Acromioclavicular Joint Injuries: Comprehensive Surgical Management
Key Takeaway
Acromioclavicular (AC) joint injuries typically result from a direct downward force on the acromion. Management is dictated by the Rockwood classification, which assesses the integrity of the AC and coracoclavicular (CC) ligaments, alongside the deltotrapezial fascia. While Types I through III are generally managed non-operatively, Types IV, V, and VI require surgical intervention to restore biomechanical stability and shoulder kinematics.
ACROMIOCLAVICULAR JOINT: ETIOLOGY, BIOMECHANICS, AND CLASSIFICATION
Historical Context and Etiology
Hippocrates was the first to distinguish acromioclavicular (AC) joint injuries from glenohumeral dislocations, accurately delineating their distinct mechanisms of injury. The AC joint represents a critical biomechanical link between the axial skeleton and the upper extremity. Injuries to this articulation are predominantly the result of a direct force applied downward on the acromion.
The most common mechanism of injury is a direct fall onto the lateral dome of the shoulder with the arm adducted. During this impact, the clavicle is driven inferiorly until it rests against the first rib, which blocks further downward displacement. As the scapula and acromion continue to be driven inferiorly, immense stress is placed on the stabilizing ligaments. If the clavicle does not fracture, the acromioclavicular and coracoclavicular (CC) ligaments are sequentially ruptured.
Pathoanatomy and Biomechanics
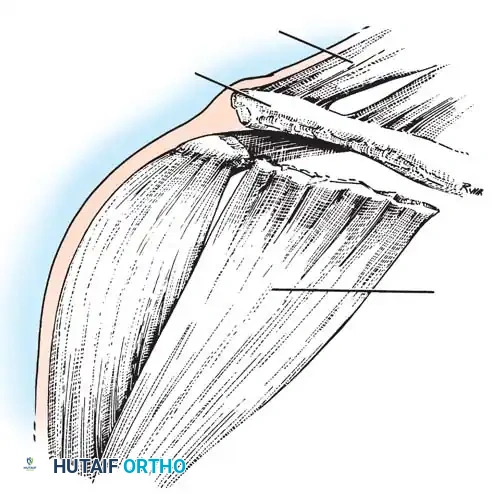
The stability of the AC joint relies on a complex interplay of static and dynamic stabilizers.
* Static Stabilizers: The AC ligaments (superior, inferior, anterior, and posterior) primarily resist anteroposterior (AP) translation. The CC ligaments (conoid and trapezoid) are the primary restraints to superior and inferior translation.
* Dynamic Stabilizers: The anterior deltoid and the trapezius muscles provide dynamic stability through their robust fascial attachments over the distal clavicle and acromion.
In severe injuries, the trauma extends beyond the ligaments to include tears in the clavicular attachments of the deltoid and trapezius muscles, fractures of the acromion, clavicle, or coracoid, disruption of the intra-articular fibrocartilaginous disc, and chondral fractures.
Clinical Pearl: Horn noted the critical clinical association of tears or avulsions of the deltoid and trapezius muscles with high-grade tears of the AC and CC ligaments. The integrity of the deltotrapezial fascia is a primary determinant of the degree of superior clavicular displacement.
In landmark cadaveric dissections, Rosenørn and Pedersen quantified this instability. They found that isolated sectioning of the AC ligament, joint capsule, and overlying muscles resulted in proximal clavicular displacement ranging from 0.5 to 1 cm, accompanied by considerable anteroposterior instability. When the CC ligaments were additionally divided, superior clavicular displacement increased dramatically, ranging from 1.5 to 2.5 cm.
The Rockwood Classification System
Sage and Salvatore initially proposed a classification based on the severity of structural damage, utilizing a three-grade system. However, Rockwood and colleagues expanded this into the universally adopted six-type classification system, which dictates modern treatment algorithms.
