ABOS Part I & AAOS OITE Orthopedic Trauma & Hand Surgery Review MCQs | Part 22228
Key Takeaway
This comprehensive module offers 42 advanced multiple-choice questions for ABOS Part I and AAOS OITE exams. It covers critical orthopedic trauma topics including proximal humerus, radial head, and distal humerus fractures, along with flexor tendon injuries like Jersey finger. Explanations detail Neer, Mason-Johnston, Leddy & Packer classifications, surgical management, and common complications, providing essential board preparation.
ABOS Part I Comprehensive Review - Batch 9
This module contains 42 advanced orthopedic multiple-choice questions developed to mirror the American Board of Orthopaedic Surgery (ABOS) Part I and AAOS OITE examinations. Questions are derived directly from high-yield clinical teaching cases.
Generated MCQ Transcript
Question 1:
A 45-year-old active male presents to the emergency department after a fall directly onto his shoulder. He complains of severe pain and inability to move his left arm. Physical examination reveals significant swelling and tenderness over the left shoulder, with ecchymosis developing. Neurovascular status is intact distally. Radiographs are obtained, as shown below.
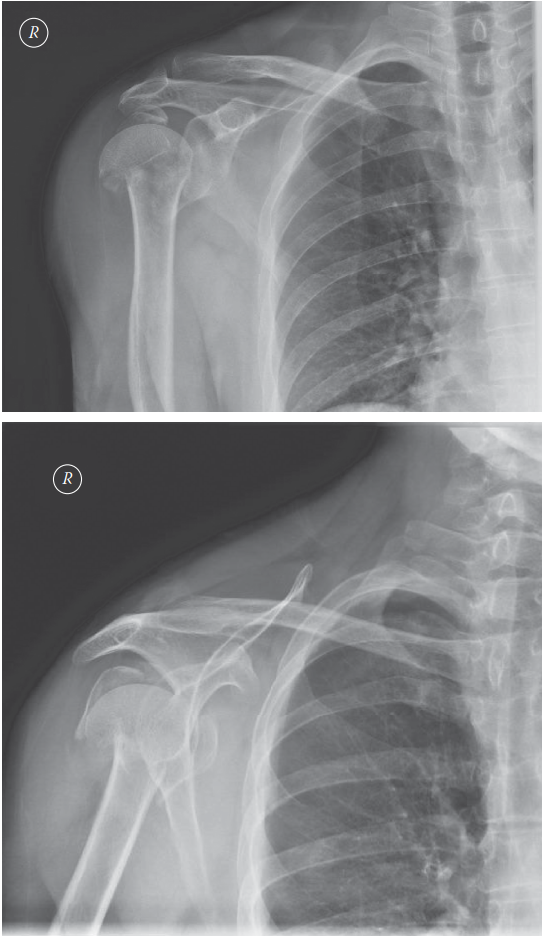
Based on the provided radiographs and the patient's presentation, what is the most appropriate Neer classification for this fracture?
- A: A. Two-part surgical neck fracture
- B: B. Three-part fracture involving the greater tuberosity
- C: C. Four-part fracture with articular involvement
- D: D. Two-part anatomical neck fracture
- E: E. Three-part fracture involving the lesser tuberosity
Explanation:
Correct Answer: B
The provided radiographs (AP and axillary lateral views) demonstrate a displaced proximal humerus fracture. Careful examination reveals that the humeral head is separated from the shaft, and the greater tuberosity is also displaced. The lesser tuberosity appears to remain attached to the humeral head fragment. This pattern, involving displacement of the humeral head, shaft, and greater tuberosity, constitutes a three-part fracture according to the Neer classification system. The Neer classification divides the proximal humerus into four segments: the articular segment (humeral head), the greater tuberosity, the lesser tuberosity, and the humeral shaft. A 'part' is defined as a major segment that is displaced by more than 1 cm or angulated by more than 45 degrees.
- Option A (Two-part surgical neck fracture): While there is a surgical neck fracture, the presence of a displaced greater tuberosity fragment makes it more than a two-part fracture.
- Option C (Four-part fracture with articular involvement): A four-part fracture would involve displacement of all four segments (head, greater tuberosity, lesser tuberosity, and shaft). In this image, the lesser tuberosity appears to be with the head fragment.
- Option D (Two-part anatomical neck fracture): An anatomical neck fracture involves the fracture line through the articular cartilage, which is not clearly depicted as the primary fracture pattern here, and it would still be more than two parts due to the displaced tuberosity.
- Option E (Three-part fracture involving the lesser tuberosity): While it is a three-part fracture, the displaced tuberosity is the greater tuberosity, not the lesser tuberosity, which appears to be with the head fragment.
Question 2:
A 45-year-old active male presents with a displaced three-part proximal humerus fracture, as seen in the provided radiographs. He has high functional demands and wishes to return to his prior level of activity, including recreational sports. Based on the case discussion, which of the following is the most appropriate initial management strategy for this patient?
- A: A. Immediate sling immobilization with early passive range of motion exercises.
- B: B. Open reduction and internal fixation (ORIF) with a proximal humerus locking plate.
- C: C. Hemiarthroplasty of the shoulder.
- D: D. Reverse total shoulder arthroplasty.
- E: E. Closed reduction and percutaneous pinning.
Explanation:
Correct Answer: B
The case explicitly states that for a more active or physiologically younger patient, surgery (specifically, fixation with a proximal humerus locking plate) is recommended to achieve the best functional outcome and avoid painful mal- or non-union. The patient's age (45 years) and high functional demands align with the criteria for surgical intervention.
