Elbow Arthroscopy & Mini-Arthrotomy for Capitellar OCD and Panner's Disease: A Masterclass
Key Takeaway
Join us in the OR for a masterclass on elbow arthroscopy and mini-arthrotomy for capitellar osteochondritis dissecans (OCD) and Panner's disease. We'll meticulously cover patient selection, anatomical considerations, step-by-step intraoperative execution, crucial pearls and pitfalls, and comprehensive postoperative management to ensure optimal outcomes for these challenging pediatric and adolescent conditions.
Introduction and Epidemiology
Panner’s disease and osteochondritis dissecans (OCD) of the capitellum represent a continuum of radiocapitellar pathology primarily affecting the pediatric and adolescent athletic populations. While historically conflated, these entities possess distinct pathophysiological profiles, demographic distributions, and prognostic trajectories. Panner’s disease is characterized by a transient, self-limiting disruption of the blood supply to the developing ossific nucleus of the capitellum. It typically manifests in preadolescents between the ages of 6 and 10 years. Because the entire ossific nucleus is involved, the condition mimics Legg-Calvé-Perthes disease of the hip but generally resolves with benign neglect and activity modification.

Conversely, OCD of the capitellum involves focal compromise of the subchondral bone, leading to secondary articular surface separation, fragmentation, and potential loose body formation. This condition predominantly affects adolescents aged 10 to 17 years. The epidemiology is heavily skewed toward athletes participating in overhead throwing sports (such as baseball pitching) and upper-extremity weight-bearing activities (such as gymnastics and competitive cheerleading). The repetitive microtrauma inherent in these activities induces valgus extension overload, disproportionately stressing the radiocapitellar articulation.

Understanding the distinction between these two entities is critical for the orthopedic surgeon, as Panner’s disease is universally treated non-operatively, whereas capitellar OCD frequently demands surgical intervention when conservative measures fail, the physis closes, or the lesion becomes unstable.
Surgical Anatomy and Biomechanics
The elbow is a highly congruent, complex hinge-pivot joint comprising three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The ulnohumeral joint primarily dictates flexion and extension, while the radiocapitellar and proximal radioulnar joints facilitate pronation and supination. The capitellum itself is a hemispherical articular prominence located on the anterior and inferior aspects of the lateral distal humerus. It articulates with the concave fovea of the radial head throughout the entire arc of flexion, extension, pronation, and supination.

The vascular anatomy of the capitellum is the fundamental anatomical vulnerability predisposing it to osteochondral pathology. The capitellum is supplied by descending extraosseous branches of the brachial artery, which arborize into end-arterial chondral vessels supplying the osseous nucleus. Unlike the medial epicondyle or the trochlea, the capitellum lacks collateral intraosseous anastomoses. This tenuous, retrograde vascular supply renders the capitellum highly susceptible to ischemic necrosis when subjected to repetitive mechanical stress.

Biomechanically, the radiocapitellar joint is subjected to immense compressive and shear forces during overhead activities. During the late cocking and early acceleration phases of throwing, the elbow experiences significant valgus torque. The anterior band of the ulnar collateral ligament (UCL) provides primary restraint to this valgus stress; however, the radiocapitellar joint serves as the secondary bony stabilizer, absorbing up to 60% of the axial load. This repetitive valgus compression, combined with shear forces during rapid extension and pronation, leads to microvascular thrombosis, subchondral microfractures, and eventual focal avascular necrosis characteristic of OCD.
Indications and Contraindications
The decision-making algorithm for radiocapitellar pathology is dictated by the patient's skeletal maturity, the stability of the lesion, and the presence of mechanical symptoms. Panner's disease is treated non-operatively with cessation of the offending activity until radiographic reossification occurs. For OCD, non-operative management is reserved for stable lesions in skeletally immature patients. Surgical intervention is indicated for unstable lesions, loose bodies, or failure of conservative management after a minimum of 3 to 6 months.

Operative vs Non Operative Management Parameters
| Parameter | Non-Operative Management | Operative Management |
|---|---|---|
| Pathology | Panner's Disease, Stable OCD | Unstable OCD, Loose Bodies, Chondral Flaps |
| Skeletal Maturity | Open capitellar physis | Approaching closure or closed physis |
| Symptoms | Vague aching, no mechanical blocks | Catching, locking, severe loss of extension |
| MRI Findings | Intact cartilage, no fluid behind lesion | Fluid interface behind lesion, subchondral cysts |
| Failed Conservative Tx | N/A (First-line therapy) | Persistent pain after 3-6 months of rest |
| Contraindications | Unstable lesions, mechanical locking | Active joint infection, advanced osteoarthritis |
Pre Operative Planning and Patient Positioning
Thorough preoperative imaging is mandatory. High-quality, orthogonal anteroposterior (AP) and lateral radiographs are the initial step. The AP view often demonstrates radiolucency, flattening, or fragmentation of the capitellum. An AP view in 45 degrees of flexion (the active pitcher's view) can better profile posterior capitellar lesions.
Magnetic Resonance Imaging (MRI) without and with intra-articular contrast (MR arthrogram) is the gold standard for assessing lesion stability. T2-weighted fluid-sensitive sequences are evaluated for a high-signal rim interposing between the osteochondral fragment and the native capitellar bed, which is the hallmark of an unstable lesion. Furthermore, MRI allows for the assessment of concomitant pathology, such as UCL attenuation or radioulnar chondromalacia.