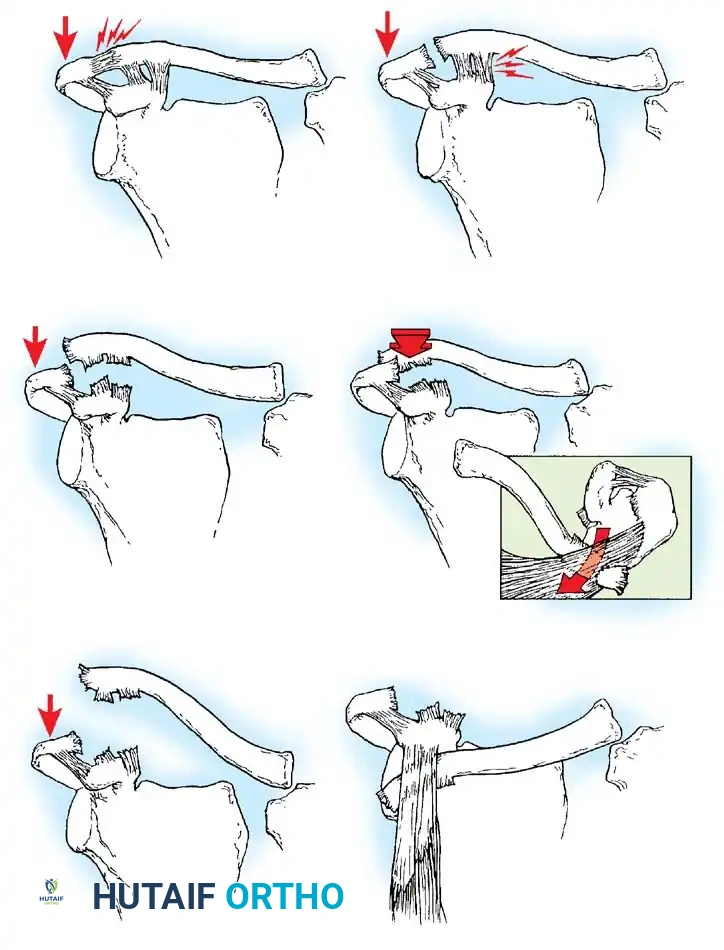
- Type I: Minor sprain of the AC ligament and joint capsule. The joint remains stable, and pain is minimal. Radiographs are typically normal, though late periosteal calcification at the distal clavicle may develop.
- Type II: Complete rupture of the AC ligaments and joint capsule, with intact CC ligaments. The joint exhibits anteroposterior instability. Radiographically, the lateral clavicle may ride slightly higher than the acromion (less than the thickness of the clavicle), even under stress.
- Type III: Complete disruption of both the AC and CC ligaments, alongside tearing of the deltotrapezial fascia. The distal clavicle is elevated above the acromion by at least the thickness of the clavicle (100% displacement). Rockwood emphasized that this deformity is largely due to the scapula and glenohumeral joint being depressed inferiorly, rather than the clavicle pulling superiorly.
- Type IV: Disruption of all AC and CC ligaments with posterior displacement of the distal clavicle into or through the trapezius muscle. This requires a high index of suspicion and an axillary lateral radiograph for diagnosis.
- Type V: Severe disruption of all ligaments and extensive detachment of the deltoid and trapezius from the distal half of the clavicle. The AC joint is displaced 100% to 300%, presenting as a gross, irreducible deformity.
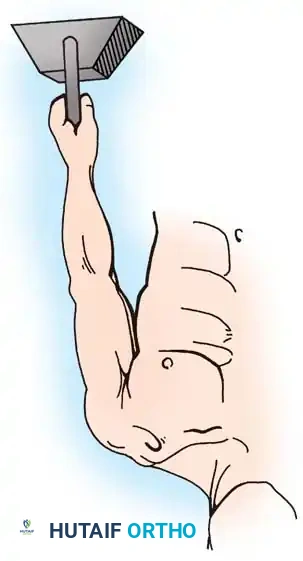
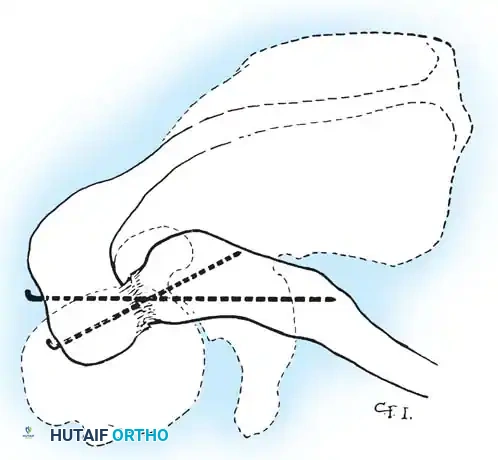
- Type VI: A rare injury caused by extreme hyperabduction. The AC and CC ligaments are torn, and the distal clavicle is dislocated inferiorly under the coracoid process, resting behind the conjoined tendon (biceps and coracobrachialis).
