ABOS Board Review: Periprosthetic Infections, Systemic Sclerosis, LCH | Part 25

Key Takeaway
This ABOS Board Review covers critical orthopedic topics including periprosthetic joint infections (PJI) – their diagnosis, common organisms like Staphylococci, and management. It also details systemic sclerosis (scleroderma) manifestations like sclerodactyly and calcinosis, and Langerhans Cell Histiocytosis (LCH), including vertebra plana, Birbeck granules, and BRAF mutations.
Question 1
A 62-year-old female is scheduled for a total hip arthroplasty. Her surgeon discusses various measures taken to minimize the risk of periprosthetic joint infection. Which of the following factors is NOT mentioned in the provided text as influencing the infection rate in total hip and knee arthroplasty?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "In total hip and knee arthroplasty, the infection rate is about 0.55–1.27% depending on the design of the surgical theatre, laminar airflow system, antibiotic prophylactic regime, use of antibiotic bone cement, etc." Patient's nutritional status, while a known risk factor for surgical site infections in general, is not explicitly listed in the provided text as one of the factors influencing the infection rate in arthroplasty. All other options are directly mentioned.
Question 2
A 67-year-old male presents with acute onset of severe pain, redness, and swelling in his knee, 3 weeks after undergoing a total knee arthroplasty. He has a high fever and chills. Physical examination reveals a warm, exquisitely tender, and markedly swollen knee joint with purulent discharge from the incision site. What is the most likely classification of this iatrogenic infection?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes "acute onset of severe pain, redness, and swelling," "high fever and chills," and "purulent discharge from the incision site" occurring 3 weeks post-op. The text describes "More serious complication is the inflammation of the surgical site caused by bacteria... with induration, high fever and pus formation in the deeper soft tissue layers." This acute presentation with systemic symptoms and pus is characteristic of an acute periprosthetic joint infection. Delayed wound healing and seroma are less severe conditions without the systemic signs and pus. Chronic PJI typically presents with more subtle symptoms over a longer period (months to years). Aseptic inflammatory reactions do not involve pus or high fever.
Question 3
A 70-year-old female presents with persistent pain and limited range of motion in her right knee, 2 years after total knee arthroplasty. She reports intermittent low-grade fevers. Physical examination reveals a swollen, warm knee with multiple surgical scars and reddish discoloration of the skin. Radiographs show septic loosening of the femoral component with paraarticular ossification and significant osteolytic changes. Which of the following is a key characteristic of the bacterial involvement in this chronic infection?
View Answer & Explanation
Correct Answer: B
Rationale: The text and image (Fig. 2.56 d) state, "Surgical exposure of the same patient: the implant is covered by slime, produced by coagulase-negative Staphylococci. The soft tissues of the joint are also covered by pyogenic pseudomembrane." This "slime" is characteristic of a bacterial biofilm, which is a hallmark of chronic implant-related infections, particularly those caused by coagulase-negative Staphylococci. Rapid systemic dissemination is more typical of acute, virulent infections. Gram-negative organisms are not exclusive, and Staphylococci are more common. There is clearly a host inflammatory response (swelling, redness, osteolysis). While bacteria contribute to bone degradation, the primary mechanism of implant loosening is through the pseudomembrane/biofilm disrupting the bone-implant interface, not direct enzymatic degradation of bone.
Question 4
A 68-year-old male presents with a chronic draining sinus in his right gluteal region, several years after total hip arthroplasty. He has experienced intermittent pain and low-grade fevers. Physical examination reveals erythema and induration around the sinus, with pus discharge. Radiographs show evidence of periprosthetic lucency. What is the most appropriate initial step in the diagnostic workup for identifying the causative organism?

View Answer & Explanation
Correct Answer: D
Rationale: While a draining sinus is present, the most reliable method to identify the causative organism in a periprosthetic joint infection is through joint aspiration for culture. Swab cultures from a draining sinus are often contaminated with skin flora and may not accurately reflect the deep infection. Blood cultures are typically positive only in acute, severe bacteremia, which is less common in chronic PJI. Empiric antibiotics should be avoided before obtaining cultures. MRI is an imaging modality, not a method for organism identification. The text implies that the pus from a draining sinus is "in direct connection with the infected joint," making joint aspiration the definitive method for culture.
Question 5
A 71-year-old female presents with a 6-month history of worsening pain and stiffness in her left knee, 4 years after total knee arthroplasty. She denies fever but reports general malaise. Physical examination reveals a warm, swollen knee with limited range of motion. Laboratory tests show elevated CRP and ESR, but a normal WBC count. Radiographs show progressive radiolucency at the bone-cement interface. Which of the following best describes the typical clinical course of a chronic periprosthetic joint infection?
View Answer & Explanation
Correct Answer: B
Rationale: The vignette describes a chronic presentation (6 months of worsening symptoms, 4 years post-op, low-grade fever or no fever, elevated inflammatory markers but normal WBC). The text states, "The clinical symptoms of an infected orthopedic implant are pain, limited function of the prosthetic joint, erythema in the involved region, subfebrility, elevated levels of C-reactive protein, erythrocyte sedimentation rate and WBC counts." This aligns with an insidious onset of symptoms, often with low-grade or absent fever, which is characteristic of chronic PJI. Rapid onset with high fever and purulent discharge describes acute PJI. The other options do not accurately describe the typical chronic course.
Question 6
A 60-year-old male presents with a chronic infection in his knee following total knee arthroplasty. Surgical exposure reveals the implant covered by slime and the soft tissues of the joint covered by a pyogenic pseudomembrane. Cultures confirm coagulase-negative Staphylococci. What is the primary reason why these organisms are particularly problematic in implant infections?
View Answer & Explanation
Correct Answer: C
Rationale: The text and image context (Fig. 2.56 d) specifically mention "The implant is covered by slime, produced by coagulase-negative Staphylococci." This "slime" is a biofilm, which allows bacteria to adhere to the implant surface and provides a protective barrier against antibiotics and the host immune system, making eradication difficult. While some strains can be antibiotic-resistant, it's their biofilm-forming capability that is the primary reason for their problematic nature in implant infections. They do not typically cause rapid systemic toxicity or directly degrade metal. Coagulase-negative Staphylococci are common skin flora, making them a frequent source of iatrogenic infections.
Question 7
A 73-year-old female presents with a several-year history of increasing pain in her right hip, following total hip arthroplasty. She reports intermittent low-grade fevers and has noticed a small area of redness and induration in her gluteal region, which occasionally drains pus. Radiographs show signs of implant loosening. Which of the following is considered one of the less severe iatrogenic infections following orthopedic surgery, as described in the text?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The range of iatrogenic infections following orthopedic surgical procedures is wide. The less severe condition is a delayed wound healing, seroma formation." All other options (PJI with draining sinus, septic non-union, metallosis with infection, septic loosening) are described or implied as more serious complications, involving deep infection, implant failure, or significant bone pathology. The vignette describes a serious PJI, but the question asks about the *less severe* condition mentioned in the text.
Question 8
A 66-year-old male presents with a 9-month history of progressive pain and swelling in his left knee, 3 years after total knee arthroplasty. He reports no fever but feels generally fatigued. Physical examination reveals a warm, swollen knee with limited range of motion. Radiographs show significant osteolytic changes around the implants. What is the primary clinical manifestation that differentiates an infected orthopedic implant from aseptic loosening?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "pain, limited function of the prosthetic joint, erythema in the involved region, subfebrility, elevated levels of C-reactive protein, erythrocyte sedimentation rate and WBC counts" as clinical symptoms of an infected orthopedic implant. While pain,
Question 8
A 68-year-old male presents with increasing pain, erythema, and swelling around his right knee, 18 months after undergoing a total knee arthroplasty. He reports intermittent low-grade fevers. Laboratory tests reveal elevated C-reactive protein and erythrocyte sedimentation rate. Arthrocentesis is planned. Based on the typical epidemiology of periprosthetic joint infections, which group of organisms is most likely to be identified?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states that Staphylococci (both coagulase-negative and Staphylococcus aureus) are the most important agents, responsible for approximately 50% of all periprosthetic joint infections. While other organisms can cause infection, Staphylococci are by far the most common. Gram-negative bacilli (A) are less common in general PJI but can be seen in specific contexts, and are not the most likely initial finding. Anaerobic bacteria (B) and Fungi (C) are rare causes of PJI. Streptococci (E) are also less common than Staphylococci.
Question 8
A 72-year-old female undergoes an elective total hip arthroplasty. Her surgeon reviews the potential complications with her, including the risk of periprosthetic joint infection (PJI). What is the approximate reported infection rate for total hip and knee arthroplasty procedures?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that "In total hip and knee arthroplasty, the infection rate is about 0.55–1.27% depending on the design of the surgical theatre, laminar airflow system, antibiotic prophylactic regime, use of antibiotic bone cement, etc." This range represents the current understanding of PJI incidence in modern orthopedic surgery. Options A, C, D, and E are either too low or too high for the typical reported rates.
Question 8
A 65-year-old male presents to the clinic with persistent pain and limited function of his right hip, 3 years after a total hip arthroplasty. On examination, there is erythema and induration in the right gluteal region, and he reports systemic symptoms including fever. The image shows local signs of inflammation with pus about to break through the skin.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette and image describe classic signs of a periprosthetic joint infection (PJI): persistent pain, limited function, erythema, induration, pus formation, and systemic symptoms like fever. The image specifically shows local signs of inflammation with pus about to break through the skin, which is a hallmark of deep infection. Aseptic loosening (A) would typically present with pain but without the prominent inflammatory signs, pus, or systemic fever. Heterotopic ossification (B) is calcification in soft tissues and would not present with pus or systemic fever. Deep vein thrombosis (D) would present with swelling and pain, but typically not erythema, induration, or pus in the gluteal region, nor fever in this context. Sciatic nerve irritation (E) would present with neurological symptoms, not local inflammation and pus.
Question 8
A 58-year-old female presents with a small discharging sinus in her groin, 2 years after a total hip arthroplasty. She has experienced intermittent pain and swelling around the hip. Plain radiographs show radiolucency around the entire implant. To further evaluate the extent and origin of the sinus tract, which diagnostic imaging modality is most indicated?

View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states, "In case of discharging sinuses fistulography is a useful tool." The image provided (Fig. 2.54) demonstrates how fistulography uses radiopaque fluid to show the way of pus through the discharging sinus, confirming its direct connection with the infected joint. While MRI (A) and CT (B) can provide detailed anatomical information, they are not as effective as fistulography for mapping the specific tract of a draining sinus. A bone scan (C) can indicate increased metabolic activity but does not delineate the sinus tract. Ultrasound (E) may show superficial fluid collections but lacks the depth and clarity for a complex sinus tract connected to a joint.
Question 8
A 70-year-old male presents with chronic pain and swelling in his left knee, 5 years after a total knee arthroplasty. Clinical examination reveals a red, swollen joint with several surgical scars. Radiographs are obtained, showing septic loosening of the total knee replacement. Which of the following radiographic findings is most indicative of septic loosening in a total knee arthroplasty?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.56 describe septic loosening of a total knee replacement, specifically noting that "In the anteroposterior aspect (b) the femoral component is tilted and paraarticular ossification is seen as a sign of septic complication. The lateral view (c) represents huge osteolytic changes around the implants." These findings, particularly component tilting and extensive osteolysis, are characteristic of septic loosening. Absence of radiolucency (A) and stable implant position (B) would suggest a well-fixed, uninfected implant. Isolated polyethylene wear (D) is a sign of aseptic loosening or wear, not typically septic loosening. Minimal periosteal reaction (E) is non-specific and not a primary indicator of septic loosening.
Question 8
During revision surgery for a chronically infected total knee arthroplasty in a 68-year-old patient, the surgeon observes the implant covered by a slimy substance and the soft tissues of the joint covered by a pyogenic pseudomembrane. What is the primary role of this bacterial pseudomembrane in the context of periprosthetic joint infection?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly states that "The connection between the implant and the host bone is disturbed by bacterial pseudomembrane." This pseudomembrane, often a biofilm, acts as a barrier, preventing host immune cells and antibiotics from reaching the bacteria, and physically interferes with the normal bone-implant interface, leading to loosening. Options A, B, D, and E describe beneficial or neutral effects, which are contrary to the pathological role of a bacterial pseudomembrane in infection.