- Option A (Immediate sling immobilization with early passive range of motion exercises): While non-operative treatment is an option for patients with very low functional demands, it is generally not recommended for displaced three-part fractures in active, younger patients due to the higher risk of malunion, nonunion, and poorer functional outcomes compared to surgical fixation.
- Option C (Hemiarthroplasty of the shoulder): Hemiarthroplasty is typically reserved for complex four-part fractures, head-splitting fractures, or fractures with significant osteonecrosis risk, especially in older patients, where ORIF is unlikely to achieve a good outcome. It is generally not the first choice for a three-part fracture in a 45-year-old.
- Option D (Reverse total shoulder arthroplasty): Reverse total shoulder arthroplasty is usually indicated for older patients with irreparable rotator cuff tears, severe comminution, or failed previous surgeries, not typically for an acute three-part fracture in a 45-year-old.
- Option E (Closed reduction and percutaneous pinning): While percutaneous pinning can be used for certain two-part or minimally displaced fractures, it is generally insufficient for a displaced three-part fracture, especially in an active patient where stable fixation for early rehabilitation is desired.
Question 3:
Following successful open reduction and internal fixation (ORIF) of a displaced proximal humerus fracture with a locking plate in an active 45-year-old male, the patient is counseled on potential complications. Which of the following complications, specifically mentioned in the case, is a significant concern following this procedure?
- A: A. Deep vein thrombosis (DVT)
- B: B. Heterotopic ossification
- C: C. Osteonecrosis of the humeral head
- D: D. Compartment syndrome
- E: E. Radial nerve palsy
Explanation:
Correct Answer: C
The case explicitly lists several risks specific to proximal humerus fracture surgery, including "osteonecrosis." Osteonecrosis of the humeral head is a well-known and significant complication following displaced proximal humerus fractures, particularly those involving the anatomical neck or with severe disruption of the blood supply to the humeral head. Locking plate fixation, while providing stable fixation, does not eliminate this risk, and in some cases, extensive dissection can further compromise vascularity.
- Option A (Deep vein thrombosis (DVT)): DVT is a general surgical risk, but not specifically highlighted as a unique risk for this particular injury and operation in the case description.
- Option B (Heterotopic ossification): Heterotopic ossification can occur around the shoulder, especially after trauma or surgery, but it is not specifically mentioned as a primary risk in the case's patient counseling section.
- Option D (Compartment syndrome): Compartment syndrome is extremely rare in the shoulder and upper arm following proximal humerus fractures or their fixation.
- Option E (Radial nerve palsy): The radial nerve is at risk during humeral shaft fractures or distal humerus surgery, but it is not the primary neurovascular structure at risk during a deltopectoral approach for proximal humerus plating. The axillary nerve is more commonly at risk in this region. The case mentions "neurovascular injury" generally, but osteonecrosis is a distinct and specific risk highlighted.
Question 4:
During the deltopectoral approach for open reduction and internal fixation of a proximal humerus fracture, as planned for the patient in the case, which of the following anatomical structures is most susceptible to iatrogenic injury?
- A: A. Radial nerve
- B: B. Ulnar nerve
- C: C. Axillary nerve
- D: D. Median nerve
- E: E. Long thoracic nerve
Explanation:
Correct Answer: C
The axillary nerve is the most vulnerable neurovascular structure during a deltopectoral approach for proximal humerus plating. It courses around the surgical neck of the humerus, approximately 5-7 cm distal to the acromion, and innervates the deltoid and teres minor muscles. Retraction of the deltoid or placement of screws too distally can put this nerve at significant risk of injury, leading to deltoid weakness and sensory deficits over the lateral shoulder.
- Option A (Radial nerve): The radial nerve is primarily at risk with humeral shaft fractures or approaches to the posterior humerus, not typically the deltopectoral approach for the proximal humerus.
- Option B (Ulnar nerve): The ulnar nerve is located medially in the arm and elbow, far from the surgical field of a deltopectoral approach.
- Option D (Median nerve): The median nerve is also located medially in the arm, distant from the proximal humerus surgical site.
- Option E (Long thoracic nerve): The long thoracic nerve innervates the serratus anterior and is located on the chest wall, not typically at risk during a deltopectoral approach to the proximal humerus.
Question 5:
The case mentions the PROFHER trial, which compared surgical and non-surgical treatment for displaced proximal humerus fractures. What was the primary conclusion of this multi-center randomized trial after 2 years?
- A: A. Surgical treatment consistently resulted in superior functional outcomes.
- B: B. Non-surgical treatment led to significantly higher rates of malunion and nonunion.
- C: C. There was no significant difference in outcomes between surgically and non-surgically treated patients.
- D: D. Surgical treatment was associated with a higher incidence of osteonecrosis.
- E: E. Non-surgical treatment was only effective for two-part fractures.
Explanation:
Correct Answer: C
The case explicitly states: "a multi-centre randomised trial (the PROFHER trial) did not find any difference in the outcomes of surgically and non-surgically treated patients after 2 years." This is a critical piece of information from the case and a key takeaway from the PROFHER trial. The trial's findings challenged the prevailing assumption that surgery was always superior for displaced proximal humerus fractures, particularly in older populations.
- Option A (Surgical treatment consistently resulted in superior functional outcomes): This contradicts the trial's findings as stated in the case.