For elbow arthroscopy, the patient may be positioned in the lateral decubitus, prone, or supine suspended position. The lateral decubitus position is highly favored in academic centers for capitellar OCD management. The patient is placed in the lateral position with the operative arm supported over a padded post or suspended via a sterile traction setup. The elbow should be allowed to hang at 90 degrees of flexion, which relaxes the anterior neurovascular structures, allowing them to fall anteriorly and safely away from the joint capsule. A non-sterile tourniquet is placed high on the brachium. Bony landmarks, including the lateral epicondyle, medial epicondyle, radial head, and olecranon, are meticulously outlined with a surgical marker prior to fluid extravasation.
Detailed Surgical Approach and Technique
Arthroscopic Portal Placement
Elbow arthroscopy requires precise portal placement due to the intimate proximity of major neurovascular structures. Joint insufflation with 20 to 30 cc of normal saline via the soft spot (center of the triangle formed by the lateral epicondyle, radial head, and olecranon tip) is a critical first step to push the neurovascular structures anteriorly.

The proximal anteromedial portal is typically established first. It is located 2 cm proximal and 1 cm anterior to the medial epicondyle. The ulnar nerve must be palpated and protected. A spinal needle is used to localize the joint, aiming toward the center of the radiocapitellar articulation. Once established, the arthroscope is introduced to visualize the anterior compartment.
The anterolateral portal is then established under direct intra-articular visualization. It is placed 3 cm distal and 1 cm anterior to the lateral epicondyle. The radial nerve lies in close proximity (average 4-7 mm from the trocar), making precise, "nick-and-spread" technique with a hemostat mandatory before penetrating the capsule.
Diagnostic Arthroscopy and Lesion Preparation
A systematic diagnostic sweep is performed. The radiocapitellar joint is inspected for loose bodies, which frequently sequester in the radiocapitellar recess or the anterior compartment. The capitellar lesion is probed. An intact but ballotable articular surface indicates a grade II lesion, while a partially detached flap indicates a grade III lesion. Grade IV represents a completely detached fragment (loose body) with an empty capitellar crater.


For unsalvageable, fragmented, or purely cartilaginous loose bodies, excision is performed. The capitellar bed must then be meticulously prepared. An arthroscopic curette and motorized shaver are utilized to debride the necrotic subchondral bone back to a stable, bleeding, vertical rim of healthy hyaline cartilage. The zone of calcified cartilage must be entirely removed to expose the subchondral bone plate.

Marrow Stimulation Techniques
For lesions smaller than 10 to 12 mm in diameter, marrow stimulation (microfracture) is the treatment of choice. Using an arthroscopic awl or specialized microfracture picks introduced via the anterolateral or a direct lateral accessory portal, multiple fenestrations are created in the subchondral bone.

The holes should be spaced 2 to 3 mm apart and penetrate deeply enough (usually 2-4 mm) to access the underlying cancellous bone marrow. The tourniquet is temporarily deflated to confirm the egress of marrow fat droplets and blood into the capitellar defect. This marrow clot provides the pluripotential mesenchymal stem cells necessary to generate a fibrocartilage repair tissue (predominantly Type I collagen).

Internal Fixation of Osteochondral Fragments
If the osteochondral fragment is large (greater than 10 mm), contains a substantial amount of subchondral bone, and is acutely detached or hinged, internal fixation should be attempted. The capitellar bed is debrided of fibrous tissue, and the fragment is anatomically reduced.

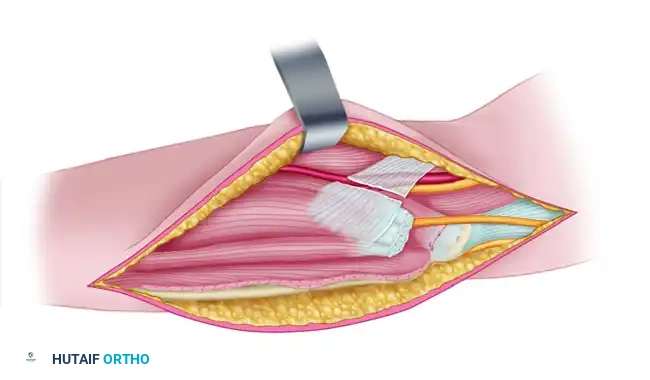
Fixation can be achieved using bioabsorbable pins, darts, or headless titanium compression screws. If headless screws are used, they must be countersunk beneath the articular cartilage surface to prevent iatrogenic damage to the radial head during pronation and supination. Arthroscopic fixation is technically demanding and often requires accessory portals or a mini-open lateral arthrotomy utilizing the Kocher interval (between the extensor carpi ulnaris and the anconeus).
Osteochondral Autograft Transfer System
For large (>12 mm), uncontained, or cystic lesions, or in cases of failed prior microfracture, an Osteochondral Autograft Transfer System (OATS) procedure is indicated. This technique replaces the defect with mature, hyaline cartilage (Type II collagen).