Question 8
A 75-year-old patient undergoes revision surgery for a chronic periprosthetic knee infection. Intraoperatively, the surgeon notes that the implant is covered by a characteristic "slime" and a pyogenic pseudomembrane. Culture results later confirm the presence of coagulase-negative Staphylococci. What is the significance of this "slime" production by coagulase-negative Staphylococci?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context mentions that "the implant is covered by slime, produced by coagulase-negative Staphylococci." This slime is a key component of the bacterial biofilm, which is crucial for the persistence of periprosthetic joint infections. Biofilms protect bacteria from host immune responses and reduce antibiotic penetration, making infections difficult to eradicate. While coagulase-negative Staphylococci are a common cause of PJI, their slime production is associated with chronic, rather than rapidly progressing, infections (A). It has significant clinical implications (B). It is not an allergic reaction (D). While severe PJI can lead to systemic sepsis, the slime's primary role is in local infection persistence (E).
Question 8
A 45-year-old male presents with a severe deformity of his lower leg and a significant limb length discrepancy following a complex open tibia fracture that developed into a septic non-union. Radiographs show a large bone defect and pseudoarticulation. What is the most likely long-term consequence of this condition if not adequately treated?

View Answer & Explanation
Correct Answer: B
Rationale: The clinical context and Fig. 2.57 describe a "Septic defect tibial non-union (pseudoarticulation) with a severe deformity of the leg and limb length discrepancy." Untreated or inadequately treated septic non-unions are characterized by chronic infection, ongoing bone destruction, and mechanical instability. This inevitably leads to progressive deformity, chronic pain, and severe functional impairment, often requiring complex reconstructive surgery or amputation. Spontaneous resolution (A) is highly unlikely in a septic non-union with a large bone defect. It does not typically lead to a benign bone tumor (C). Complete restoration of limb length and function (D) would require successful treatment. Conversion to an aseptic non-union (E) is not a natural progression; the infection must be eradicated first.
Question 8
A 60-year-old patient with a history of a modular tumor knee endoprosthesis presents with a grayish discoloration of the skin around the knee and chronic pain. Surgical exposure reveals a black synovial membrane full of wear particles. This presentation is consistent with an infected prosthesis complicated by metallosis. What is the primary mechanism by which the metal particles cause the grayish skin discoloration?

View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly describes this phenomenon: "The metal particles are transported by phagocytes through the lymphatic vessels; the skin has a grayish color." This explains the localized discoloration as phagocytes carrying metal debris migrate through the lymphatic system to the skin. Direct absorption (A) or systemic circulation (B) would not typically cause such localized and specific discoloration. Allergic reactions (D) and melanin overproduction (E) are not the described mechanisms for metallosis-induced skin changes.
Question 8
A 63-year-old female presents with new onset pain and swelling in her left hip, 6 months after a total hip arthroplasty. She reports feeling generally unwell and has had intermittent low-grade fevers. Which of the following laboratory findings would be most consistent with a periprosthetic joint infection?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that "The clinical symptoms of an infected orthopedic implant are pain, limited function of the prosthetic joint, erythema in the involved region, subfebrility, elevated levels of C-reactive protein, erythrocyte sedimentation rate and WBC counts." Therefore, elevated CRP and ESR are key systemic inflammatory markers indicative of infection. Normal CRP and ESR (A) would argue against infection. A decreased WBC count (C) is not typical for an active infection. Elevated hemoglobin and hematocrit (D) are not direct indicators of infection. Normal synovial fluid WBC count (E) would argue against a joint infection.
Question 8
A 70-year-old male with a total knee arthroplasty presents with chronic knee pain. Radiographs show significant osteolytic changes around the implants and a tilted femoral component. The connection between the implant and the host bone appears disturbed. What is the most likely underlying cause for these radiographic findings in the context of infection?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context explicitly states, "The connection between the implant and the host bone is disturbed by bacterial pseudomembrane." This pseudomembrane (biofilm) is a hallmark of periprosthetic infection and directly contributes to osteolysis and implant loosening by creating an inflammatory environment and physically separating the implant from the bone. While mechanical wear (A) can cause aseptic loosening and osteolysis, the presence of a tilted component and the context of infection point more strongly to the bacterial pseudomembrane. Stress shielding (C) typically causes bone atrophy, not extensive osteolysis around the implant. Osteoporosis (D) can contribute to poor bone quality but doesn't directly cause the specific pattern of septic loosening. Ligamentous laxity (E) is a soft tissue issue and not the direct cause of osteolytic changes around the implant.
Question 8
A 62-year-old female develops a periprosthetic joint infection after a total hip arthroplasty. The infection is caused by coagulase-negative Staphylococci. These bacteria are known to produce a "slime" layer. What is the primary function of this slime layer in the pathogenesis of chronic periprosthetic infections?
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions that the implant is "covered by slime, produced by coagulase-negative Staphylococci." This slime is a key component of the bacterial biofilm. Biofilms are crucial in chronic infections as they provide a protective barrier for bacteria, shielding them from host immune defenses and significantly reducing the efficacy of antibiotics, leading to persistent infection and difficulty in eradication. It does not primarily enhance motility (A), facilitate rapid replication (B), stimulate bone growth (D), or directly neutralize immune cells (E) in the way a biofilm protects the colony.
Question 8
A 55-year-old male develops a surgical site infection with induration, high fever, and pus formation in the deeper soft tissue layers following an open reduction and internal fixation of a distal tibia fracture. This type of infection, occurring after a surgical procedure, is broadly classified as:
View Answer & Explanation
Correct Answer: C
Rationale: The entire section is titled "2.4 Iatrogenic Infections" and the introductory paragraph states, "The range of iatrogenic infections following orthopedic surgical procedures is wide." An iatrogenic infection is one caused by medical examination or treatment. In this case, the infection directly resulted from the surgical procedure. Hematogenous (A) refers to spread through the bloodstream. Contiguous (B) refers to spread from an adjacent infected site. Spontaneous (D) implies no clear external cause. Opportunistic (E) refers to infections by organisms that usually do not cause disease in a healthy host, which may be true for some iatrogenic infections but "iatrogenic" is the more encompassing and specific term for the cause.
Question 8
A 68-year-old patient presents with a small discharging sinus in the vicinity of his total hip arthroplasty, performed 4 years prior. He has no systemic symptoms, but local erythema is noted. Radiographs show radiolucency around the implant. Which of the following conditions is most likely represented by this clinical picture?
View Answer & Explanation
Correct Answer: B
Rationale: The presence of a discharging sinus following arthroplasty, especially with radiolucency around the implant, is a classic sign of a periprosthetic joint infection (PJI). The text states, "The infected implant or other device may become loosened, and the pus produced around the foreign material may come through the skin, causing a draining sinus." While aseptic loosening (A) can cause pain and radiolucency, it does not typically present with a draining sinus. Sterile seroma (C) would not typically have a draining sinus connected to the joint or cause implant loosening. Allergic reactions (D) are rare and do not typically cause draining sinuses or radiolucency. DVT (E) would present differently and not with a sinus tract from the joint.
Question 8
During surgical exploration of an infected modular tumor knee endoprosthesis, the synovial membrane is observed to have a distinct black color and is full of wear particles. This finding is characteristic of metallosis. What is the primary reason for the black discoloration of the synovial membrane in this context?

View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.60 explicitly state that in metallosis, "the synovial membrane has a black color, it is full with wear particles." This black discoloration is directly caused by the accumulation and deposition of these metal wear particles within the synovial tissue, often taken up by phagocytes. Hemarthrosis (A) would typically cause a reddish-brown discoloration. Melanin (B) is not the cause in this context. Necrosis (D) would present with different tissue characteristics. Fungal colonization (E) would have a different appearance and would be confirmed by culture.
Question 8
A 60-year-old patient with an infected modular tumor knee endoprosthesis develops metallosis, characterized by grayish skin discoloration and a black synovial membrane. The clinical context describes the transport of metal particles by phagocytes. Through which anatomical structures are these metal particles primarily transported to cause the skin discoloration?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly states, "The metal particles are transported by phagocytes through the lymphatic vessels; the skin has a grayish color." This describes the mechanism of how the metal particles, once phagocytosed, are carried away from the joint, eventually leading to deposition and discoloration in the skin. Arterial (A) and venous (B) circulation are primarily for blood flow, not for the transport of particulate matter by phagocytes to cause localized skin discoloration in this manner. Nerve sheaths (D) and direct tissue diffusion (E) are not the primary transport mechanisms for these particles.
Question 8
A 72-year-old female presents with chronic pain and swelling in her right knee, 4 years after a total knee arthroplasty. Radiographs reveal septic loosening of the implant, including a tilted femoral component and extensive osteolytic changes. Additionally, paraarticular ossification is noted. What is the significance of paraarticular ossification in the context of a total knee arthroplasty?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.56 explicitly state that "paraarticular ossification is seen as a sign of septic complication" in the context of septic loosening of a total knee replacement. While some degree of heterotopic ossification can occur post-operatively, significant or progressive paraarticular ossification in the setting of pain and other signs of infection is a strong indicator of a septic process. It is not a normal finding (A) in this context, nor does it specifically indicate aseptic loosening (B) or primary metabolic bone disease (D). It is clinically relevant (E) as a marker of infection.
Question 8
A 67-year-old male presents with erythema and induration in his right gluteal region, several years following a total hip arthroplasty. He reports systemic symptoms including fever, and there is pus about to break through the skin. This delayed presentation of infection, occurring years after the initial surgery, is most consistent with which type of periprosthetic joint infection?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes symptoms appearing "several years following total hip arthroplasty." Periprosthetic joint infections are often classified by their time of onset. Infections presenting years after surgery, especially with chronic signs like induration, pus formation, and systemic symptoms, are characteristic of late chronic infections. Acute postoperative infections (A) typically occur within weeks. Early chronic infections (B) might occur within a few months to a year. Superficial wound infections (D) are localized to the skin and subcutaneous tissue and usually
Question 9
A 68-year-old male presents with increasing pain, erythema, and swelling around his right knee, 18 months after undergoing a total knee arthroplasty. He reports intermittent low-grade fevers. Laboratory tests reveal elevated C-reactive protein and erythrocyte sedimentation rate. Arthrocentesis is planned. Based on the typical epidemiology of periprosthetic joint infections, which group of organisms is most likely to be identified?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states that Staphylococci (both coagulase-negative and Staphylococcus aureus) are the most important agents, responsible for approximately 50% of all periprosthetic joint infections. While other organisms can cause infection, Staphylococci are by far the most common. Gram-negative bacilli (A) are less common in general PJI but can be seen in specific contexts, and are not the most likely initial finding. Anaerobic bacteria (B) and Fungi (C) are rare causes of PJI. Streptococci (E) are also less common than Staphylococci.
Question 10
A 72-year-old female undergoes an elective total hip arthroplasty. Her surgeon reviews the potential complications with her, including the risk of periprosthetic joint infection (PJI). What is the approximate reported infection rate for total hip and knee arthroplasty procedures?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that "In total hip and knee arthroplasty, the infection rate is about 0.55–1.27% depending on the design of the surgical theatre, laminar airflow system, antibiotic prophylactic regime, use of antibiotic bone cement, etc." This range represents the current understanding of PJI incidence in modern orthopedic surgery. Options A, C, D, and E are either too low or too high for the typical reported rates.
Question 11
A 65-year-old male presents to the clinic with persistent pain and limited function of his right hip, 3 years after a total hip arthroplasty. On examination, there is erythema and induration in the right gluteal region, and he reports systemic symptoms including fever. The image shows local signs of inflammation with pus about to break through the skin.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette and image describe classic signs of a periprosthetic joint infection (PJI): persistent pain, limited function, erythema, induration, pus formation, and systemic symptoms like fever. The image specifically shows local signs of inflammation with pus about to break through the skin, which is a hallmark of deep infection. Aseptic loosening (A) would typically present with pain but without the prominent inflammatory signs, pus, or systemic fever. Heterotopic ossification (B) is calcification in soft tissues and would not present with pus or systemic fever. Deep vein thrombosis (D) would present with swelling and pain, but typically not erythema, induration, or pus in the gluteal region, nor fever in this context. Sciatic nerve irritation (E) would present with neurological symptoms, not local inflammation and pus.