- Option B (Non-surgical treatment led to significantly higher rates of malunion and nonunion): While non-surgical treatment can lead to malunion/nonunion, the PROFHER trial's primary outcome measure (Oxford Shoulder Score) did not show a significant difference in overall patient-reported outcomes, despite potential radiographic differences.
- Option D (Surgical treatment was associated with a higher incidence of osteonecrosis): While osteonecrosis is a risk of both the fracture itself and surgical intervention, the PROFHER trial's primary conclusion was about overall outcomes, not specifically a higher incidence of osteonecrosis with surgery.
- Option E (Non-surgical treatment was only effective for two-part fractures): The PROFHER trial included a range of displaced proximal humerus fractures, and its conclusion was broad, not limited to two-part fractures.
Question 6:
Considering the patient's age (45-year-old) and high functional demands, the orthopedic surgeon decides on open reduction and internal fixation (ORIF) with a locking plate. Which of the following is a primary rationale for recommending surgical intervention over non-operative management in this specific patient, as discussed in the case?
- A: A. To minimize the risk of infection.
- B: B. To ensure a faster return to work.
- C: C. To achieve the best functional outcome and avoid potentially painful mal- or non-union.
- D: D. To reduce the overall cost of treatment.
- E: E. To prevent the development of adhesive capsulitis.
Explanation:
Correct Answer: C
The case explicitly states the rationale for surgery: "I would tell the patient that surgery is generally safe and is likely to give him the best functional outcome and to avoid potentially painful mal- or non-union." This directly addresses the benefits of surgery for an active, younger patient with high functional demands, aiming for a more reliable and optimal recovery.
- Option A (To minimize the risk of infection): Infection is a risk of surgery, not something surgery prevents compared to non-operative treatment.
- Option B (To ensure a faster return to work): While surgery might facilitate an earlier start to rehabilitation, a faster return to work is not the primary stated rationale for choosing surgery over non-operative treatment in the case. The focus is on the quality of the functional outcome.
- Option D (To reduce the overall cost of treatment): Surgical treatment is generally more expensive than non-operative treatment.
- Option E (To prevent the development of adhesive capsulitis): Shoulder stiffness (adhesive capsulitis) is listed as a potential risk of surgery, not something surgery prevents. Both operative and non-operative management can lead to stiffness.
Question 7:
A 78-year-old sedentary female with low functional demands presents with a similar displaced three-part proximal humerus fracture. She has significant comorbidities, including severe osteoporosis and poorly controlled diabetes. Based on the principles discussed in the case, what would be the most appropriate initial management consideration for this patient?
- A: A. Open reduction and internal fixation with a locking plate.
- B: B. Hemiarthroplasty of the shoulder.
- C: C. Non-operative treatment with sling immobilization and early gentle pendulum exercises.
- D: D. Reverse total shoulder arthroplasty.
- E: E. Immediate referral for complex reconstructive surgery.
Explanation:
Correct Answer: C
The case contrasts the management of an active, younger patient with that of a patient with lower demands: "It is possible that for a patient with very low functional demands, non-operative treatment may allow healing with a functional result..." For an elderly, sedentary patient with low functional demands and significant comorbidities (osteoporosis, diabetes), the risks of surgery (infection, fixation failure in osteoporotic bone, general anesthesia risks) often outweigh the potential benefits. Non-operative management, focusing on pain control and early gentle motion to prevent stiffness, is often the preferred approach, aiming for a functional rather than perfect anatomical outcome.
- Option A (Open reduction and internal fixation with a locking plate): While an option for some, the severe osteoporosis and comorbidities in an elderly, low-demand patient make fixation challenging and prone to failure, and the surgical risks are higher.
- Option B (Hemiarthroplasty of the shoulder): Hemiarthroplasty is a significant surgical procedure, usually reserved for more complex fractures (e.g., four-part, head-splitting) or failed ORIF, and still carries substantial risks for a patient with multiple comorbidities.
- Option D (Reverse total shoulder arthroplasty): Reverse total shoulder arthroplasty is typically considered for very complex fractures in older patients, especially with rotator cuff deficiency, or as a salvage procedure. While it might be considered in some elderly patients with complex fractures, for a three-part fracture in a low-demand patient with comorbidities, non-operative treatment is often the safer initial choice.
- Option E (Immediate referral for complex reconstructive surgery): This is too aggressive for an initial management consideration in a patient who might benefit from non-operative care.
Question 8:
A 45-year-old active male undergoes ORIF of his displaced three-part proximal humerus fracture with a locking plate. During the post-operative period, he develops persistent pain, crepitus, and progressive loss of shoulder motion despite adherence to physical therapy. Radiographs show evidence of hardware loosening and partial collapse of the humeral head. Which of the following complications, mentioned in the case, is most likely occurring?
- A: A. Neurovascular injury
- B: B. Infection
- C: C. Shoulder stiffness
- D: D. Failure of fixation
- E: E. Adhesive capsulitis
Explanation:
Correct Answer: D
The case lists "failure of fixation" as a specific risk of the operation. The symptoms described – persistent pain, crepitus, progressive loss of motion, and radiographic evidence of hardware loosening and humeral head collapse – are classic signs of fixation failure. This can occur due to poor bone quality, inadequate reduction, improper plate placement, or early aggressive rehabilitation.
- Option A (Neurovascular injury): While a risk, neurovascular injury would typically present with immediate post-operative neurological deficits (e.g., axillary nerve palsy) or vascular compromise, not progressive pain and hardware issues.