CLINICAL EVALUATION AND DIAGNOSTIC IMAGING
Physical Examination
Patients typically present with localized pain, swelling, and a visible step-off deformity at the AC joint. The distal clavicle is often highly mobile and ballotable (the "piano key" sign). Cross-body adduction testing will reliably reproduce pain in the AC joint.
Radiographic Assessment
Standard AP views of the shoulder may obscure the AC joint due to overpenetration. A dedicated Zanca view (AP radiograph with a 10° to 15° cephalad tilt, using 50% of standard shoulder penetrance) is mandatory.
Urist noted that widening of the AC joint in the AP projection is a hallmark of Type II injuries. To further assess instability, stress radiographs are utilized.
Surgical Warning: When obtaining stress views, 10 to 15 lb (4.5 to 6.8 kg) weights must be tied to the patient's wrists. Having the patient actively grip the weights causes muscle contraction, which can artificially reduce the joint and mask the true degree of instability.

With the patient standing erect, bilateral AP radiographs are compared. In significant subluxations, the lateral clavicle is displaced superiorly (or the scapula inferiorly) by more than half the thickness of the clavicle. In complete dislocations, the displacement equals or exceeds the clavicle's full thickness.
EVIDENCE-BASED MANAGEMENT STRATEGIES
Non-Operative Treatment
Type I and II Injuries: These are universally treated non-surgically. Protocols include cryotherapy, mild analgesics, a brief period of sling immobilization (2 to 3 weeks) for comfort, and early range-of-motion (ROM) exercises. Return to heavy lifting or contact sports is typically restricted for 6 weeks.
Type III Injuries: The management of Type III injuries remains historically controversial but has shifted heavily toward non-operative management. Isokinetic testing demonstrates that non-surgical treatment yields strength and endurance comparable to the uninjured side. While athletes may occasionally report pain with throwing or contact sports, late distal clavicle excision (Mumford procedure) provides excellent salvage relief. The current consensus is an initial non-operative approach for all Type III injuries, reserving surgery for chronic, symptomatic cases.
Operative Indications
Type IV, V, and VI Injuries: There is universal agreement among authorities (Rowe, Neer, Rockwood) that the severe displacement and soft-tissue interposition in these grades are unacceptable. Open reduction and internal fixation (ORIF) or ligamentous reconstruction is strictly indicated.
Urist, Jacobs, and Wade demonstrated that conservative treatment in high-grade injuries fails due to the interposition of the torn articular disc, frayed capsular ligaments, and osteochondral fragments between the acromion and clavicle.
Disadvantages of Closed Treatment in High-Grade Injuries:
- Skin pressure necrosis and ulceration over the prominent clavicle.
- Recurrence of gross deformity.
- Prolonged immobilization (up to 8 weeks).
- Loss of shoulder and elbow motion, particularly in older demographics.
- Late acromioclavicular arthrosis.
- Muscle atrophy, weakness, and fatigue.
Complications of Surgical Intervention:
While surgery restores anatomy, it carries risks including infection, hematoma, hardware migration or breakage, suture loosening, distal clavicle osteolysis, and the potential need for a secondary procedure for hardware removal.
SURGICAL APPROACHES AND OPERATIVE TECHNIQUES
Surgical intervention permits direct joint inspection, debridement of interposed tissue, anatomical reduction, and secure fixation. Procedures are broadly divided into five categories:
1. AC joint reduction and transarticular fixation.
2. CC ligament repair and coracoclavicular fixation.
3. A combination of AC and CC fixation.
4. Distal clavicle excision with ligament reconstruction.
5. Dynamic muscle transfers.
Patient Positioning and Approach
The patient is placed in the beach-chair position at 30° to 45° of elevation. A sabre-cut incision is made in Langer's lines, starting 1 cm posterior to the AC joint and extending anteriorly over the coracoid process. Full-thickness fasciocutaneous flaps are elevated to expose the deltotrapezial fascia.
Technique 1: Acromioclavicular Reduction and Transarticular Fixation
Historically utilized by Murray, Phemister, and Neviaser, this involves direct reduction of the AC joint and stabilization using smooth or threaded Kirschner wires driven from the lateral acromion into the distal clavicle.
Pitfall: Transarticular pinning carries a high risk of hardware migration, pin breakage, and secondary AC joint arthrosis. It is rarely used in modern practice without supplemental CC fixation and is generally reserved for temporary stabilization.