Question 12
A 58-year-old female presents with a small discharging sinus in her groin, 2 years after a total hip arthroplasty. She has experienced intermittent pain and swelling around the hip. Plain radiographs show radiolucency around the entire implant. To further evaluate the extent and origin of the sinus tract, which diagnostic imaging modality is most indicated?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states, "In case of discharging sinuses fistulography is a useful tool." The image provided (Fig. 2.54) demonstrates how fistulography uses radiopaque fluid to show the way of pus through the discharging sinus, confirming its direct connection with the infected joint. While MRI (A) and CT (B) can provide detailed anatomical information, they are not as effective as fistulography for mapping the specific tract of a draining sinus. A bone scan (C) can indicate increased metabolic activity but does not delineate the sinus tract. Ultrasound (E) may show superficial fluid collections but lacks the depth and clarity for a complex sinus tract connected to a joint.
Question 13
A 70-year-old male presents with chronic pain and swelling in his left knee, 5 years after a total knee arthroplasty. Clinical examination reveals a red, swollen joint with several surgical scars. Radiographs are obtained, showing septic loosening of the total knee replacement. Which of the following radiographic findings is most indicative of septic loosening in a total knee arthroplasty?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.56 describe septic loosening of a total knee replacement, specifically noting that "In the anteroposterior aspect (b) the femoral component is tilted and paraarticular ossification is seen as a sign of septic complication. The lateral view (c) represents huge osteolytic changes around the implants." These findings, particularly component tilting and extensive osteolysis, are characteristic of septic loosening. Absence of radiolucency (A) and stable implant position (B) would suggest a well-fixed, uninfected implant. Isolated polyethylene wear (D) is a sign of aseptic loosening or wear, not typically septic loosening. Minimal periosteal reaction (E) is non-specific and not a primary indicator of septic loosening.
Question 14
During revision surgery for a chronically infected total knee arthroplasty in a 68-year-old patient, the surgeon observes the implant covered by a slimy substance and the soft tissues of the joint covered by a pyogenic pseudomembrane. What is the primary role of this bacterial pseudomembrane in the context of periprosthetic joint infection?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly states that "The connection between the implant and the host bone is disturbed by bacterial pseudomembrane." This pseudomembrane, often a biofilm, acts as a barrier, preventing host immune cells and antibiotics from reaching the bacteria, and physically interferes with the normal bone-implant interface, leading to loosening. Options A, B, D, and E describe beneficial or neutral effects, which are contrary to the pathological role of a bacterial pseudomembrane in infection.
Question 15
A 75-year-old patient undergoes revision surgery for a chronic periprosthetic knee infection. Intraoperatively, the surgeon notes that the implant is covered by a characteristic "slime" and a pyogenic pseudomembrane. Culture results later confirm the presence of coagulase-negative Staphylococci. What is the significance of this "slime" production by coagulase-negative Staphylococci?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context mentions that "the implant is covered by slime, produced by coagulase-negative Staphylococci." This slime is a key component of the bacterial biofilm, which is crucial for the persistence of periprosthetic joint infections. Biofilms protect bacteria from host immune responses and reduce antibiotic penetration, making infections difficult to eradicate. While coagulase-negative Staphylococci are a common cause of PJI, their slime production is associated with chronic, rather than rapidly progressing, infections (A). It has significant clinical implications (B). It is not an allergic reaction (D). While severe PJI can lead to systemic sepsis, the slime's primary role is in local infection persistence (E).
Question 16
A 45-year-old male presents with a severe deformity of his lower leg and a significant limb length discrepancy following a complex open tibia fracture that developed into a septic non-union. Radiographs show a large bone defect and pseudoarticulation. What is the most likely long-term consequence of this condition if not adequately treated?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context and Fig. 2.57 describe a "Septic defect tibial non-union (pseudoarticulation) with a severe deformity of the leg and limb length discrepancy." Untreated or inadequately treated septic non-unions are characterized by chronic infection, ongoing bone destruction, and mechanical instability. This inevitably leads to progressive deformity, chronic pain, and severe functional impairment, often requiring complex reconstructive surgery or amputation. Spontaneous resolution (A) is highly unlikely in a septic non-union with a large bone defect. It does not typically lead to a benign bone tumor (C). Complete restoration of limb length and function (D) would require successful treatment. Conversion to an aseptic non-union (E) is not a natural progression; the infection must be eradicated first.
Question 17
A 60-year-old patient with a history of a modular tumor knee endoprosthesis presents with a grayish discoloration of the skin around the knee and chronic pain. Surgical exposure reveals a black synovial membrane full of wear particles. This presentation is consistent with an infected prosthesis complicated by metallosis. What is the primary mechanism by which the metal particles cause the grayish skin discoloration?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly describes this phenomenon: "The metal particles are transported by phagocytes through the lymphatic vessels; the skin has a grayish color." This explains the localized discoloration as phagocytes carrying metal debris migrate through the lymphatic system to the skin. Direct absorption (A) or systemic circulation (B) would not typically cause such localized and specific discoloration. Allergic reactions (D) and melanin overproduction (E) are not the described mechanisms for metallosis-induced skin changes.
Question 18
A 63-year-old female presents with new onset pain and swelling in her left hip, 6 months after a total hip arthroplasty. She reports feeling generally unwell and has had intermittent low-grade fevers. Which of the following laboratory findings would be most consistent with a periprosthetic joint infection?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that "The clinical symptoms of an infected orthopedic implant are pain, limited function of the prosthetic joint, erythema in the involved region, subfebrility, elevated levels of C-reactive protein, erythrocyte sedimentation rate and WBC counts." Therefore, elevated CRP and ESR are key systemic inflammatory markers indicative of infection. Normal CRP and ESR (A) would argue against infection. A decreased WBC count (C) is not typical for an active infection. Elevated hemoglobin and hematocrit (D) are not direct indicators of infection. Normal synovial fluid WBC count (E) would argue against a joint infection.
Question 19
A 70-year-old male with a total knee arthroplasty presents with chronic knee pain. Radiographs show significant osteolytic changes around the implants and a tilted femoral component. The connection between the implant and the host bone appears disturbed. What is the most likely underlying cause for these radiographic findings in the context of infection?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context explicitly states, "The connection between the implant and the host bone is disturbed by bacterial pseudomembrane." This pseudomembrane (biofilm) is a hallmark of periprosthetic infection and directly contributes to osteolysis and implant loosening by creating an inflammatory environment and physically separating the implant from the bone. While mechanical wear (A) can cause aseptic loosening and osteolysis, the presence of a tilted component and the context of infection point more strongly to the bacterial pseudomembrane. Stress shielding (C) typically causes bone atrophy, not extensive osteolysis around the implant. Osteoporosis (D) can contribute to poor bone quality but doesn't directly cause the specific pattern of septic loosening. Ligamentous laxity (E) is a soft tissue issue and not the direct cause of osteolytic changes around the implant.
Question 20
A 62-year-old female develops a periprosthetic joint infection after a total hip arthroplasty. The infection is caused by coagulase-negative Staphylococci. These bacteria are known to produce a "slime" layer. What is the primary function of this slime layer in the pathogenesis of chronic periprosthetic infections?
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions that the implant is "covered by slime, produced by coagulase-negative Staphylococci." This slime is a key component of the bacterial biofilm. Biofilms are crucial in chronic infections as they provide a protective barrier for bacteria, shielding them from host immune defenses and significantly reducing the efficacy of antibiotics, leading to persistent infection and difficulty in eradication. It does not primarily enhance motility (A), facilitate rapid replication (B), stimulate bone growth (D), or directly neutralize immune cells (E) in the way a biofilm protects the colony.
Question 21
A 55-year-old male develops a surgical site infection with induration, high fever, and pus formation in the deeper soft tissue layers following an open reduction and internal fixation of a distal tibia fracture. This type of infection, occurring after a surgical procedure, is broadly classified as:
View Answer & Explanation
Correct Answer: C
Rationale: The entire section is titled "2.4 Iatrogenic Infections" and the introductory paragraph states, "The range of iatrogenic infections following orthopedic surgical procedures is wide." An iatrogenic infection is one caused by medical examination or treatment. In this case, the infection directly resulted from the surgical procedure. Hematogenous (A) refers to spread through the bloodstream. Contiguous (B) refers to spread from an adjacent infected site. Spontaneous (D) implies no clear external cause. Opportunistic (E) refers to infections by organisms that usually do not cause disease in a healthy host, which may be true for some iatrogenic infections but "iatrogenic" is the more encompassing and specific term for the cause.
Question 22
A 68-year-old patient presents with a small discharging sinus in the vicinity of his total hip arthroplasty, performed 4 years prior. He has no systemic symptoms, but local erythema is noted. Radiographs show radiolucency around the implant. Which of the following conditions is most likely represented by this clinical picture?
View Answer & Explanation
Correct Answer: B
Rationale: The presence of a discharging sinus following arthroplasty, especially with radiolucency around the implant, is a classic sign of a periprosthetic joint infection (PJI). The text states, "The infected implant or other device may become loosened, and the pus produced around the foreign material may come through the skin, causing a draining sinus." While aseptic loosening (A) can cause pain and radiolucency, it does not typically present with a draining sinus. Sterile seroma (C) would not typically have a draining sinus connected to the joint or cause implant loosening. Allergic reactions (D) are rare and do not typically cause draining sinuses or radiolucency. DVT (E) would present differently and not with a sinus tract from the joint.
Question 23
During surgical exploration of an infected modular tumor knee endoprosthesis, the synovial membrane is observed to have a distinct black color and is full of wear particles. This finding is characteristic of metallosis. What is the primary reason for the black discoloration of the synovial membrane in this context?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.60 explicitly state that in metallosis, "the synovial membrane has a black color, it is full with wear particles." This black discoloration is directly caused by the accumulation and deposition of these metal wear particles within the synovial tissue, often taken up by phagocytes. Hemarthrosis (A) would typically cause a reddish-brown discoloration. Melanin (B) is not the cause in this context. Necrosis (D) would present with different tissue characteristics. Fungal colonization (E) would have a different appearance and would be confirmed by culture.
Question 24
A 60-year-old patient with an infected modular tumor knee endoprosthesis develops metallosis, characterized by grayish skin discoloration and a black synovial membrane. The clinical context describes the transport of metal particles by phagocytes. Through which anatomical structures are these metal particles primarily transported to cause the skin discoloration?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context explicitly states, "The metal particles are transported by phagocytes through the lymphatic vessels; the skin has a grayish color." This describes the mechanism of how the metal particles, once phagocytosed, are carried away from the joint, eventually leading to deposition and discoloration in the skin. Arterial (A) and venous (B) circulation are primarily for blood flow, not for the transport of particulate matter by phagocytes to cause localized skin discoloration in this manner. Nerve sheaths (D) and direct tissue diffusion (E) are not the primary transport mechanisms for these particles.
Question 25
A 72-year-old female presents with chronic pain and swelling in her right knee, 4 years after a total knee arthroplasty. Radiographs reveal septic loosening of the implant, including a tilted femoral component and extensive osteolytic changes. Additionally, paraarticular ossification is noted. What is the significance of paraarticular ossification in the context of a total knee arthroplasty?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 2.56 explicitly state that "paraarticular ossification is seen as a sign of septic complication" in the context of septic loosening of a total knee replacement. While some degree of heterotopic ossification can occur post-operatively, significant or progressive paraarticular ossification in the setting of pain and other signs of infection is a strong indicator of a septic process. It is not a normal finding (A) in this context, nor does it specifically indicate aseptic loosening (B) or primary metabolic bone disease (D). It is clinically relevant (E) as a marker of infection.
Question 26
A 45-year-old female presents with progressive skin thickening and stiffness in her fingers. Biopsy of the affected skin reveals excessive collagen deposition. Which of the following cellular dysfunctions is primarily implicated in the pathological deposition of extracellular matrix in systemic sclerosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." This highlights the central role of fibroblasts in the fibrotic process. Endothelial cell dysfunction (A) is also a feature but fibroblast dysregulation is the primary cause of matrix deposition. T-lymphocyte hyperactivity (B), macrophage phagocytosis (D), and mast cell degranulation (E) are involved in the inflammatory response but not the direct cause of extracellular matrix deposition.