- Option B (Infection): Infection is a risk, but it would typically present with signs like fever, redness, warmth, purulent drainage, and elevated inflammatory markers, which are not described as the primary issue here.
- Option C (Shoulder stiffness): Shoulder stiffness is a risk, but the description of hardware loosening and humeral head collapse points to a structural failure rather than just soft tissue contracture. While stiffness can result from fixation failure, it's a symptom, not the underlying primary complication described.
- Option E (Adhesive capsulitis): Adhesive capsulitis is a form of shoulder stiffness, but the radiographic findings of hardware loosening and collapse indicate a mechanical failure of the construct, which is distinct from primary adhesive capsulitis.
Question 9:
The case highlights the importance of patient counseling regarding the risks of surgery for proximal humerus fractures. When discussing the risk of shoulder stiffness with a patient undergoing ORIF, which of the following statements is most accurate?
- A: A. Shoulder stiffness is a rare complication that can be entirely prevented with early aggressive physical therapy.
- B: B. Stiffness is a common complication, and while early motion is important, some degree of stiffness can occur despite optimal management.
- C: C. Stiffness is primarily caused by neurovascular injury during surgery and is usually temporary.
- D: D. The locking plate prevents stiffness by providing rigid fixation, allowing immediate full range of motion.
- E: E. Stiffness is only a concern in non-operative management and not after surgical fixation.
Explanation:
Correct Answer: B
The case lists "shoulder stiffness" as a risk inherent with the operation. Shoulder stiffness (including adhesive capsulitis) is a common complication following both operative and non-operative treatment of proximal humerus fractures. While early, controlled rehabilitation is crucial to prevent severe stiffness, some degree of stiffness can still occur due to the initial trauma, prolonged immobilization, or inflammatory response, even with optimal surgical fixation and rehabilitation. It's important to set realistic expectations for patients.
- Option A (Shoulder stiffness is a rare complication that can be entirely prevented with early aggressive physical therapy): Stiffness is not rare, and while therapy helps, it cannot entirely prevent it in all cases. Aggressive therapy too early can also compromise fixation.
- Option C (Stiffness is primarily caused by neurovascular injury during surgery and is usually temporary): Stiffness is not primarily caused by neurovascular injury; it's more related to soft tissue healing, inflammation, and immobilization.
- Option D (The locking plate prevents stiffness by providing rigid fixation, allowing immediate full range of motion): While locking plates provide stable fixation, they do not prevent stiffness, and immediate full range of motion is typically not allowed due to the risk of fixation failure and compromise of fracture healing.
- Option E (Stiffness is only a concern in non-operative management and not after surgical fixation): This is incorrect. Stiffness is a concern in both operative and non-operative management of shoulder fractures.
Question 10:
A 45-year-old active male presents with the displaced proximal humerus fracture shown in the radiographs. The fracture involves the surgical neck and a displaced greater tuberosity. The surgeon plans for ORIF with a locking plate. Which of the following specific fracture characteristics, visible in the provided image, is a key consideration influencing the decision for surgical fixation in an active patient?
- A: A. The presence of a comminuted humeral head.
- B: B. The degree of valgus impaction of the humeral head.
- C: C. The significant displacement of the greater tuberosity.
- D: D. The presence of an isolated lesser tuberosity fracture.
- E: E. The absence of any articular surface involvement.
Explanation:
Correct Answer: C
The radiographs clearly show significant displacement of the greater tuberosity fragment. In an active patient, a displaced greater tuberosity fracture is a strong indication for surgical fixation. The greater tuberosity is the insertion site for the supraspinatus, infraspinatus, and teres minor (rotator cuff muscles). Significant displacement can lead to rotator cuff dysfunction, impingement, and poor functional outcomes if not anatomically reduced and fixed. The case emphasizes achieving the "best functional outcome" for an active patient, which necessitates addressing such displacement.
- Option A (The presence of a comminuted humeral head): While comminution can influence treatment, the primary visible displacement driving the surgical decision for a three-part fracture in this context is the tuberosity. The head itself is not described as severely comminuted in the case.
- Option B (The degree of valgus impaction of the humeral head): Valgus impaction can be a stable pattern, sometimes managed non-operatively, especially if the head is well-aligned. The image shows displacement, not necessarily stable valgus impaction.
- Option D (The presence of an isolated lesser tuberosity fracture): The image shows a displaced greater tuberosity, not an isolated lesser tuberosity fracture. Isolated lesser tuberosity fractures are less common and often associated with posterior dislocations.
- Option E (The absence of any articular surface involvement): While the articular surface may not be severely comminuted, the displacement of the head relative to the shaft and the tuberosity implies significant disruption that, if left unaddressed, could lead to articular incongruity and pain. However, the most striking and functionally significant displacement for an active patient is the greater tuberosity.
Question 11:
A 45-year-old male sustains a fall onto an outstretched hand, resulting in a radial head fracture. Radiographs show a displaced, comminuted fracture involving 40% of the articular surface with a 3mm step-off, but no mechanical block to forearm rotation. Which Mason-Johnston classification best describes this injury?
- A: Type I
- B: Type II
- C: Type III
- D: Type IV
- E: Modified Type II
Explanation:
Correct Answer: C
Mason-Johnston Type III fractures are characterized by significant comminution and/or displacement, often involving more than 30% of the articular surface and/or displacement of more than 2mm, or with mechanical block. While a Type II involves a single displaced fragment, a Type III implies more extensive disruption, typically precluding successful closed reduction and often requiring surgical intervention. Type I is a non-displaced crack. Type IV involves an associated elbow dislocation.
