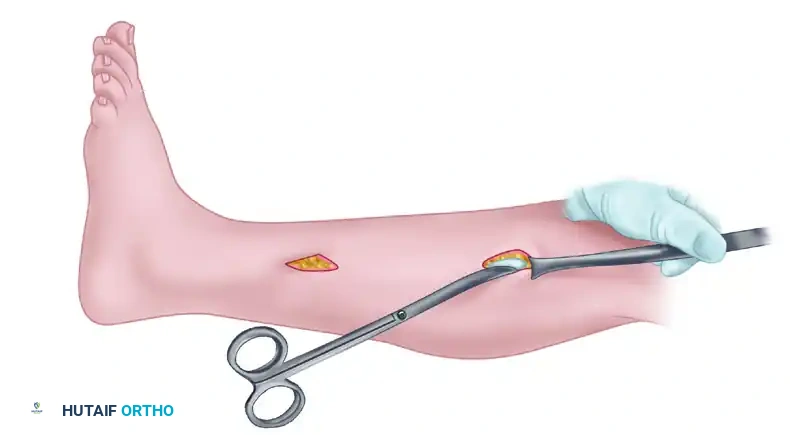
Retract the skin anteriorly and posteriorly using the mobile subcutaneous window to allow the fasciotomy to proceed under direct vision.
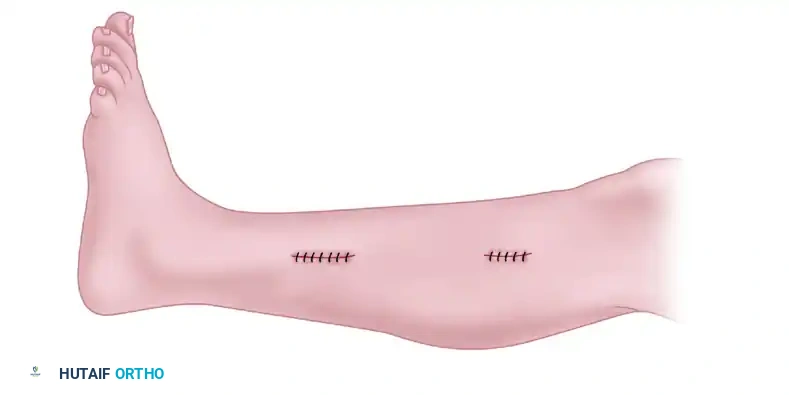
Figure 3: Skin retraction utilizing the mobilized subcutaneous flap. This allows the surgeon to perform the anterior and/or lateral fasciotomy under direct vision, ensuring complete release and nerve protection.
Using long, blunt-tipped Mayo scissors or a specialized fasciotome, extend the fascial release proximally toward the tibial tubercle and distally toward the superior extensor retinaculum.
Surgical Pitfall: Incomplete fascial release is the leading cause of recurrent CECS. The surgeon must ensure the fascia is released completely from the proximal muscle origin down to the extensor retinaculum. If the scissors encounter resistance or if visualization is lost, use a gloved finger inserted through the incisions to palpate the fascial edges and complete the release bluntly, or extend the incision slightly. Never cut blindly.
If a concomitant lateral compartment release is indicated, it can be performed through the same incisions by directing the scissors posteriorly to the anterior intermuscular septum, taking extreme care to protect the superficial peroneal nerve throughout its course.
Step 4: Hemostasis and Closure
Because the procedure is performed without a tourniquet, hemostasis can be evaluated in real-time. Irrigate the subcutaneous tunnel copiously with sterile saline to clear any hematoma. Cauterize any bleeding perforating vessels.
The deep fascia is left entirely open.
Close the two skin incisions meticulously. Standard closure involves using a 3.0 monofilament non-absorbable suture (e.g., Nylon or Prolene) in a simple interrupted or vertical mattress fashion, supplemented with sterile adhesive strips (Steri-Strips).
Figure 4: Final appearance after wound closure. The two mini-incisions are closed with 3.0 monofilament sutures and sterile adhesive strips, minimizing cosmetic deformity.