Question 27
A 42-year-old patient is diagnosed with systemic sclerosis after presenting with Raynaud's phenomenon and progressive skin changes. When discussing the epidemiology of this condition, which of the following statements is most accurate?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states, "Affected patients are female in 80% of the cases." The prevalence is 15/100,000, not 150/100,000 (B). While early signs can appear under age 3, skin signs generally present in the forties, not typically in childhood (C), and early signs can appear before 18 (E).
Question 28
A 50-year-old woman presents with progressively stiff and thick skin on her fingers, making it difficult to make a fist. Physical examination reveals taut, shiny skin over the digits, with some digital pitting. This specific clinical finding is best described as:

View Answer & Explanation
Correct Answer: C
Rationale: The image and clinical context describe "Sclerodactyly with thick and stiff skin of fingers." This term specifically refers to the skin thickening and tightening of the digits characteristic of scleroderma. Psoriatic dactylitis (A) involves inflammation of the entire digit but is associated with psoriasis. Dupuytren's contracture (B) is a fibrotic condition of the palmar fascia, not diffuse skin thickening. Erythema nodosum (D) and Livedo reticularis (E) are different dermatological conditions.
Question 29
A 55-year-old female with a history of systemic sclerosis complains of chronic pain and shortening of her fingers. A radiograph of her hand is obtained. Which of the following radiographic findings is commonly associated with sclerodactyly in systemic sclerosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 12.2 states, "On radiograph, resorption of distal phalanx is possible." This is a characteristic radiographic finding in advanced sclerodactyly. Periarticular erosions (B) are more typical of rheumatoid arthritis. Joint space widening (A), subchondral cysts (D), and osteophyte formation (E) are not primary or characteristic radiographic features of scleroderma.
Question 30
A 60-year-old woman with systemic sclerosis develops painful, firm nodules on her hands and elbows. Physical examination reveals palpable subcutaneous deposits. Subcutaneous calcinosis in scleroderma is typically located on which of the following surfaces?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 12.2 states that subcutaneous calcinosis "is usually located on the extensor surface of the phalanges, periarticular tissue, and over the bone prominences." The extensor surface of the phalanges is a key location. The flexor surface (A) is incorrect. While calcinosis can occur over bone prominences like the elbow, the question asks for a typical location on the phalanges.
Question 31
A 48-year-old female with systemic sclerosis reports increasing pain and stiffness in her wrists and ankles. On physical examination, a grating sensation is noted with passive range of motion over the tendons. This finding, known as a tendon friction rub, is often associated with which of the following manifestations?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 12.2 states, "Joint pain and tendon friction rub are common because of subcutaneous calcinosis, which is usually located on the extensor surface of the phalanges, periarticular tissue, and over the bone prominences." Myositis (A) and Raynaud's phenomenon (B) are other common features but not the direct cause of tendon friction rubs. Arterial hypertension (D) and glomerulonephritis (E) are systemic complications.
Question 32
A 58-year-old female with long-standing systemic sclerosis presents with new-onset shortness of breath, palpitations, and signs of heart failure. Which of the following cardiovascular complications is a known late manifestation of systemic sclerosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context lists "myocardial involvement" as a late complication of systemic sclerosis. While other cardiac issues can occur, myocardial involvement is specifically mentioned. Atrial fibrillation (A) and valvular heart disease (B) are not explicitly listed as late complications in the provided text, nor is pericarditis (D) or aortic dissection (E).
Question 33
A 62-year-old female with systemic sclerosis is admitted for acute kidney injury. Her blood pressure is significantly elevated, and urinalysis shows proteinuria. Which renal complication is specifically mentioned as a late complication of systemic sclerosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that "glomerulonephritis can appear as late complications." While renal artery involvement (B) can occur in scleroderma renal crisis, glomerulonephritis is the specific renal complication listed in the text. The other options are not mentioned as specific complications of scleroderma.
Question 34
A 65-year-old male with severe generalized scleroderma develops progressive weakness and sensory changes in his lower extremities. MRI of the spine reveals compression of the spinal cord. This rare but serious neurological complication is often due to which of the following in the context of scleroderma?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context mentions, "Rare but serious neurological complications are also known in cases of spinal involvement and spinal cord compression by calcinosis." This directly identifies calcinosis as the cause of spinal cord compression in scleroderma. The other options are general causes of spinal cord compression but are not specifically highlighted as complications of scleroderma in the text.
Question 35
A 36-year-old woman presents with a linear area of skin thickening and induration on her forehead, resembling a "saber cut." Radiographs of her elbow also show linear calcifications. This specific manifestation of scleroderma is referred to as:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 12.4 states, "On the radiograph of the elbow, linear scleroderma is also seen. It is called also “en coup de sabre”." This term specifically describes the linear form of scleroderma, often on the head or limbs, resembling a saber cut. Morphea (A) is a localized form of scleroderma, but "en coup de sabre" is the specific descriptive term for this linear presentation. Sclerodactyly (B) refers to finger involvement. CREST syndrome (D) is a limited form of systemic sclerosis, and diffuse cutaneous systemic sclerosis (E) is a generalized form.
Question 36
A 40-year-old female is diagnosed with systemic sclerosis. The underlying pathological process involves the excessive deposition of extracellular matrix in connective tissues. This process is primarily driven by altered regulation of which specific cell type?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states, "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." Dermal fibroblasts are the primary cells responsible for producing extracellular matrix components like collagen. Keratinocytes (A), melanocytes (B), adipocytes (D), and Langerhans cells (E) have different primary functions in the skin and are not the main drivers of fibrosis in scleroderma.
Question 37
A 50-year-old patient is being evaluated for suspected systemic sclerosis due to new-onset Raynaud's phenomenon and skin thickening. Which of the following is a fundamental characteristic of this syndrome as described in the provided text?
View Answer & Explanation
Correct Answer: B
Rationale: The introductory sentence of the clinical context defines scleroderma as "a syndrome... characterized by inflammation associated with fibrosis and pathological remodeling of connective tissues." This is the most accurate fundamental characteristic. It is not exclusively dermatological (C), nor does it primarily affect skeletal muscle without connective tissue involvement (A). While vasculopathy is present, it's not primarily a large vessel vasculitis (D), and it's not a congenital disorder (E).
Question 38
A 45-year-old woman presents with new onset skin thickening on her hands and face. While early signs of scleroderma can appear at a young age, skin signs generally present in which decade of life?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context states, "Early signs can appear under age of 3, but skin signs generally present in the forties." This directly answers the question about the typical decade for skin sign presentation. While early signs can be much younger, the characteristic skin changes usually manifest later.
Question 39
A 38-year-old female with systemic sclerosis reports episodic digital pallor, cyanosis, and rubor
Question 39
A 45-year-old female presents with progressive skin thickening and stiffness in her hands. Biopsy reveals excessive collagen deposition.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." Endothelial cells are involved in vascular changes, but the primary pathological deposition is fibroblast-driven.
Question 39
A 50-year-old patient is diagnosed with systemic sclerosis after presenting with Raynaud's phenomenon and sclerodactyly.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states, "Affected patients are female in 80% of the cases." While 60% represents a majority, 80% is the precise figure provided.
Question 39
A 3-year-old child is brought to the clinic by her parents who noticed unusual skin changes. A diagnosis of scleroderma is being considered.
View Answer & Explanation
Correct Answer: E
Rationale: The text mentions, "Early signs can appear under age of 3, but skin signs generally present in the forties." Childhood (B) is incorrect as it refers to early signs, not the general presentation of skin signs.
Question 39
A 55-year-old woman presents with thick and stiff skin of her fingers, consistent with sclerodactyly. She complains of chronic hand pain.
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 12.2 states, "On radiograph, resorption of distal phalanx is possible." While joint issues can occur, distal phalanx resorption is a specific and characteristic radiographic finding mentioned for sclerodactyly.
Question 39
A 60-year-old female with a history of systemic sclerosis presents with painful nodules on her hands and elbows. Physical examination reveals firm, subcutaneous deposits.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.2 specifies that subcutaneous calcinosis "is usually located on the extensor surface of the phalanges, periarticular tissue, and over the bone prominences." The flexor surface of the phalanges (A) is incorrect as calcinosis is typically on the extensor surfaces.
Question 39
A 48-year-old woman with a new diagnosis of systemic sclerosis reports episodic digital ischemia, especially in cold weather, causing her fingers to turn white, then blue, then red.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.2 explicitly states, "Myositis and Raynaud’s phenomenon are also often seen." The described symptoms are classic for Raynaud's phenomenon. Carpal tunnel syndrome (A) is a nerve compression, not a vascular phenomenon.
Question 39
A 52-year-old female with systemic sclerosis complains of pain and stiffness in her wrists and ankles. On examination, a palpable and audible grating sensation is noted with movement of the affected joints.
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 12.2 states, "Joint pain and tendon friction rub are common because of subcutaneous calcinosis." While joint crepitus (A) can occur, "tendon friction rub" is the specific term mentioned in the context of calcinosis in scleroderma.
Question 39
A 65-year-old woman with a long-standing history of severe generalized scleroderma presents with significant limitations in her hand function, unable to fully extend her fingers or wrists.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "In serious generalized forms, calcification in the subcutaneous soft tissues and contractures can be observed." Joint hypermobility (A) is contrary to the fibrotic and stiffening nature of scleroderma.
Question 39
A 70-year-old male with systemic sclerosis develops progressive weakness and sensory changes in his lower extremities. Imaging reveals a mass effect on the spinal cord.
View Answer & Explanation
Correct Answer: C
Rationale: The text notes, "Rare but serious neurological complications are also known in cases of spinal involvement and spinal cord compression by calcinosis." While disc herniation (B) is a common cause of spinal compression, calcinosis is the specific cause mentioned in the context of scleroderma.
Question 39
A 36-year-old woman with scleroderma undergoes radiographs of her elbow, which reveal a linear area of increased density in the soft tissues.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.4 states, "On the radiograph of the elbow, linear scleroderma is also seen. It is called also “en coup de sabre”." "Sunburst" appearance (A) is typically associated with osteosarcoma, not scleroderma.
Question 39
A 58-year-old female with systemic sclerosis is being evaluated for new-onset shortness of breath and peripheral edema. Her medical history includes long-standing Raynaud's phenomenon.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "Obliteration of arteries and arterioles" as a late complication. While other cardiac issues can occur, this specific vascular complication is directly mentioned. Atrial fibrillation (A) is a common arrhythmia but not specifically highlighted as a late complication of scleroderma in the text.
Question 39
A 62-year-old female with systemic sclerosis presents with rapidly worsening hypertension and elevated creatinine levels.
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "glomerulonephritis" as a late complication. Renal calculi (A) are not a specific late complication of scleroderma mentioned in the provided text.
Question 39
A 68-year-old female with a history of systemic sclerosis is undergoing a cardiac workup due to new symptoms of fatigue and exercise intolerance.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "myocardial involvement, and glomerulonephritis can appear as late complications" and also "arterial hypertension." Hypothyroidism (A) is not specifically mentioned as a late complication in the provided text.
Question 39
A research scientist is studying the pathogenesis of systemic sclerosis. Her focus is on the cellular changes leading to the characteristic fibrosis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." Keratinocytes (E) are skin cells, but fibroblasts are directly responsible for extracellular matrix deposition and fibrosis.
Question 39
A medical student is preparing a presentation on systemic sclerosis, focusing on its fundamental characteristics.
View Answer & Explanation
Correct Answer: C
Rationale: The definition of scleroderma in the text is "characterized by inflammation associated with fibrosis and pathological remodeling of connective tissues." Atrophy and necrosis (A) are not the primary defining characteristics of scleroderma's pathology.
Question 39
A 36-year-old woman presents with severe hand stiffness and difficulty with fine motor tasks. Examination reveals significant skin changes in her fingers.