Question 12:
A 30-year-old male presents with persistent wrist pain and instability following a radial head fracture managed non-operatively 6 weeks ago. Initial radiographs showed a Mason-Johnston Type II radial head fracture. On examination, there is tenderness over the distal radio-ulnar joint (DRUJ) and a positive 'shuck test' at the wrist. What is the most likely underlying diagnosis causing these new symptoms?
- A: Radial head non-union
- B: Heterotopic ossification of the elbow
- C: Essex-Lopresti lesion
- D: Chronic lateral collateral ligament insufficiency
- E: Cubital tunnel syndrome
Explanation:
Correct Answer: C
The combination of a radial head fracture, interosseous membrane disruption (leading to proximal radial migration), and distal radio-ulnar joint (DRUJ) injury (manifested by wrist pain and instability/positive shuck test) constitutes an Essex-Lopresti lesion. This severe injury often leads to chronic pain and dysfunction if not recognized and treated appropriately, typically with radial head replacement and potentially DRUJ stabilization. Radial head non-union might cause local pain but wouldn't explain DRUJ instability. Heterotopic ossification and LCL insufficiency are elbow-centric and wouldn't directly cause DRUJ instability in this context. Cubital tunnel syndrome is a nerve compression issue.
Question 13:
A 62-year-old female presents with a Mason-Johnston Type II radial head fracture with 2mm displacement and a palpable block to terminal forearm pronation. There is no associated elbow dislocation or other obvious ligamentous injury. What is the most appropriate initial management strategy?
- A: Sling immobilization for 3 weeks followed by physiotherapy
- B: Open reduction and internal fixation (ORIF)
- C: Radial head excision
- D: Radial head replacement
- E: Attempt closed reduction under local anesthetic
Explanation:
Correct Answer: B
A Mason-Johnston Type II fracture with a mechanical block to forearm rotation (even with only 2mm displacement) is a strong indication for surgical intervention, typically ORIF if the fragment is amenable. The mechanical block signifies impingement of the displaced fragment, which will prevent full range of motion and lead to chronic dysfunction if not addressed. Sling immobilization alone is insufficient. Radial head excision is generally reserved for severely comminuted fractures not amenable to ORIF, or in low-demand patients, and can lead to proximal radial migration and DRUJ issues. Radial head replacement is typically indicated for highly comminuted (Type III/IV) fractures not reconstructible, or in Essex-Lopresti injuries. Attempting closed reduction is unlikely to succeed with a palpable block from a displaced articular fragment.
Question 14:
Which of the following associated injuries is most commonly missed in the initial evaluation of an isolated radial head fracture?
- A: Medial collateral ligament tear
- B: Coronoid process fracture
- C: Capitellum chondral injury
- D: Distal radio-ulnar joint (DRUJ) instability
- E: Olecranon fracture
Explanation:
Correct Answer: D
While all listed injuries can occur with radial head fractures, DRUJ instability, indicative of an Essex-Lopresti lesion or other forearm axis disruption, is often missed initially. It presents as insidious wrist pain and instability that becomes apparent days or weeks after the initial injury to the radial head. Coronoid and MCL injuries are typically associated with terrible triad injuries involving elbow dislocation. Capitellum chondral injuries are less common and often only seen on arthroscopy or MRI. Olecranon fractures are usually obvious on initial X-rays.
Question 15:
A 55-year-old painter presents with a Mason-Johnston Type III radial head fracture with 4 fragments, involving 60% of the articular surface. He is very active and desires a full return to function. There is no associated elbow dislocation. What is the preferred surgical option to restore function and stability?
- A: Open reduction and internal fixation (ORIF) with headless screws
- B: Radial head excision
- C: Radial head replacement
- D: Primary arthrodesis of the elbow
- E: Non-operative management with early motion
Explanation:
Correct Answer: C
For highly comminuted (Mason-Johnston Type III or IV) radial head fractures, particularly in active patients where restoration of articular congruity and preservation of radial length are critical, radial head replacement is often the preferred surgical option. ORIF may be difficult or impossible with 4 fragments involving 60% of the articular surface. Radial head excision can lead to proximal radial migration and DRUJ issues, especially in younger, active patients. Arthrodesis is a salvage procedure for end-stage arthritis or instability, not a primary option for acute fractures. Non-operative management is not appropriate for a significantly comminuted, displaced Type III fracture in an active individual.
Question 16:
What is the primary concern when considering radial head excision for a comminuted radial head fracture in a young, active patient?
- A: Risk of heterotopic ossification
- B: Development of chronic elbow stiffness
- C: Increased risk of infection
- D: Proximal migration of the radius and DRUJ instability
- E: Failure to relieve mechanical block
Explanation:
Correct Answer: D
The primary concern with radial head excision, especially in younger, active patients, is the loss of longitudinal stability of the forearm, leading to proximal migration of the radius and subsequent distal radio-ulnar joint (DRUJ) instability. This can cause significant wrist pain and dysfunction. While elbow stiffness and heterotopic ossification are potential complications of any elbow trauma or surgery, proximal migration and DRUJ issues are specific and major drawbacks of radial head excision.
Question 17:
Which of the following is an absolute contraindication for radial head excision in the management of a radial head fracture?