Apply a sterile, non-adherent dressing over the incisions, followed by a firm, compressive bandage extending from the midfoot to just below the knee. This compression is vital to prevent postoperative hematoma formation within the dead space created by the fascial release.
Postoperative Care and Rehabilitation Protocol
The success of a double mini-incision fasciotomy relies heavily on a structured, progressive postoperative rehabilitation protocol. The primary goals are to prevent hematoma formation, avoid fascial scarring (which can lead to recurrence), and restore normal muscle gliding.
Phase I: Immediate Postoperative Period (Days 0 to 7)
- Elevation and Cryotherapy: The limb must be strictly elevated above the level of the heart for the first 24 to 48 hours to minimize edema. Ice is applied for 20 minutes every 2 hours.
- Weight Bearing: Patients are allowed progressive weight bearing as tolerated. Most patients will require the use of crutches for up to 7 to 10 days to assist with ambulation and reduce mechanical stress on the healing soft tissues.
- Early Mobilization: Supervised active range-of-motion (ROM) exercises for the ankle and toes are initiated immediately in the recovery room. Active dorsiflexion and plantarflexion act as a muscle pump, reducing edema and preventing the cut edges of the fascia from adhering to the underlying muscle.
Phase II: Intermediate Rehabilitation (Weeks 1 to 3)
- Wound Care: Sutures are typically removed at 10 to 14 days postoperatively.
- Physical Therapy: Once the incisions are healed, scar massage is initiated to prevent subcutaneous adhesions.
- Strengthening: Gentle isometric strengthening of the anterior compartment musculature begins, progressing to isotonic exercises using resistance bands.
- Cardiovascular Conditioning: Low-impact activities such as stationary cycling or deep-water running can be introduced once the wounds are fully closed and pain allows.
Phase III: Return to Sport (Weeks 3 to 6)
- Progression: Sports activities and impact loading are gradually resumed at 3 to 4 weeks after surgery, provided the patient has full, painless ROM and symmetrical muscle strength.
- Return to Play: A graduated return-to-run program is implemented. Athletes should begin with short intervals on a soft surface (e.g., a track or treadmill) and incrementally increase distance and intensity. Full return to unrestricted competitive sports is typically achieved between 4 to 6 weeks postoperatively.
Complications and Management
While the double mini-incision technique significantly reduces the complication profile compared to open fasciotomy, surgeons must remain vigilant regarding potential adverse outcomes:
- Superficial Peroneal Nerve Injury: The most feared complication. It can occur via direct transection, traction neuropraxia during retraction, or entrapment in postoperative scar tissue. Meticulous identification at the distal incision is the primary preventative measure.
- Incomplete Release / Recurrence: Failure to release the extreme proximal or distal extents of the fascia will result in persistent symptoms. If recurrence is suspected, repeat dynamic ICP testing is indicated.
- Hematoma Formation: Operating without a tourniquet and achieving meticulous hemostasis minimizes this risk. However, if a large hematoma develops, it can act as a space-occupying lesion, paradoxically increasing compartment pressure or leading to severe fibrosis.
- Infection: Superficial surgical site infections are rare but can occur. They are typically managed effectively with oral antibiotics and local wound care.
- Muscle Herniation: Small fascial defects can occasionally lead to symptomatic muscle herniation. While usually asymptomatic, painful herniations may require subsequent surgical revision or enlargement of the fascial defect to prevent strangulation of the muscle belly.
Conclusion
The Mouhsine et al. double mini-incision fasciotomy is a highly effective, evidence-based surgical intervention for chronic anterior compartment syndrome. By combining the biomechanical necessity of a complete fascial release with the principles of minimally invasive surgery, this technique offers excellent clinical outcomes. The avoidance of a tourniquet, meticulous protection of the superficial peroneal nerve, and an aggressive early mobilization protocol are the cornerstones of success, allowing high-demand patients and athletes to achieve a rapid, durable return to their peak functional baseline.
You Might Also Like