View Answer & Explanation
Correct Answer: C</p
Question 40
A 45-year-old female presents with progressive skin thickening and stiffness in her hands. Biopsy reveals excessive collagen deposition.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." Endothelial cells are involved in vascular changes, but the primary pathological deposition is fibroblast-driven.
Question 41
A 50-year-old patient is diagnosed with systemic sclerosis after presenting with Raynaud's phenomenon and sclerodactyly.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states, "Affected patients are female in 80% of the cases." While 60% represents a majority, 80% is the precise figure provided.
Question 42
A 3-year-old child is brought to the clinic by her parents who noticed unusual skin changes. A diagnosis of scleroderma is being considered.
View Answer & Explanation
Correct Answer: E
Rationale: The text mentions, "Early signs can appear under age of 3, but skin signs generally present in the forties." Childhood (B) is incorrect as it refers to early signs, not the general presentation of skin signs.
Question 43
A 55-year-old woman presents with thick and stiff skin of her fingers, consistent with sclerodactyly. She complains of chronic hand pain.
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 12.2 states, "On radiograph, resorption of distal phalanx is possible." While joint issues can occur, distal phalanx resorption is a specific and characteristic radiographic finding mentioned for sclerodactyly.
Question 44
A 60-year-old female with a history of systemic sclerosis presents with painful nodules on her hands and elbows. Physical examination reveals firm, subcutaneous deposits.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.2 specifies that subcutaneous calcinosis "is usually located on the extensor surface of the phalanges, periarticular tissue, and over the bone prominences." The flexor surface of the phalanges (A) is incorrect as calcinosis is typically on the extensor surfaces.
Question 45
A 48-year-old woman with a new diagnosis of systemic sclerosis reports episodic digital ischemia, especially in cold weather, causing her fingers to turn white, then blue, then red.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.2 explicitly states, "Myositis and Raynaud’s phenomenon are also often seen." The described symptoms are classic for Raynaud's phenomenon. Carpal tunnel syndrome (A) is a nerve compression, not a vascular phenomenon.
Question 46
A 52-year-old female with systemic sclerosis complains of pain and stiffness in her wrists and ankles. On examination, a palpable and audible grating sensation is noted with movement of the affected joints.
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 12.2 states, "Joint pain and tendon friction rub are common because of subcutaneous calcinosis." While joint crepitus (A) can occur, "tendon friction rub" is the specific term mentioned in the context of calcinosis in scleroderma.
Question 47
A 65-year-old woman with a long-standing history of severe generalized scleroderma presents with significant limitations in her hand function, unable to fully extend her fingers or wrists.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "In serious generalized forms, calcification in the subcutaneous soft tissues and contractures can be observed." Joint hypermobility (A) is contrary to the fibrotic and stiffening nature of scleroderma.
Question 48
A 70-year-old male with systemic sclerosis develops progressive weakness and sensory changes in his lower extremities. Imaging reveals a mass effect on the spinal cord.
View Answer & Explanation
Correct Answer: C
Rationale: The text notes, "Rare but serious neurological complications are also known in cases of spinal involvement and spinal cord compression by calcinosis." While disc herniation (B) is a common cause of spinal compression, calcinosis is the specific cause mentioned in the context of scleroderma.
Question 49
A 36-year-old woman with scleroderma undergoes radiographs of her elbow, which reveal a linear area of increased density in the soft tissues.
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 12.4 states, "On the radiograph of the elbow, linear scleroderma is also seen. It is called also “en coup de sabre”." "Sunburst" appearance (A) is typically associated with osteosarcoma, not scleroderma.
Question 50
A 58-year-old female with systemic sclerosis is being evaluated for new-onset shortness of breath and peripheral edema. Her medical history includes long-standing Raynaud's phenomenon.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "Obliteration of arteries and arterioles" as a late complication. While other cardiac issues can occur, this specific vascular complication is directly mentioned. Atrial fibrillation (A) is a common arrhythmia but not specifically highlighted as a late complication of scleroderma in the text.
Question 51
A 62-year-old female with systemic sclerosis presents with rapidly worsening hypertension and elevated creatinine levels.
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "glomerulonephritis" as a late complication. Renal calculi (A) are not a specific late complication of scleroderma mentioned in the provided text.
Question 52
A 68-year-old female with a history of systemic sclerosis is undergoing a cardiac workup due to new symptoms of fatigue and exercise intolerance.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "myocardial involvement, and glomerulonephritis can appear as late complications" and also "arterial hypertension." Hypothyroidism (A) is not specifically mentioned as a late complication in the provided text.
Question 53
A research scientist is studying the pathogenesis of systemic sclerosis. Her focus is on the cellular changes leading to the characteristic fibrosis.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Pathological deposition of extracellular matrix in systemic sclerosis is most probably caused by changes in the regulation of dermal fibroblasts." Keratinocytes (E) are skin cells, but fibroblasts are directly responsible for extracellular matrix deposition and fibrosis.
Question 54
A medical student is preparing a presentation on systemic sclerosis, focusing on its fundamental characteristics.
View Answer & Explanation
Correct Answer: C
Rationale: The definition of scleroderma in the text is "characterized by inflammation associated with fibrosis and pathological remodeling of connective tissues." Atrophy and necrosis (A) are not the primary defining characteristics of scleroderma's pathology.
Question 55
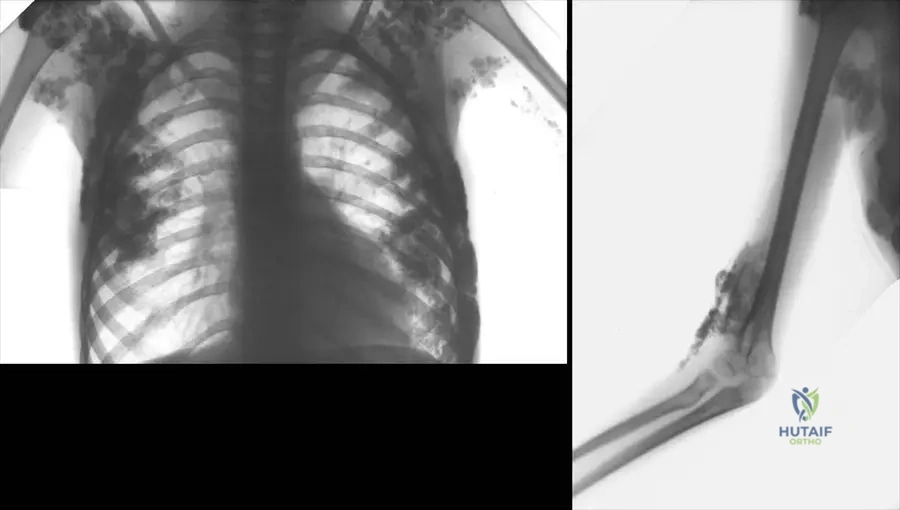
A 5-year-old boy presents with a 3-month history of localized pain and swelling over his left parietal skull. Physical examination reveals a tender, palpable mass. Radiographs of the skull show a well-demarcated, lytic lesion with beveled edges and no significant periosteal reaction. There are no other skeletal lesions identified on skeletal survey.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation and radiographic findings are highly suggestive of Langerhans Cell Histiocytosis (LCH), specifically eosinophilic granuloma (solitary bone lesion). While intralesional steroids can be effective, a definitive diagnosis requires biopsy. Open biopsy and curettage not only provide tissue for diagnosis but also serve as a therapeutic intervention for solitary, accessible lesions. Observation is not appropriate given the symptomatic nature and need for diagnosis. Systemic chemotherapy is reserved for multifocal or systemic disease. Radiation therapy is typically used for inaccessible lesions, recurrent disease, or those unresponsive to other treatments.
Question 56
A 7-year-old girl presents with a 2-month history of back pain. Physical examination reveals tenderness over the T8 spinous process. Neurological examination is normal. Radiographs of the thoracic spine show a flattened vertebral body (vertebra plana) at T8. MRI confirms the T8 vertebral body collapse without significant spinal canal compromise. A biopsy of the lesion is performed.
View Answer & Explanation
Correct Answer: D
Rationale: Vertebra plana, or a flattened vertebral body, in a child is highly characteristic of Langerhans Cell Histiocytosis (LCH), specifically eosinophilic granuloma. While other conditions can cause vertebral collapse, LCH is the classic cause of vertebra plana in this age group. Ewing sarcoma typically presents as a more aggressive lytic lesion with soft tissue mass. Osteomyelitis would show signs of infection and often less complete collapse. Aneurysmal bone cysts are expansile and rarely cause complete vertebra plana. Osteoid osteoma is a sclerotic lesion with a nidus, not a lytic collapse.
Question 57
A 4-year-old boy undergoes a biopsy for a lytic lesion in his proximal femur. Histopathological examination reveals a proliferation of histiocyte-like cells mixed with eosinophils, lymphocytes, and plasma cells. Immunohistochemical staining is performed to confirm the diagnosis.
View Answer & Explanation
Correct Answer: C
Rationale: Langerhans Cell Histiocytosis (LCH) is characterized by the proliferation of Langerhans cells, which are antigen-presenting cells. These cells are typically positive for S100 protein and CD1a on immunohistochemical staining. The presence of Birbeck granules on electron microscopy is also pathognomonic. CD30 is associated with anaplastic large cell lymphoma. CD20 is a B-cell marker. Factor VIII is a marker for endothelial cells. HMB-45 is a marker for melanoma.
Question 58
A 6-year-old girl is diagnosed with a solitary, asymptomatic lytic lesion in her distal tibia consistent with Langerhans Cell Histiocytosis after an incidental finding on radiographs for an unrelated injury. The lesion is non-weight-bearing and not causing any pain or functional deficit. A biopsy confirmed the diagnosis.
View Answer & Explanation
Correct Answer: D
Rationale: For asymptomatic, solitary bone lesions of Langerhans Cell Histiocytosis (eosinophilic granuloma) that are not in a critical weight-bearing location and have been definitively diagnosed, observation with serial radiographs is a reasonable initial management strategy. Many such lesions can spontaneously regress. Surgical curettage, intralesional steroids, or radiation are typically reserved for symptomatic lesions, lesions in critical locations, or those that progress. Systemic chemotherapy is for multifocal or systemic disease.
Question 59
A 2-year-old boy presents with a 6-month history of recurrent ear discharge, scalp rash, and irritability. Physical examination reveals otitis externa, seborrheic dermatitis-like rash on the scalp, and hepatosplenomegaly. Skeletal survey shows multiple lytic lesions in the skull and long bones. Biopsy confirms Langerhans Cell Histiocytosis.
View Answer & Explanation
Correct Answer: D
Rationale: This patient presents with involvement of multiple organ systems (skin, ear, liver/spleen, and multiple bones). This constitutes multisystem disease, which is the most severe form of Langerhans Cell Histiocytosis and requires systemic treatment. Solitary bone lesion is a single lesion in one bone. Multifocal bone disease involves multiple bone lesions but no other organ involvement. Single system, multifocal disease refers to multiple lesions within one organ system (e.g., multiple bone lesions). Hand-Schüller-Christian disease is a historical term for a specific triad (exophthalmos, diabetes insipidus, lytic skull lesions) which is now classified under multisystem LCH.
Question 60
A 10-year-old boy presents with a 4-week history of pain and swelling in his right humerus. Radiographs show an expansile, lytic lesion with a "soap bubble" appearance and thin periosteal reaction. There is no evidence of a soft tissue mass. A biopsy is planned.
View Answer & Explanation
Correct Answer: C
Rationale: While Langerhans Cell Histiocytosis can present as a lytic lesion, the description of an "expansile, soap bubble" appearance is highly characteristic of an aneurysmal bone cyst (ABC). ABCs are often expansile and can have a thin periosteal reaction. Osteosarcoma typically presents with a more aggressive, destructive pattern and often a soft tissue mass. Fibrous dysplasia has a ground-glass appearance. Chronic osteomyelitis can be lytic but often has sequestra and involucrum. LCH lesions are typically purely lytic and less expansile than ABCs, though they can mimic many lesions.
Question 61
A 3-year-old girl is diagnosed with Langerhans Cell Histiocytosis affecting the T6 vertebral body, resulting in vertebra plana. She is asymptomatic with no neurological deficits. The lesion was confirmed by biopsy. What is the most appropriate initial management?