Technique 2: Coracoclavicular (CC) Fixation
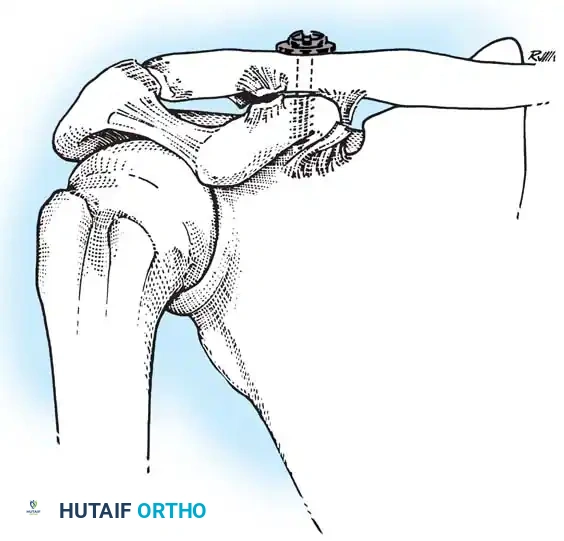
Rigid or semi-rigid fixation between the clavicle and the coracoid process is the cornerstone of modern AC joint reconstruction. Techniques include heavy non-absorbable sutures, metallic screws (Bosworth technique), and modern bioabsorbable suture anchors or cortical button constructs.
When utilizing a coracoclavicular screw, the clavicle is reduced, and a drill hole is placed through the superior clavicle directly into the base of the coracoid. A lag screw is inserted to hold the reduction. This provides rigid fixation but requires routine hardware removal at 8 to 12 weeks to prevent screw breakage once normal scapulothoracic motion resumes.
Technique 3: Ligament Reconstruction and Distal Clavicle Excision
In chronic injuries (or acute injuries with severe comminution), the native ligaments are often irreparable. Weinstein et al. demonstrated that early repairs yield 96% satisfactory results, whereas late reconstructions drop to 77%.
For chronic instability, resection of the distal 1 cm of the clavicle (Mumford procedure) prevents late arthrosis. The CC ligaments are then reconstructed.
The classic Weaver-Dunn procedure involves detaching the coracoacromial (CA) ligament from the acromion and transferring it into the medullary canal of the distal clavicle. Because the CA ligament is biomechanically weaker than the native CC ligaments, this transfer must be protected with supplemental CC fixation (e.g., heavy suture loops or cortical buttons) while the graft heals. Free tendon grafts (e.g., semitendinosus or allograft) looped under the coracoid and through clavicular bone tunnels are increasingly preferred for their superior biomechanical strength.
Technique 4: Muscle Transfers and Deltotrapezial Repair
Regardless of the bony fixation method chosen, meticulous repair of the deltotrapezial fascia is paramount. The deltoid and trapezius muscles are dynamic stabilizers; failure to repair their fascial envelope will result in persistent instability and weakness.
In cases of massive soft tissue loss, dynamic muscle transfers, such as transferring the tip of the coracoid with the attached conjoined tendon to the distal clavicle (Dewar and Barrington technique), can be utilized to hold the lateral clavicle in a reduced position dynamically.
POSTOPERATIVE REHABILITATION PROTOCOL
Successful surgical outcomes depend heavily on strict adherence to postoperative rehabilitation:
* Phase I (0-4 weeks): The shoulder is immobilized in a sling. Active elbow, wrist, and hand ROM are encouraged. Passive forward elevation is limited to 90° to protect the CC reconstruction.
* Phase II (4-8 weeks): Sling is discontinued. Active-assisted ROM begins, gradually progressing to full active ROM. Cross-body adduction and heavy lifting are strictly avoided.
* Phase III (8-12 weeks): Progressive isotonic strengthening of the deltoid, trapezius, and periscapular stabilizers.
* Phase IV (3-6 months): Return to sport-specific activities and heavy labor is permitted once symmetric strength is achieved and radiographic healing is confirmed.
CONCLUSION
The management of acromioclavicular joint injuries requires a nuanced understanding of shoulder biomechanics and a precise application of the Rockwood classification. While conservative management remains the gold standard for low-grade and most Type III injuries, high-grade displacements demand meticulous surgical reconstruction. By combining robust coracoclavicular stabilization with meticulous deltotrapezial fascial repair, orthopedic surgeons can reliably restore function, alleviate pain, and return patients to high-demand activities.
📚 Medical References
You Might Also Like

