Acetabular Fractures: Comprehensive Principles and Operative Management
Key Takeaway
The management of acetabular fractures represents one of the most demanding disciplines in orthopedic trauma. Dictated by a steep learning curve, successful outcomes rely heavily on anatomical reduction of the articular surface. This guide details the critical initial ATLS resuscitation, emergency reduction of hip dislocations, advanced imaging protocols, and the foundational surgical anatomy required to navigate complex acetabular reconstruction and preserve the native hip joint.
ACETABULAR FRACTURES: PRINCIPLES AND MANAGEMENT
The operative treatment of acetabular fractures remains one of the most formidable challenges in the field of orthopedic trauma. It is a complex, continually evolving discipline that demands a profound understanding of pelvic anatomy, spatial reasoning, and meticulous surgical technique. The primary goal of intervention is the restoration of articular congruity to prevent post-traumatic osteoarthritis and preserve the native hip joint.
The mastery of acetabular fracture surgery involves a well-documented and steep learning curve. This was definitively illustrated in a landmark report by Matta and Merritt, which analyzed the first 100 acetabular fractures treated operatively by Matta. By grouping the surgical reductions chronologically into cohorts of 20, the data clearly demonstrated that accumulated experience directly correlated with a surgeon’s ability to avoid unsatisfactory reductions and consistently achieve anatomical restoration. Similarly, Kebaish, Roy, and Rennie reinforced this concept by comparing reductions obtained by experienced pelvic trauma surgeons against those performed by less experienced operators; the latter group demonstrated a significantly lower rate of anatomical reduction, underscoring the necessity of specialized training and high-volume experience in this subspecialty.
Clinical Pearl: The Learning Curve
Acetabular surgery is unforgiving. A residual articular step-off of greater than 2 mm significantly increases the risk of rapid-onset post-traumatic osteoarthritis. Surgeons early in their practice should have a low threshold for referring complex fracture patterns (e.g., associated both-column, transverse-posterior wall) to high-volume tertiary pelvic trauma centers.
INITIAL EVALUATION AND RESUSCITATION
Acetabular fractures are predominantly the result of high-energy blunt trauma, such as motor vehicle collisions or falls from significant heights. Consequently, associated life-threatening injuries to the head, chest, abdomen, and genitourinary system are exceedingly common.
The management of the polytraumatized patient must strictly adhere to the Advanced Trauma Life Support (ATLS) protocols. Orthopedic management of the acetabular fracture must be appropriately integrated into the overarching resuscitation plan. In general, the operative treatment (Open Reduction and Internal Fixation - ORIF) of an acetabular fracture is not an orthopedic emergency. Surgery is typically delayed for 3 to 7 days to allow for hemodynamic stabilization, optimization of the patient, and resolution of intrapelvic hemorrhage.
However, there are absolute indications for emergent surgical intervention:
1. Open Acetabular Fractures: Requiring immediate irrigation and debridement.
2. Irreducible Hip Dislocations: Where closed reduction methods have failed.
3. Progressive Neurologic Deficit: Most commonly involving the sciatic nerve, particularly following a posterior fracture-dislocation.
4. Vascular Injury: Requiring emergent exploration and repair.
In the case of an irreducible dislocation, urgent open reduction of the hip followed by treatment of the associated fracture is mandatory. Delaying reduction exponentially increases the risk of osteonecrosis (avascular necrosis) of the femoral head and exacerbates ongoing cartilaginous damage caused by the sharp, abrasive edges of the fracture fragments.
EMERGENCY MANAGEMENT AND CLOSED REDUCTION
When a patient presents with an acetabular fracture associated with a hip dislocation, closed reduction must be attempted emergently. This should be performed in the emergency department under deep conscious sedation, or ideally, in the operating room under general anesthesia with fluoroscopic guidance to ensure complete muscle relaxation and prevent iatrogenic iatrogenic damage to the femoral head.
Following a successful closed reduction, the stability of the hip must be assessed. If the hip is stable and the patient can be managed on an abduction wedge pillow, skeletal traction may not be strictly necessary. However, for most patients with potentially operative fractures, the application of skeletal traction is highly recommended.
Surgical Warning: Skeletal Traction
We advocate placing patients with unstable or potentially operative acetabular fractures in skeletal traction (20 to 35 pounds) while they are still in the resuscitation area. This maintains joint distraction, prevents the femoral head from repeatedly striking the sharp articular fracture edges, and helps stretch the contracted soft tissue envelope, which facilitates subsequent surgical reduction.
Traction Pin Placement:
We strongly prefer the use of distal femoral traction pins over proximal tibial pins.