View Answer & Explanation
Correct Answer: B
Rationale: For vertebra plana due to Langerhans Cell Histiocytosis without neurological compromise, bracing and observation is often the initial treatment of choice. The vertebral body often remodels and reconstitutes over time, especially in younger children. Surgical stabilization is reserved for progressive deformity, instability, or neurological deficits. Systemic chemotherapy is for multifocal or multisystem disease. Radiation therapy is typically for lesions unresponsive to other treatments or with neurological compromise. Intralesional steroids are difficult to administer safely and effectively in the spine.
Question 62
A 1-year-old infant presents with a rapidly growing, tender mass in the right femur. Radiographs show an aggressive lytic lesion with cortical destruction and a large soft tissue component. Biopsy reveals a proliferation of histiocytes with positive staining for CD1a and S100. Electron microscopy shows Birbeck granules. Further workup reveals no other lesions.
View Answer & Explanation
Correct Answer: A
Rationale: Birbeck granules (also known as Langerhans cell granules) are rod-shaped or tennis-racket-shaped organelles found in Langerhans cells and are considered pathognomonic for Langerhans Cell Histiocytosis (LCH) on electron microscopy. While the lesion is aggressive, it is described as a single lesion with no other involvement, making it a solitary bone lesion (eosinophilic granuloma), not necessarily requiring systemic chemotherapy unless it progresses or is in a critical location. Diabetes insipidus is a complication of skull base or pituitary involvement, not typically a direct risk from a solitary femur lesion. Spontaneous regression is possible for less aggressive, asymptomatic lesions, but a rapidly growing, tender lesion warrants intervention.
Question 63
A 14-year-old boy presents with a 6-month history of persistent pain in his left iliac wing. Radiographs show a large, ill-defined lytic lesion. A biopsy confirms Langerhans Cell Histiocytosis. Considering the typical epidemiology of LCH, which age group is most commonly affected by solitary bone lesions?
View Answer & Explanation
Correct Answer: C
Rationale: Langerhans Cell Histiocytosis, particularly the solitary bone lesion form (eosinophilic granuloma), most commonly affects children between 5 and 10 years of age. While it can occur at any age, this is the peak incidence for the localized form. Infants and toddlers are more prone to multifocal or multisystem disease. Adolescents and young adults can also be affected, but less commonly than young children.
Question 64
A 6-year-old boy is diagnosed with a solitary lytic lesion in his right femur, confirmed as Langerhans Cell Histiocytosis. He undergoes curettage and bone grafting. What is the expected prognosis for a solitary bone lesion of LCH?
View Answer & Explanation
Correct Answer: C
Rationale: Solitary bone lesions of Langerhans Cell Histiocytosis (eosinophilic granuloma) generally have an excellent prognosis. The vast majority resolve with local treatment or even observation, and the recurrence rate is relatively low (around 10-20%). Malignant transformation is exceedingly rare. Progression to multisystem disease is uncommon for truly solitary lesions. Diabetes insipidus is a complication of skull base involvement, not typical for a solitary femur lesion. Lifelong systemic chemotherapy is not required for solitary bone disease.
Question 65
A 2-year-old girl presents with multiple lytic lesions in her skull, ribs, and femurs, along with a persistent rash and mild hepatomegaly. Biopsy confirms Langerhans Cell Histiocytosis. What is the most appropriate initial treatment strategy?
View Answer & Explanation
Correct Answer: C
Rationale: This patient has multisystem Langerhans Cell Histiocytosis (multiple bone lesions plus skin rash and hepatomegaly). Multisystem disease, especially in younger children, requires systemic chemotherapy to control the disease and prevent further organ damage. Localized treatments like curettage, radiation, or intralesional steroids are insufficient for widespread disease. Observation is not appropriate for active, multisystem LCH.
Question 66
A 5-year-old boy with a history of Langerhans Cell Histiocytosis involving the skull base and sella turcica presents with increased thirst and frequent urination. Laboratory tests reveal elevated serum osmolality and decreased urine osmolality, which improves with desmopressin administration.
View Answer & Explanation
Correct Answer: B
Rationale: The symptoms of increased thirst (polydipsia) and frequent urination (polyuria), along with laboratory findings of elevated serum osmolality and decreased urine osmolality, responsive to desmopressin, are classic signs of diabetes insipidus. This is a common complication of Langerhans Cell Histiocytosis when it involves the hypothalamus or pituitary gland, particularly the posterior pituitary, which is responsible for antidiuretic hormone (ADH) production. While other endocrine dysfunctions can occur, diabetes insipidus is specifically indicated by these symptoms and test results.
Question 67
A 7-year-old girl presents with persistent pain in her left hip. Plain radiographs show a lytic lesion in the femoral neck. After biopsy confirms Langerhans Cell Histiocytosis, the orthopaedic surgeon wants to assess the full extent of skeletal involvement and rule out other systemic disease. Which imaging modality is most appropriate for a comprehensive skeletal survey?
View Answer & Explanation
Correct Answer: E
Rationale: Whole-body MRI is increasingly recognized as the most sensitive and comprehensive imaging modality for detecting skeletal lesions in Langerhans Cell Histiocytosis, especially for multifocal disease, and can also detect soft tissue involvement. While Technetium-99m bone scans can detect some lesions, they often miss purely lytic lesions or those with minimal osteoblastic activity, which is common in LCH. CT scans are good for specific areas but not for a whole-body survey. PET-CT can be useful but may not be as sensitive for purely lytic bone lesions as MRI and involves radiation. MRI of the spine alone would miss other skeletal sites.
Question 68
A 9-year-old boy underwent curettage for a solitary Langerhans Cell Histiocytosis lesion in his distal radius 1 year ago. He now presents with new pain at the same site. Radiographs show a recurrent lytic lesion. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: B
Rationale: For a local recurrence of a solitary bone lesion of Langerhans Cell Histiocytosis, repeat curettage, often combined with an intralesional corticosteroid injection, is a common and effective treatment. This approach aims to control the local disease without resorting to more aggressive systemic therapies. Systemic chemotherapy is typically reserved for multifocal or multisystem disease. Observation is not appropriate for a symptomatic, recurrent lesion. Low-dose radiation therapy is an option for recurrent or inaccessible lesions but is often considered after repeat local intervention. Biopsy of a new distant site would be indicated if there were suspicion of new lesions, but the question specifies recurrence at the *same* site.
Question 69
A 4-year-old girl is diagnosed with Langerhans Cell Histiocytosis affecting her left femur. The underlying pathophysiology involves a clonal proliferation of which cell type?
View Answer & Explanation
Correct Answer: C
Rationale: Langerhans Cell Histiocytosis (LCH) is characterized by the clonal proliferation of Langerhans cells, which are immature dendritic cells of myeloid origin. While other inflammatory cells like eosinophils, lymphocytes, and plasma cells are often present in the lesions, the primary neoplastic cell is the Langerhans cell. Osteoblasts and osteoclasts are involved in normal bone remodeling, and plasma cells and eosinophils are part of the inflammatory response but are not the primary proliferating cell in LCH.
Question 70
A 6-year-old boy presents with a painful lytic lesion in his right proximal humerus, confirmed as Langerhans Cell Histiocytosis. The lesion is causing significant pain and limiting shoulder movement. There is no evidence of other lesions on skeletal survey.
View Answer & Explanation
Correct Answer: C
Rationale: For a symptomatic, solitary bone lesion of Langerhans Cell Histiocytosis, intralesional corticosteroid injection is a well-established and effective treatment option, particularly for accessible lesions. It can reduce pain and promote healing. Observation is not appropriate for a painful, symptomatic lesion. Systemic chemotherapy is for multifocal or multisystem disease. Radiation therapy is an option for inaccessible or recurrent lesions but often reserved due to potential long-term side effects. Surgical resection and reconstruction are typically overly aggressive for a benign LCH lesion, unless there is significant bone destruction or impending fracture.
Question 71
A 1-year-old infant presents with a diffuse papular rash, hepatosplenomegaly, and multiple lytic bone lesions. Biopsy of a skin lesion shows histiocytic infiltration. The patient is diagnosed with Langerhans Cell Histiocytosis. Which of the following is a key distinguishing feature of LCH from other non-Langerhans cell histiocytoses?
View Answer & Explanation
Correct Answer: D
Rationale: The definitive diagnostic markers for Langerhans Cell Histiocytosis are positive immunohistochemical staining for CD1a and S100 protein, which identify the Langerhans cells. While other histiocytoses may have foam cells or be positive for CD68 (a general histiocyte marker), these are not specific to LCH. Eosinophils are often present in LCH lesions (especially eosinophilic granuloma). While LCH can rarely be associated with HLH, it is not a distinguishing feature of LCH itself from other histiocytoses; rather, it's a potential complication or co-occurrence.
Question 72
A 3-year-old boy with multisystem Langerhans Cell Histiocytosis involving bone, skin, and liver is undergoing systemic chemotherapy with vinblastine and prednisone. After 6 months of treatment, his bone lesions have healed, skin rash has resolved, and liver function tests are normal. What is the typical duration of systemic therapy for multisystem LCH?
View Answer & Explanation
Correct Answer: C
Rationale: For multisystem Langerhans Cell Histiocytosis, standard treatment protocols (e.g., LCH-III, LCH-IV) typically involve systemic chemotherapy for a duration of 12 months. This includes an induction phase followed by a maintenance phase. While some patients may respond earlier, a full 12-month course is generally recommended to minimize recurrence and ensure complete disease control. Shorter durations may lead to higher relapse rates. Lifelong therapy is not typically required.
Question 73
A 7-year-old girl was treated for a large Langerhans Cell Histiocytosis lesion in her left proximal femur with curettage and low-dose radiation therapy at age 3. She now presents with a leg length discrepancy and angular deformity of the left femur. What is the most likely cause of these long-term sequelae?
View Answer & Explanation
Correct Answer: C
Rationale: Radiation therapy, especially in young children and near growth plates, can cause significant damage to the physis, leading to growth disturbance, leg length discrepancy, and angular deformities. This is a known long-term complication of radiation therapy for bone lesions in children. While recurrence is possible, it typically presents as pain and a new lytic lesion, not primarily as growth disturbance. Malignant transformation is exceedingly rare. Pathological fracture is an acute event, not a chronic growth problem. Avascular necrosis can occur but is less directly linked to radiation of the proximal femur than growth plate damage.
Question 74
A 5-year-old boy presents with a 3-month history of a painful lump on his scalp. Radiographs show a well-defined lytic lesion in the parietal bone. A biopsy confirms Langerhans Cell Histiocytosis. Which of the following skeletal sites is most commonly affected by LCH?
View Answer & Explanation
Correct Answer: D
Rationale: The skull is the most common skeletal site for Langerhans Cell Histiocytosis, accounting for approximately 50-60% of all bone lesions. Other common sites include the vertebrae, long bones, pelvis, and ribs, but the skull is the most frequently involved. This is consistent with the vignette describing a parietal bone lesion.
Question 75
A 3-year-old boy presents with a several-month history of a palpable, non-tender mass on his scalp. Physical examination reveals a 2 cm firm, fixed lesion over the parietal bone. Radiographs demonstrate a solitary, well-demarcated lytic lesion in the parietal bone without sclerotic margins. There are no other systemic symptoms or findings. Which of the following is the most common site for solitary bone lesions in Langerhans Cell Histiocytosis (LCH)?
View Answer & Explanation
Correct Answer: C
Rationale: The skull is the most common site for solitary bone lesions in Langerhans Cell Histiocytosis, accounting for approximately 50-60% of cases. Other common sites include the long bones, pelvis, and vertebrae, but less frequently than the skull. Main Distractor: A) Femur is a common site for long bone involvement, but overall less frequent than the skull.
Question 76
A 5-year-old girl undergoes a biopsy of a lytic lesion in her proximal humerus. Histopathological examination reveals a proliferation of large, mononuclear cells with abundant eosinophilic cytoplasm and characteristic reniform nuclei, interspersed with eosinophils, lymphocytes, and plasma cells. Immunohistochemical staining is positive for CD1a and S100. Which cell type is pathognomonic for Langerhans Cell Histiocytosis?