- A: Concomitant ipsilateral distal radius fracture
- B: Older, low-demand patient
- C: Associated interosseous membrane disruption (Essex-Lopresti lesion)
- D: Previous elbow surgery
- E: Type II radial head fracture
Explanation:
Correct Answer: C
Associated interosseous membrane disruption, characteristic of an Essex-Lopresti lesion, is an absolute contraindication for radial head excision. In these cases, the radial head plays a critical role in longitudinal forearm stability. Removing it would exacerbate proximal radial migration, leading to severe DRUJ disruption and chronic wrist pain. In such scenarios, radial head replacement is indicated to restore length and stability. Concomitant distal radius fracture is a relative contraindication but not absolute. Older, low-demand patients might be candidates for excision in certain scenarios. Previous elbow surgery is a relative consideration, and a Type II fracture may be amenable to ORIF or, in some cases, excision if small and non-reconstructible, but it is not an absolute contraindication.
Question 18:
A 28-year-old male sustains a Mason-Johnston Type IV radial head fracture with a posterior elbow dislocation. After successful closed reduction of the elbow, radiographs show significant comminution of the radial head. What is the most appropriate next step in management?
- A: Immediate radial head excision
- B: Open reduction and internal fixation (ORIF) of the radial head
- C: Radial head replacement with concurrent assessment of elbow stability
- D: Sling immobilization and early range of motion
- E: Long arm casting for 6 weeks
Explanation:
Correct Answer: C
A Mason-Johnston Type IV fracture with elbow dislocation (often part of a 'terrible triad' if coronoid and LCL are also injured) requires careful management. After reduction of the dislocation, the radial head injury needs to be addressed to restore stability and function. Given significant comminution in an active 28-year-old, radial head replacement is often the best option to restore radial length and provide buttress to the lateral elbow, preventing recurrent instability. Concurrently, the elbow's stability, especially regarding the LCL and potentially MCL, must be assessed. ORIF would be challenging with significant comminution. Excision is contraindicated due to the high risk of instability. Non-operative management or casting would not address the inherent instability caused by the radial head comminution in this severe injury.
Question 19:
Which surgical approach provides the best exposure for ORIF of a radial head fracture while minimizing the risk to the posterior interosseous nerve (PIN)?
- A: Posterolateral approach (Kocher approach)
- B: Anterior approach (Henry approach)
- C: Medial approach
- D: Direct posterior approach
- E: Lateral approach with anconeus muscle split
Explanation:
Correct Answer: A
The posterolateral approach, also known as the Kocher approach, is widely preferred for radial head fractures. It uses the interval between the anconeus and extensor carpi ulnaris (ECU) muscles. This approach protects the posterior interosseous nerve (PIN), which typically lies within the supinator muscle, distal and anterior to the radial head. The anterior (Henry) approach risks the PIN more directly, and medial or direct posterior approaches are generally not suitable for radial head fixation. The lateral approach with anconeus muscle split is similar to Kocher but the key is the safe interval.
Question 20:
Regarding the posterior interosseous nerve (PIN) during surgical approaches to the radial head, at what point is it most vulnerable?
- A: As it passes anterior to the humerus
- B: As it exits the radial tunnel
- C: As it pierces the superficial head of the supinator muscle
- D: Distal to the radial tuberosity
- E: Proximally, near the axilla
Explanation:
Correct Answer: C
The posterior interosseous nerve (PIN) is a branch of the radial nerve. It becomes vulnerable as it enters and passes through the supinator muscle (often referred to as the Arcade of Frohse, the proximal edge of the superficial head of the supinator). During surgical approaches to the radial head, particularly if the dissection extends too far anterior or distal, the PIN can be at risk, especially where it pierces the superficial head of the supinator muscle within the radial tunnel. This is why the Kocher approach, staying posterior, is preferred.
Question 21:
A 45-year-old male sustains a comminuted distal humerus fracture involving both columns and the articular surface (AO 13-C3) after a fall from a height. Clinically, he has significant swelling, pain, and a palpable ulnar nerve neuropraxia. Radiographs confirm the diagnosis, and a CT scan reveals severe comminution. Which of the following surgical approaches is generally considered the workhorse for achieving adequate exposure for anatomical reduction and stable fixation of such a fracture?
- A: Anterior approach (Henry)
- B: Medial approach
- C: Lateral approach (Kocher)
- D: Posterior approach with olecranon osteotomy
- E: Triceps-sparing posterior approach
Explanation:
Correct Answer: D
For complex, comminuted intra-articular distal humerus fractures (AO 13-C3), a posterior approach with an olecranon osteotomy (e.g., Chevron osteotomy) provides the most extensive and direct visualization of the entire distal humeral articular surface and both columns. This allows for precise anatomical reduction of articular fragments and robust plate application. While triceps-sparing approaches are gaining popularity, they often provide less complete visualization for severely comminuted intra-articular fractures. Anterior, medial, and lateral approaches are typically reserved for specific fracture patterns (e.g., isolated capitellar or trochlear fractures) or for less complex supracondylar fractures.
Question 22:
Regarding the surgical fixation of a complex intra-articular distal humerus fracture, what is the most biomechanically stable construct for dual plating?