* Biomechanics: A distal femoral pin directly transmits traction forces to the hip joint without traversing the knee.
* Surgical Advantage: It allows for intraoperative knee flexion (crucial for relaxing the sciatic nerve during posterior approaches).
* Complication Avoidance: It avoids exacerbating undiagnosed ligamentous knee injuries, which are common in "dashboard" injury mechanisms.
THE CENTRAL FRACTURE-DISLOCATION
Historically, the term "central fracture-dislocation" was used as a catch-all phrase to describe any acetabular fracture accompanied by medial subluxation of the femoral head. While modern orthopedic practice has largely replaced this terminology with the more precise and descriptive Letournel and Judet classification system, a true central fracture-dislocation—where the femoral head is completely dislocated medially through the quadrilateral plate and into the true pelvis—remains a catastrophic and unusual injury requiring urgent attention.
In these severe patterns, the femoral head frequently becomes incarcerated or "locked" between the displaced anterior and posterior column fragments. This makes closed reduction exceptionally difficult.
Reduction Technique for Medial Incarceration:
1. General anesthesia with complete neuromuscular blockade is essential.
2. Fluoroscopic assistance is mandatory.
3. Longitudinal traction alone is often insufficient. Lateral traction must be applied. This can be achieved by placing a large threaded Schanz pin or a specialized lateral traction screw into the greater trochanter, allowing the surgeon to pull the femoral head laterally out of the pelvis while an assistant applies longitudinal traction.
4. Once reduced, the femoral head is profoundly unstable and will immediately redisplace medially if traction is released. Heavy skeletal traction (often requiring up to 35-40 pounds) must be maintained continuously until definitive ORIF can be performed.
ADVANCED IMAGING AND PREOPERATIVE PLANNING
If closed reduction of a hip dislocation associated with an acetabular fracture is unsuccessful, the immediate treatment depends heavily on the surgeon's experience and the availability of advanced imaging.
A rapid, high-resolution Computed Tomography (CT) scan of the pelvis with fine cuts (2-mm to 3-mm) is the gold standard. The CT scan serves several critical functions:
* Identifying Obstructions: It will clearly demonstrate the anatomical block to reduction (e.g., an incarcerated osteochondral fragment, a flipped labrum, or a trapped piriformis tendon).
* Fracture Morphology: It delineates the exact fracture pattern, allowing for accurate classification according to the Letournel system.
* Marginal Impaction: It identifies areas of articular cartilage that have been crushed into the underlying cancellous bone, which will require elevation and bone grafting during surgery.
Pitfall: Inadequate Imaging
Never attempt an open reduction of an acetabular fracture without a high-quality CT scan with 3D reconstructions. Plain radiographs (the AP pelvis and Judet oblique views) are essential for understanding the overall columns, but CT is mandatory for identifying intra-articular debris and planning the trajectory of internal fixation. If your facility cannot obtain these images or manage the resulting surgical complexity, prompt transfer to a Level I trauma center is indicated.
SURGICAL ANATOMY AND BIOMECHANICS
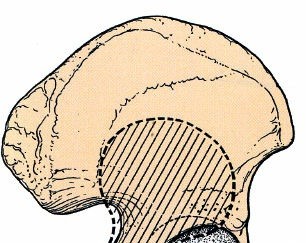
To understand the treatment of acetabular fractures, one must master the complex three-dimensional anatomy of the innominate bone. The acetabulum is best described as an incomplete hemispherical socket with an inverted horseshoe-shaped articular surface (the lunate surface). The inferior aspect of the horseshoe is open, forming the acetabular notch, which is bridged by the transverse acetabular ligament. The central, non-articular portion is the cotyloid fossa, which houses the ligamentum teres and a fat pad.
The Two-Column Concept (Letournel and Judet):
The biomechanical foundation of the acetabulum rests on an inverted "Y" structure, consisting of two distinct columns of bone that transmit weight from the axial skeleton to the lower extremities.
- The Anterior Column: Extends from the anterior iliac crest down to the pubic symphysis. It includes the anterior wall of the acetabulum, the anterior half of the ilium, and the superior and inferior pubic rami.
- The Posterior Column: Extends from the dense bone of the greater sciatic notch down to the ischial tuberosity. It includes the posterior wall of the acetabulum, the quadrilateral surface (the medial wall of the acetabulum), and the ischium.
The thickest and most biomechanically critical portion of the acetabulum is the weight-bearing dome (the superior roof). Fractures that disrupt the dome lead to rapid joint destruction if not anatomically reduced.