The procedure is typically performed via a mini-open lateral approach. The capitellar defect is sized and reamed to a precise depth (usually 10-12 mm) to create a recipient socket. The donor graft is harvested from a non-weight-bearing portion of the ipsilateral or contralateral lateral femoral condyle of the knee.

The graft must be harvested perpendicularly to the articular surface to ensure a flush fit. The osteochondral plug is then press-fit into the capitellar recipient site. Care is taken to match the contour of the capitellum to prevent step-offs, which could lead to accelerated radial head wear.

Complications and Management
Surgical management of capitellar OCD carries inherent risks, primarily related to the proximity of neurovascular structures and the unique biomechanics of the elbow joint. Iatrogenic nerve injury is the most devastating complication. The radial nerve is at risk during anterolateral portal placement, the median nerve during anteromedial portal placement, and the ulnar nerve during proximal anteromedial portal placement.

Postoperative stiffness is common due to the highly reactive nature of the elbow joint capsule. Heterotopic ossification, while less common in isolated arthroscopy than in trauma, can occur. Failure of graft incorporation or subsidence of an OATS plug can lead to recurrent mechanical symptoms and early-onset osteoarthritis.

Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Nerve Injury (Neuropraxia) | 2% - 5% | Use "nick and spread" technique; distend joint prior to portal entry. Salvage: Observation, EMG at 6 weeks if no recovery. |
| Postoperative Stiffness | 10% - 15% | Early, controlled ROM. Avoid prolonged immobilization. Salvage: Static progressive splinting, arthroscopic capsular release. |
| OATS Graft Subsidence | 5% - 10% | Ensure perpendicular harvest and exact depth matching. Salvage: Revision grafting or fragment excision. |
| Hardware Prominence (Fixation) | < 5% | Countersink headless screws at least 1-2 mm below subchondral bone. Salvage: Arthroscopic hardware removal. |
| Infection | < 1% | Strict sterile technique, prophylactic antibiotics. Salvage: Arthroscopic irrigation and debridement, targeted IV antibiotics. |
Post Operative Rehabilitation Protocols
Rehabilitation protocols must be tailored to the specific surgical intervention performed. The overarching goal is to protect the healing osteochondral interface while preventing capsular contracture.
For patients who undergo simple debridement and microfracture, the elbow is placed in a soft dressing, and immediate active and active-assisted range of motion (ROM) is initiated within 48 hours to stimulate fibrocartilage formation. Weight-bearing and valgus-stress activities are strictly prohibited for 6 weeks. Strengthening begins at 6 to 8 weeks, with a gradual return to throwing or gymnastics typically permitted at 4 to 6 months, contingent upon the resolution of symptoms and radiographic evidence of subchondral healing.

For patients undergoing internal fixation or OATS procedures, rehabilitation is more conservative. The elbow is often splinted in 90 degrees of flexion for 7 to 10 days to allow for soft tissue healing of the mini-open arthrotomy. Following this, a hinged elbow brace is utilized, allowing progressive ROM while protecting against valgus stress. Continuous Passive Motion (CPM) machines may be utilized to promote hyaline cartilage nutrition. Strengthening is delayed until 8 to 12 weeks, and return to high-level impact or throwing sports is generally restricted until 6 to 9 months postoperatively, requiring advanced functional testing prior to clearance.
Summary of Key Literature and Guidelines
The academic literature strongly supports surgical intervention for unstable capitellar OCD lesions, though debate remains regarding the optimal surgical technique for varying lesion sizes. Takahara et al. provided foundational natural history data, demonstrating that conservative management frequently fails in patients with closed physes or large lesions, leading to progressive osteoarthritis.

Current guidelines suggest that arthroscopic debridement and microfracture yield excellent clinical outcomes for contained lesions smaller than 10 to 12 mm. Studies by Ruch and colleagues have shown high rates of return to sport following marrow stimulation in this specific cohort. However, for lesions larger than 12 mm, or those involving the lateral capitellar margin (uncontained lesions), microfracture results in inferior outcomes due to the poor shear-resistance of fibrocartilage.
In these advanced cases, OATS has emerged as the gold standard. Baumgarten and others have published extensive series demonstrating that osteochondral autografting provides superior long-term durability, higher rates of return to competitive throwing, and better restoration of the native radiocapitellar congruency. The orthopedic surgeon must carefully weigh the morbidity of knee graft harvest against the biomechanical necessity of hyaline cartilage restoration in the young, high-demand athlete.
Clinical & Radiographic Imaging
You Might Also Like