View Answer & Explanation
Correct Answer: C
Rationale: Langerhans Cell Histiocytosis is characterized by the proliferation of pathological Langerhans cells, which are a type of dendritic cell. These cells are identified by their characteristic morphology (reniform nuclei, abundant cytoplasm) and specific immunohistochemical markers like CD1a, S100, and Langerin (CD207), the latter of which identifies Birbeck granules on electron microscopy. Main Distractor: A) Macrophages are often present in inflammatory lesions, but the specific morphology and immunophenotype of Langerhans cells distinguish LCH.
Question 77
A 2-year-old boy presents with a tender, palpable mass on his forehead. Radiographs of the skull reveal a sharply demarcated lytic lesion in the frontal bone. On closer inspection, the lesion demonstrates a "hole-within-a-hole" appearance due to differential destruction of the inner and outer tables of the skull. This radiographic finding is highly suggestive of Langerhans Cell Histiocytosis and is known as which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The "beveled edge sign" or "hole-within-a-hole" appearance is a classic radiographic finding in Langerhans Cell Histiocytosis affecting the skull. It results from the differential destruction of the inner and outer tables of the skull, creating an appearance of one lytic lesion superimposed on a larger one. Main Distractor: A) Sunburst appearance and B) Codman's triangle are typically associated with aggressive bone tumors like osteosarcoma. D) Hair-on-end appearance is seen in chronic hemolytic anemias, and E) Onion skinning is characteristic of Ewing sarcoma.
Question 78
A 4-year-old girl presents with progressive back pain and a limping gait. Physical examination reveals tenderness over the thoracic spine. Radiographs of the spine show a complete collapse of a single vertebral body, resulting in a flattened appearance. This characteristic finding, often associated with Langerhans Cell Histiocytosis, is best described as which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: Vertebra plana, or a "pancake vertebra," is a classic radiographic finding in Langerhans Cell Histiocytosis affecting the spine. It describes the complete collapse of a vertebral body, often without significant neurological compromise, which can spontaneously re-ossify over time. Main Distractor: D) Kyphosis can be a secondary deformity, but vertebra plana describes the primary vertebral body collapse. A) Spondylolisthesis, B) Scoliosis, and E) Schmorl's node are different spinal pathologies.
Question 79
A 6-year-old boy presents with a 3-month history of pain and swelling in his left distal femur. Radiographs show a lytic lesion with ill-defined margins and some periosteal reaction. Given the suspicion of Langerhans Cell Histiocytosis, which of the following is the most appropriate initial diagnostic step?
View Answer & Explanation
Correct Answer: B
Rationale: The definitive diagnosis of Langerhans Cell Histiocytosis requires a tissue biopsy of the affected lesion. An open surgical biopsy or core needle biopsy is necessary to obtain sufficient tissue for histopathological examination and immunohistochemical staining (CD1a, S100, CD207). Main Distractor: A) Bone marrow biopsy is part of the staging workup for multifocal or multi-system disease but is not the initial diagnostic step for a solitary bone lesion. C) PET scan and D) MRI of the entire spine are imaging modalities used for staging and assessing disease extent, not for initial diagnosis. E) Observation is inappropriate given the need for definitive diagnosis and treatment.
Question 80
A 7-year-old girl undergoes a biopsy of a lytic lesion in her ilium. Microscopic examination reveals a characteristic infiltrate. Which of the following is a key histological feature seen in Langerhans Cell Histiocytosis?
View Answer & Explanation
Correct Answer: C
Rationale: The hallmark histological feature of Langerhans Cell Histiocytosis is the proliferation of pathological Langerhans cells, which are often accompanied by a variable inflammatory infiltrate, most notably eosinophils. Lymphocytes, plasma cells, and neutrophils may also be present. Main Distractor: A) Sheets of small round blue cells are characteristic of Ewing sarcoma. B) Spindle cells in a storiform pattern are seen in fibrous histiocytoma. D) Chondrocytes in a myxoid matrix are typical of chondrosarcoma. E) Atypical osteoblasts forming osteoid are characteristic of osteosarcoma.
Question 81
A biopsy of a lytic lesion in a 1-year-old infant's tibia confirms Langerhans Cell Histiocytosis. To further characterize the cells and confirm the diagnosis, immunohistochemical staining is performed. Which of the following markers is most specific for Langerhans cells and their characteristic Birbeck granules?
View Answer & Explanation
Correct Answer: C
Rationale: CD1a is a highly sensitive and specific immunohistochemical marker for Langerhans cells. It is expressed on the cell surface and is crucial for confirming the diagnosis of LCH. Langerin (CD207) is another highly specific marker, as it is a component of Birbeck granules, which are characteristic organelles of Langerhans cells seen on electron microscopy. S100 is also positive but less specific. Main Distractor: E) CD68 is a marker for macrophages, which can be present in the lesion but are not the pathognomonic cell type. A) CD3 is a T-cell marker, B) CD20 is a B-cell marker, and D) CD34 is a hematopoietic stem cell marker.
Question 82
A 9-month-old infant is diagnosed with Langerhans Cell Histiocytosis. Initial staging reveals multiple lytic bone lesions, skin rash, and hepatosplenomegaly. Blood tests show mild anemia and thrombocytopenia. In the context of LCH, which of the following organs are considered "risk organs" due to their critical function and poorer prognosis when involved?
View Answer & Explanation
Correct Answer: B
Rationale: In Langerhans Cell Histiocytosis, the "risk organs" are the liver, spleen, and hematopoietic system (bone marrow). Involvement of these organs, especially in young children, is associated with a higher risk of treatment failure and mortality. Main Distractor: A) Skin, lymph nodes, and bone are common sites of involvement but are generally not considered "risk organs" in terms of immediate life-threatening complications, although extensive involvement can be problematic. C, D, E are other organs that can be involved, but B lists the classic "risk organs."
Question 83
A 4-year-old boy is diagnosed with a solitary lytic lesion in his right femur, confirmed by biopsy as Langerhans Cell Histiocytosis. There is no evidence of other bone lesions or systemic involvement. The lesion is causing mild pain but no functional deficit or impending fracture. Which of the following is the most appropriate initial management strategy for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: For solitary bone lesions of Langerhans Cell Histiocytosis, local treatment options are often sufficient. These include intralesional corticosteroid injection, curettage (with or without bone grafting), or simple observation if asymptomatic and non-weight-bearing. These methods aim to resolve the lesion locally with minimal invasiveness. Main Distractor: A) Systemic chemotherapy is reserved for multifocal or multi-system disease. B) Radiation therapy is generally avoided in children due to long-term risks but can be considered for inaccessible or refractory lesions. E) While observation is an option for asymptomatic, non-critical lesions, the presence of mild pain often warrants intervention. Amputation (D) is never indicated for LCH.
Question 84
A 3-year-old girl presents with a 2-month history of progressive back pain. Radiographs show a collapsed T8 vertebral body (vertebra plana) consistent with Langerhans Cell Histiocytosis. She has no neurological deficits. What is the most appropriate management approach for this spinal lesion?
View Answer & Explanation
Correct Answer: C
Rationale: For vertebra plana due to Langerhans Cell Histiocytosis, especially in the absence of neurological deficits, conservative management with bracing and observation is often sufficient. The vertebral body often spontaneously re-ossifies and remodels over time. Surgical intervention is reserved for cases with neurological compromise or progressive deformity. Main Distractor: A) Immediate surgical stabilization is typically not indicated unless there is neurological compromise or severe instability. B) Systemic chemotherapy is used for multifocal or multi-system disease, not typically for an isolated, asymptomatic vertebra plana. D) Radiation therapy is generally avoided in the spine due to risks to growth and surrounding tissues. E) Vertebroplasty is not a standard treatment for LCH in children.
Question 85
A 6-year-old boy is diagnosed with multifocal bone Langerhans Cell Histiocytosis, with lytic lesions identified in the skull, left humerus, and right tibia. A thorough workup, including bone marrow biopsy and imaging of risk organs, shows no evidence of systemic involvement beyond the bones. Which of the following is the most appropriate treatment strategy?
View Answer & Explanation
Correct Answer: B
Rationale: For multifocal bone Langerhans Cell Histiocytosis without risk organ involvement, systemic chemotherapy is the standard of care. This approach aims to treat all existing lesions and prevent the development of new ones. Common regimens include vinblastine and corticosteroids. Main Distractor: A) Local curettage or D) intralesional steroid injections are suitable for solitary or a very limited number of accessible lesions, but impractical and insufficient for multifocal disease. C) Radiation therapy is generally reserved for refractory or inaccessible lesions. E) Observation is not appropriate for multifocal disease, which requires active treatment.
Question 86
A 1-year-old infant presents with a diffuse skin rash, hepatosplenomegaly, and multiple lytic bone lesions. Biopsy confirms Langerhans Cell Histiocytosis. Laboratory tests reveal elevated liver enzymes and mild pancytopenia. This presentation indicates multi-system LCH with risk organ involvement. What is the cornerstone of treatment for this severe form of LCH?
View Answer & Explanation
Correct Answer: C
Rationale: Multi-system Langerhans Cell Histiocytosis, especially with risk organ involvement (liver, spleen, hematopoietic system), is a severe and potentially life-threatening condition. The cornerstone of treatment is systemic multi-agent chemotherapy, typically involving vinblastine and corticosteroids, often for an extended duration. Main Distractor: A) Local surgical excision is not feasible or effective for multi-system disease. B) High-dose radiation therapy is not the primary treatment and carries significant risks in infants. D) Immunosuppressive therapy is not the standard first-line treatment. E) Allogeneic hematopoietic stem cell transplantation is a salvage therapy for refractory or relapsed high-risk LCH, not initial treatment.
Question 87
A 7-year-old boy with a history of multi-system Langerhans Cell Histiocytosis, which included involvement of the skull base and pituitary region, is now in remission. However, his parents report that he has developed excessive thirst and frequent urination, even at night. Laboratory tests reveal hypernatremia and dilute urine. Which of the following is the most likely long-term complication of LCH in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Diabetes insipidus (DI) is the most common long-term endocrine complication of Langerhans Cell Histiocytosis, particularly when there is involvement of the skull base, sella turcica, or hypothalamus-pituitary axis. It results from damage to the posterior pituitary, leading to insufficient antidiuretic hormone (ADH) production. The symptoms of polyuria and polydipsia are classic for DI. Main Distractor: B) Growth hormone deficiency is another common endocrine complication, but the symptoms described (polyuria, polydipsia) are specific to DI. A) Hypothyroidism, D) Adrenal insufficiency, and E) Precocious puberty can also occur but are less common than DI and do not present with these specific symptoms.
Question 88
A 10-year-old girl with a history of multi-system Langerhans Cell Histiocytosis, including central nervous system involvement, is now experiencing progressive ataxia, dysarthria, and cognitive decline, despite being in remission from her systemic disease. MRI of the brain shows cerebellar atrophy and white matter changes. This clinical picture is most consistent with which of the following long-term complications of LCH?
View Answer & Explanation
Correct Answer: C
Rationale: Neurodegenerative Langerhans Cell Histiocytosis (ND-LCH) is a severe and progressive long-term complication, particularly in patients with CNS involvement. It is characterized by progressive neurological symptoms such as ataxia, dysarthria, spasticity, and cognitive decline, often with characteristic MRI findings of cerebellar atrophy and white matter lesions. It can occur years after the initial diagnosis and treatment of systemic LCH. Main Distractor: E) Brain tumor recurrence is a possibility, but the progressive, diffuse neurological symptoms and specific MRI findings are more indicative of neurodegeneration rather than a focal tumor recurrence. A) Stroke, B) Epilepsy, and D) Hydrocephalus are less typical presentations for this specific constellation of symptoms in LCH.
Question 89
A 5-year-old boy presents with a lytic lesion in his frontal bone. Radiographs show a well-demarcated lesion with a sclerotic rim. While Langerhans Cell Histiocytosis is a strong consideration, which of the following is an important differential diagnosis for a solitary lytic skull lesion in a child?