SURGICAL APPROACHES: STEP-BY-STEP OVERVIEW
The choice of surgical approach is dictated entirely by the fracture pattern identified on the CT scan. The goal is to choose the approach that provides the most direct access to the displaced articular fragments.
1. The Kocher-Langenbeck Approach
Indications: Posterior wall, posterior column, and certain transverse or T-type fractures where the major displacement is posterior.
Positioning: The patient is placed in the prone or lateral decubitus position. The knee must be flexed to at least 90 degrees, and the hip extended, to remove tension from the sciatic nerve.
Step-by-Step:
* Incision: A curved incision is made starting near the posterior superior iliac spine (PSIS), extending to the greater trochanter, and continuing distally along the femoral shaft.
* Superficial Dissection: The fascia lata is incised, and the gluteus maximus is split in line with its fibers.
* Deep Dissection: The sciatic nerve is identified and gently protected. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) are tagged and tenotomized near their insertion on the greater trochanter.
* Exposure: The rotators are reflected medially over the sciatic nerve, acting as a protective cushion. This exposes the posterior column and the posterior wall of the acetabulum.
* Warning: The quadratus femoris should generally be left intact to protect the ascending branch of the medial circumflex femoral artery, which provides the primary blood supply to the femoral head.
2. The Ilioinguinal Approach
Indications: Anterior column, anterior wall, and associated both-column fractures.
Positioning: Supine on a radiolucent table.
Step-by-Step:
* Incision: Extends from the anterior two-thirds of the iliac crest, curving distally to the pubic symphysis.
* Windows of Access: This approach does not strip muscles off the pelvis but rather works through three distinct anatomical "windows" created by mobilizing neurovascular structures.
* Lateral Window: Lateral to the iliopsoas muscle and femoral nerve. Exposes the internal iliac fossa.
* Middle Window: Between the iliopsoas/femoral nerve laterally and the external iliac vessels medially. Exposes the pelvic brim and quadrilateral plate.
* Medial Window: Medial to the external iliac vessels and lateral to the spermatic cord/round ligament. Exposes the superior pubic ramus.
3. The Anterior Intrapelvic (Modified Stoppa) Approach
Indications: Increasingly utilized as an alternative or adjunct to the ilioinguinal approach for fractures involving the quadrilateral plate and medial displacement.
Positioning: Supine.
Step-by-Step:
* Incision: A transverse Pfannenstiel incision is made just superior to the pubic symphysis.
* Dissection: The rectus abdominis is split vertically in the midline. The transversalis fascia is incised, and the surgeon dissects bluntly into the preperitoneal space of Retzius.
* Exposure: By retracting the bladder and iliac vessels, the surgeon gains direct, orthogonal access to the quadrilateral plate, allowing for the application of buttress plates to prevent medial subluxation of the femoral head.
* Warning: The "Corona Mortis" (an anastomotic vein or artery between the external iliac and obturator systems) is frequently encountered crossing the superior pubic ramus and must be meticulously ligated to prevent catastrophic hemorrhage.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of an anatomically reduced acetabular fracture can be easily compromised by poor postoperative management.
Weight-Bearing Status:
Patients are strictly restricted to touch-down weight-bearing (TDWB) or flat-foot weight-bearing (maximum 20 lbs of force) on the operative extremity for a minimum of 8 to 12 weeks. Early weight-bearing risks catastrophic failure of fixation and loss of articular reduction.
Deep Vein Thrombosis (DVT) Prophylaxis:
Pelvic trauma patients are at an exceptionally high risk for venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) should be initiated as soon as it is surgically safe (typically 12-24 hours postoperatively) and continued for 4 to 6 weeks. Mechanical prophylaxis (SCDs) should be used continuously while the patient is hospitalized.
Heterotopic Ossification (HO) Prophylaxis:
HO is a frequent complication, particularly following the Kocher-Langenbeck or extensile approaches, where extensive muscle stripping occurs. Prophylaxis is highly recommended to prevent severe postoperative stiffness.
* Pharmacologic: Indomethacin (75 mg sustained release daily) for 3 to 6 weeks.
* Radiation: A single dose of 700 to 800 cGy of localized external beam radiation administered within 72 hours of surgery is highly effective and often preferred for high-risk patients.
In conclusion, the management of acetabular fractures requires a synthesis of rigorous ATLS resuscitation, precise interpretation of advanced imaging, and masterful execution of complex surgical exposures. By adhering to these strict biomechanical and anatomical principles, the orthopedic surgeon can navigate the steep learning curve and optimize the long-term survivorship of the patient's native hip joint.
You Might Also Like