- A: Two parallel plates on the posterior surface
- B: A single long plate spanning the medial and lateral columns
- C: Orthogonal plating (medial and posterior/posterolateral plates)
- D: Two plates applied to the anterior surface
- E: Parallel plating (two plates on the medial and lateral columns)
Explanation:
Correct Answer: C
Orthogonal plating, typically with a medial plate and a posterior or posterolateral plate, creates a more stable construct biomechanically than parallel plating. This configuration provides support against both valgus/varus and torsional forces, acting as a '90-90' system (relative to each other, not the bone's long axis). Parallel plating (medial and lateral column plates) is also a strong construct, particularly for stabilizing the columns, but biomechanical studies often show orthogonal plating to be superior in complex fractures due to better load distribution and resistance to displacement. Posterior plates alone or anterior plates are insufficient for complex intra-articular fractures.
Question 23:
During the surgical exposure for a distal humerus fracture, which anatomical structure is at highest risk of iatrogenic injury, particularly during posteromedial dissection?
- A: Radial nerve
- B: Musculocutaneous nerve
- C: Median nerve
- D: Ulnar nerve
- E: Brachial artery
Explanation:
Correct Answer: D
The ulnar nerve is the most vulnerable neurological structure during posterior approaches to the distal humerus. It courses through the cubital tunnel posterior to the medial epicondyle and is often directly exposed, mobilized, and protected (often transposed anteriorly) during complex distal humerus fracture fixation to prevent iatrogenic injury or secondary compression. The radial nerve is at risk more proximally in the humeral shaft, the median nerve and brachial artery are anterior and generally protected by muscle bellies, and the musculocutaneous nerve is even further anterior and lateral.
Question 24:
Following open reduction and internal fixation (ORIF) of a severely comminuted intra-articular distal humerus fracture in a 68-year-old osteoporotic patient, what is the most common early complication directly related to the fixation construct in this patient population?
- A: Nonunion
- B: Heterotopic ossification
- C: Infection
- D: Hardware pull-out or failure
- E: Ulnar nerve palsy
Explanation:
Correct Answer: D
In osteoporotic patients, the primary concern for early complication after ORIF of a comminuted distal humerus fracture is hardware pull-out or failure. Poor bone quality provides inadequate purchase for screws, leading to loss of reduction and implant failure. This necessitates specific techniques like locking plates, longer screws, and sometimes bone augmentation. Nonunion and heterotopic ossification are typically later complications. Infection is a risk but not specifically heightened by osteoporosis itself. Ulnar nerve palsy is a risk from the surgery but not directly related to implant mechanics in osteoporotic bone.
Question 25:
A 32-year-old presents with a displaced intra-articular distal humerus fracture (AO 13-C1). Initial assessment reveals a healthy patient with no neurovascular deficits. What is the most appropriate next step in management after initial stabilization and plain radiographs?
- A: Immediate surgical exploration and ORIF
- B: Application of a long-arm cast and follow-up in 2 weeks
- C: Order a CT scan with 3D reconstructions of the elbow
- D: Begin immediate active range of motion exercises
- E: Administer broad-spectrum antibiotics and admit for observation
Explanation:
Correct Answer: C
While surgical fixation is likely indicated, a CT scan with 3D reconstructions is crucial for operative planning of intra-articular distal humerus fractures. Plain radiographs often underestimate the degree of articular comminution and displacement. The CT scan provides detailed information about fragment size, location, and the extent of articular involvement, which guides the choice of surgical approach and fixation strategy. Immediate ORIF without CT is suboptimal. A cast is inappropriate for displaced intra-articular fractures, and immediate ROM is contraindicated pre-operatively. Antibiotics are not indicated unless an open fracture is suspected.
Question 26:
What is the primary role of the olecranon osteotomy in the surgical management of complex distal humerus fractures?
- A: To provide a tension band effect for the triceps muscle
- B: To facilitate ulnar nerve decompression
- C: To allow direct, panoramic visualization of the articular surface and distal humerus
- D: To prevent heterotopic ossification in the olecranon fossa
- E: To shorten the healing time of the overall fracture
Explanation:
Correct Answer: C
The primary advantage of an olecranon osteotomy is to provide a wide, direct, and panoramic surgical exposure of the entire distal humeral articular surface and both columns. This enables accurate anatomical reduction of often numerous small articular fragments under direct vision, which is paramount for restoring elbow function and minimizing post-traumatic arthritis. While an ulnar nerve decompression can be performed concomitantly, it's not the primary role of the osteotomy. The osteotomy itself is a separate fracture that requires fixation and has its own potential complications, and it doesn't directly prevent HO or shorten overall healing time.
Question 27:
A 75-year-old female with severe osteoporosis sustains a highly comminuted distal humerus fracture (AO 13-C3) with significant bone loss. She has a low functional demand but is medically fit for surgery. What surgical option might be considered in this specific scenario, even if ORIF is technically possible but challenging to achieve stable fixation?
- A: Functional bracing and early mobilization
- B: Total elbow arthroplasty (TEA)
- C: Elbow fusion
- D: Excision arthroplasty
- E: Hemiarthroplasty of the distal humerus
Explanation:
Correct Answer: B
For elderly, osteoporotic patients with highly comminuted distal humerus fractures where stable ORIF is unlikely to be achieved, or if stable fixation will not allow early motion, Total Elbow Arthroplasty (TEA) is an increasingly accepted option, particularly in patients with low functional demands. It allows for immediate stability and early motion, which is critical in this population to prevent stiffness. Functional bracing is unlikely to yield a good result with a highly comminuted, unstable fracture. Elbow fusion would be highly disabling for a low-demand patient. Excision arthroplasty is rarely performed today due to poor outcomes. Hemiarthroplasty of the distal humerus is not a standard procedure for complex distal humerus fractures due to the articulation challenges with the native ulna and radius.