View Answer & Explanation
Correct Answer: C
Rationale: Epidermoid cysts (or dermoid cysts) are benign congenital lesions that can present as solitary lytic lesions in the skull, often with a sclerotic rim, making them an important differential diagnosis for LCH. Other considerations include fibrous dysplasia, osteoma, and rarely, metastatic neuroblastoma. Main Distractor: A) Osteosarcoma and B) Ewing sarcoma are malignant bone tumors but typically present with more aggressive features (e.g., periosteal reaction, soft tissue mass) and are less common in the skull as primary lesions. D) Chondrosarcoma is rare in children. E) Multiple myeloma is a plasma cell malignancy primarily affecting older adults.
Question 90
A 2-year-old child is diagnosed with Langerhans Cell Histiocytosis. The prognosis and treatment intensity are largely determined by the extent of disease. Which of the following factors is considered the most important prognostic indicator in LCH?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of risk organ involvement (liver, spleen, hematopoietic system) is the most important prognostic indicator in Langerhans Cell Histiocytosis. Patients with risk organ involvement, especially infants, have a significantly poorer prognosis and require more intensive systemic chemotherapy. Main Distractor: A) Age at diagnosis is also an important factor, with younger age (especially <2 years) being associated with a worse prognosis, but risk organ involvement is generally considered the primary determinant of outcome. B) The number of bone lesions indicates multifocal disease, which requires systemic treatment, but risk organ involvement carries a higher mortality risk. D) Location of bone lesions is less critical than systemic involvement. E) Serum calcium levels are not a primary prognostic indicator.
Question 91
Recent advances in the understanding of Langerhans Cell Histiocytosis have identified recurrent genetic mutations in a significant proportion of patients. Which of the following genes is most commonly mutated in LCH, leading to constitutive activation of the MAPK pathway?
View Answer & Explanation
Correct Answer: B
Rationale: The BRAF V600E mutation is the most common genetic alteration found in Langerhans Cell Histiocytosis, present in approximately 50-60% of cases. This mutation leads to constitutive activation of the MAPK (mitogen-activated protein kinase) signaling pathway, which drives the proliferation and survival of LCH cells. Detection of this mutation has opened avenues for targeted therapies. Main Distractor: D) KRAS is another gene in the MAPK pathway that can be mutated in LCH, but BRAF V600E is significantly more common. A) TP53, C) RET, and E) MYC are oncogenes or tumor suppressor genes associated with other cancers but are not the primary drivers in LCH.
Question 92
A 45-year-old male presents with chronic cough, dyspnea, and a lytic lesion in his rib. Biopsy of the rib lesion confirms Langerhans Cell Histiocytosis. What is a key difference in the presentation or prognosis of LCH in adults compared to children?
View Answer & Explanation
Correct Answer: B
Rationale: In adults, pulmonary Langerhans Cell Histiocytosis (PLCH) is a distinct entity, often strongly associated with smoking, and is the most common form of LCH in adults. While bone lesions can occur, pulmonary involvement is a more prominent feature in adult LCH compared to pediatric LCH. Main Distractor: A) Children, especially infants, are more prone to multi-system disease with risk organ involvement. D) The prognosis for adult LCH is variable; while some forms like PLCH can be chronic, overall mortality is lower than for high-risk pediatric LCH. C) Solitary bone lesions can occur in adults, though less frequently than in children. E) Diabetes insipidus can occur in adults with LCH, especially with CNS involvement, though it might be less frequent than in pediatric LCH with skull base involvement.
Question 93
A 48-year-old female presents with a 3-year history of progressive skin thickening and stiffness, initially in her fingers and hands, now extending to her forearms. She reports difficulty making a fist and frequent episodes of painful, cold-induced digital blanching. Physical examination reveals taut, shiny skin over her hands and fingers, with limited range of motion at the MCP and PIP joints. Radiographs of the hands show soft tissue thickening and early periarticular erosions.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of progressive skin thickening (sclerodactyly), Raynaud's phenomenon (cold-induced digital blanching), and joint stiffness is highly characteristic of systemic sclerosis (scleroderma). Rheumatoid arthritis typically presents with symmetric polyarthritis and morning stiffness, but less prominent skin thickening. Psoriatic arthritis involves skin psoriasis and dactylitis, but not the diffuse skin changes described. Systemic lupus erythematosus has diverse manifestations but not typically progressive skin thickening as the primary complaint. Osteoarthritis is a degenerative condition without inflammatory or autoimmune skin features. Main Distractor: A) Rheumatoid arthritis can cause joint pain and stiffness, but the prominent skin thickening and Raynaud's phenomenon are not typical primary features.
Question 94
A 55-year-old female with a known history of systemic sclerosis complains of increasing difficulty with fine motor tasks and hand hygiene. On examination, her fingers appear tapered and stiff, with a "bound-down" quality of the skin, making it difficult to pinch or grasp objects. She has flexion contractures at the PIP joints. Radiographs show soft tissue atrophy at the fingertips and early acro-osteolysis.
View Answer & Explanation
Correct Answer: C
Rationale: Sclerodactyly refers to the localized thickening and tightening of the skin of the fingers and hands, a hallmark feature of systemic sclerosis. This leads to the characteristic "bound-down" appearance, tapering of the digits, and difficulty with fine motor skills. Boutonnière and swan neck deformities are specific joint deformities, often seen in rheumatoid arthritis. Dupuytren's contracture involves palmar fascia thickening, not diffuse skin changes. Ulnar deviation is a common deformity in inflammatory arthritis but does not describe the skin changes. Main Distractor: D) Dupuytren's contracture causes flexion contractures of the fingers due to fascial thickening, but it does not involve the diffuse skin thickening and tapering seen in sclerodactyly.
Question 95
A 38-year-old male with systemic sclerosis presents with recurrent episodes of digital pallor, cyanosis, and rubor, particularly when exposed to cold temperatures or stress. These episodes are often painful and can last for several minutes to hours. Physical examination reveals no active ulcers, but his fingertips appear slightly atrophic. Radiographs are unremarkable for acute bony changes.
View Answer & Explanation
Correct Answer: C
Rationale: The described triphasic color changes (pallor, cyanosis, rubor) in response to cold or stress are classic for Raynaud's phenomenon, which is present in nearly all patients with systemic sclerosis. It is caused by vasospasm of the digital arteries. While vasculitis can cause digital ischemia, Raynaud's is a distinct vasospastic phenomenon. Carpal tunnel syndrome and digital nerve entrapment cause numbness and tingling, not color changes. CRPS involves pain, swelling, and autonomic dysfunction, but the specific triphasic color changes are less characteristic than for Raynaud's. Main Distractor: B) Vasculitis can cause digital ischemia and pain, but Raynaud's phenomenon is a specific vasospastic disorder characterized by the triphasic color changes, which is a hallmark of systemic sclerosis.
Question 96
A 62-year-old female with limited cutaneous systemic sclerosis (CREST syndrome) presents with painful, firm nodules on her fingertips and over her olecranon. Some of these nodules have ulcerated, draining a chalky white material. Physical examination reveals multiple subcutaneous, firm, non-mobile nodules, some with overlying skin breakdown. Radiographs show dense, amorphous calcifications within the soft tissues of the affected areas.
View Answer & Explanation
Correct Answer: C
Rationale: Calcinosis cutis, the deposition of calcium salts in the skin and subcutaneous tissues, is a common manifestation of systemic sclerosis, particularly the limited cutaneous form (CREST syndrome). The description of firm nodules, chalky white drainage, and radiographic calcifications is pathognomonic. Gouty tophi are urate crystal deposits, rheumatoid nodules are inflammatory granulomas, xanthomas are lipid deposits, and lipomas are benign fatty tumors; none typically present with the described radiographic calcifications or chalky drainage in this context. Main Distractor: A) Gouty tophi can present as subcutaneous nodules and may ulcerate, but they are composed of urate crystals and would not show dense, amorphous calcifications on radiographs in the same manner as calcinosis cutis.
Question 97
A 50-year-old male with diffuse systemic sclerosis reports progressive stiffness and limited movement in his elbows and knees, in addition to his hands. On examination, he has significant flexion contractures of the PIP joints, elbows, and knees, with taut, thickened skin overlying these joints. Passive range of motion is severely restricted. Radiographs show no acute bony pathology, but joint spaces appear narrowed in some areas.
View Answer & Explanation
Correct Answer: C
Rationale: The progressive skin thickening and fibrosis in systemic sclerosis lead to severe fibrotic contractures, particularly in the fingers, elbows, and knees. These contractures are primarily due to the tightening of the skin and subcutaneous tissues, rather than intrinsic joint inflammation (inflammatory arthritis) or cartilage degeneration (osteoarthritis). Septic arthritis would present acutely with signs of infection. Charcot arthropathy is neuropathic joint destruction. Main Distractor: A) While inflammatory arthritis can cause joint stiffness and contractures, the primary driver in systemic sclerosis is the extensive skin and soft tissue fibrosis, leading to fibrotic contractures, rather than synovitis as the main cause.
Question 98
A 42-year-old female with long-standing systemic sclerosis presents with chronic pain and tenderness at the tips of her fingers. She reports occasional digital ulcers. Physical examination reveals shortened, club-like fingertips with some nail changes. Radiographs of the hands demonstrate resorption of the distal phalangeal tufts, particularly of the index and middle fingers.
View Answer & Explanation
Correct Answer: C
Rationale: Acro-osteolysis, the resorption of the distal phalangeal tufts, is a characteristic radiographic finding in systemic sclerosis, often associated with severe Raynaud's phenomenon and digital ischemia. It contributes to the shortened, club-like appearance of the fingertips. Osteoarthritis and rheumatoid arthritis have different radiographic patterns. Psoriatic arthritis can cause "pencil-in-cup" deformities but not typically isolated distal phalangeal tuft resorption. Osteomyelitis would show signs of infection and bone destruction, not typically resorption of the tufts in this pattern. Main Distractor: A) Osteoarthritis typically affects the DIP and PIP joints with joint space narrowing and osteophytes, not specific resorption of the distal phalangeal tufts.
Question 99
A 58-year-old female with systemic sclerosis complains of numbness, tingling, and pain in her thumb, index, middle, and radial half of her ring finger, worse at night. She also reports weakness in her hand. On examination, she has thenar atrophy and a positive Tinel's sign at the wrist. Radiographs of the wrist are unremarkable.
View Answer & Explanation
Correct Answer: C
Rationale: The symptoms of numbness, tingling, and pain in the median nerve distribution (thumb, index, middle, radial ring finger), worse at night, with thenar atrophy and a positive Tinel's sign, are classic for carpal tunnel syndrome. This condition is more common in patients with systemic sclerosis due to tenosynovitis and thickening of the flexor tendons and synovial sheaths within the carpal tunnel. Ulnar nerve entrapment affects the small finger and ulnar ring finger. Radial nerve palsy affects wrist/finger extension. Cervical radiculopathy would have neck pain and broader dermatomal/myotomal involvement. Thoracic outlet syndrome has vascular and neurological symptoms but a different distribution. Main Distractor: D) Cervical radiculopathy can cause similar sensory symptoms in the hand, but the specific distribution, nocturnal worsening, thenar atrophy, and positive Tinel's sign strongly point to a peripheral nerve entrapment at the wrist, rather than a cervical spine issue.
Question 100
A 45-year-old female with diffuse systemic sclerosis presents with pain and swelling along the flexor aspects of her wrists and fingers. On examination, palpation over the flexor tendons elicits a characteristic "friction rub" or "creaking" sensation with passive motion. Radiographs show no acute bony abnormalities.
View Answer & Explanation
Correct Answer: C
Rationale: Tenosynovitis, particularly with palpable friction rubs (also known as "tendon friction rubs" or "scleroderma crepitus"), is a common and characteristic feature of systemic sclerosis, especially in the diffuse form. It is caused by inflammation and fibrosis of the tendon sheaths. Septic tenosynovitis would present with more acute signs of infection. De Quervain's affects the first dorsal compartment. Trigger finger involves nodule formation and catching. A ganglion cyst is a localized fluid-filled sac. Main Distractor: A) Septic tenosynovitis also causes pain and swelling, but the "friction rub" is a specific finding in scleroderma tenosynovitis due to fibrotic changes, and septic tenosynovitis would typically have more pronounced signs of infection (fever, erythema, severe pain with passive extension).
You Might Also Like