Question 28:
Following ORIF of a distal humerus fracture, a patient develops severe progressive elbow stiffness. What is the most common cause of this complication after successful fracture healing?
- A: Nonunion of the fracture
- B: Post-traumatic heterotopic ossification (HO)
- C: Ulnar nerve entrapment
- D: Chronic infection
- E: Radial head subluxation
Explanation:
Correct Answer: B
Post-traumatic heterotopic ossification (HO) is a common cause of severe elbow stiffness after distal humerus fractures and their surgical treatment, even after successful fracture healing. It can restrict motion significantly. While nonunion can cause pain and instability, it doesn't directly cause stiffness in the same way HO does. Ulnar nerve entrapment typically causes paresthesia and weakness, not direct mechanical stiffness. Chronic infection is possible but less common than HO. Radial head subluxation is not a typical complication leading to global stiffness after a distal humerus fracture.
Question 29:
Which of the following is an absolute indication for surgical intervention in a distal humerus fracture?
- A: An open fracture
- B: Neurovascular deficit (motor only)
- C: Intra-articular displacement > 2mm
- D: Age greater than 65 years
- E: Associated olecranon fracture
Explanation:
Correct Answer: A
An open fracture is an absolute indication for surgical débridement and fixation due to the high risk of infection. Neurovascular deficits, especially an acute deficit following injury, often warrant emergent exploration but can sometimes be observed if a neuropraxia is suspected without overt vascular compromise. Intra-articular displacement > 2mm is a strong indication for ORIF but is generally considered a relative indication (compared to open fracture). Age > 65 years is a patient factor, not a fracture characteristic dictating surgery. An associated olecranon fracture is a complex injury but not an absolute indication in itself compared to an open fracture.
Question 30:
A 55-year-old male undergoes ORIF of a distal humerus fracture. Post-operatively, he develops severe pain, swelling, and bullae around the elbow. What is the most appropriate initial management step to prevent catastrophic complications?
- A: Elevate the limb and administer oral analgesics
- B: Immediate release of constrictive dressings and fasciotomy if compartment syndrome is suspected
- C: Start intravenous antibiotics immediately
- D: Perform a diagnostic ultrasound to rule out DVT
- E: Apply a hot pack to reduce swelling
Explanation:
Correct Answer: B
Severe pain, swelling, and bullae post-operatively are highly concerning for evolving compartment syndrome, particularly in the forearm. Immediate release of all constrictive dressings (splints, casts, bandages) is paramount. If suspicion remains high or objective signs (e.g., pain out of proportion, pain with passive stretch) are present, emergent fasciotomy is indicated to prevent irreversible ischemic damage. While elevation is good, and antibiotics might be considered later if infection is suspected, the immediate life-altering threat is compartment syndrome. Ultrasound for DVT is not relevant to acute swelling and pain in this context, and hot packs would worsen swelling.
Question 31:
A 30-year-old professional football player sustains an injury to his ring finger during a game. He reports his finger was forcibly extended while gripping an opponent's jersey. On examination, he has swelling and tenderness over the palmar aspect of the distal phalanx. He is unable to actively flex the DIP joint of the ring finger. The remaining fingers show a normal cascade. Passive DIP flexion is full. Initial X-rays are negative for any bony avulsion. Given this presentation, what is the most likely Leddy and Packer classification, and what is the primary concern dictating the urgency of surgical intervention?
- A: Type II; risk of FDS tendon rupture.
- B: Type III; prevention of articular incongruity.
- C: Type I; preservation of FDP tendon vascularity.
- D: Type IV; management of the avulsed bone fragment.
- E: Type I; prevention of intrinsic muscle contracture.
Explanation:
Correct Answer: C
Rationale:
This clinical scenario describes a classic Leddy and Packer Type I Jersey finger. A Type I injury involves a complete avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx, without an associated bony avulsion. Due to the lack of a bony fragment, the tendon typically retracts proximally, often into the palm or even the forearm. This significant retraction usually results in the stripping of the vincula tendinum, which are the primary source of blood supply to the FDP tendon within the flexor sheath. Loss of this blood supply places the tendon at high risk of necrosis.
- Option C (Type I; preservation of FDP tendon vascularity) is correct. The primary concern driving the urgency for surgical repair (ideally within 7-10 days) in a Type I injury is to re-establish the tendon's blood supply and prevent necrosis, which would severely compromise healing and functional outcome.
- Option A (Type II; risk of FDS tendon rupture) is incorrect. A Type II injury also lacks a bony avulsion, but the tendon retracts only to the level of the A3 pulley or PIP joint, often retaining some vincula and thus better vascularity, making it slightly less urgent than Type I. FDS rupture is not the primary concern.
- Option B (Type III; prevention of articular incongruity) is incorrect. A Type III injury involves a bony avulsion fragment that prevents significant tendon retraction and often preserves the tendon's blood supply. Articular incongruity is a concern with intra-articular fractures (Type V) but not the defining feature or primary urgency for Type III.
- Option D (Type IV; management of the avulsed bone fragment) is incorrect. A Type IV injury involves a bony avulsion where the FDP tendon has also avulsed from the bone fragment itself. The scenario explicitly states no bony avulsion.
- Option E (Type I; prevention of intrinsic muscle contracture) is incorrect. While contractures can be a complication of prolonged immobilization or stiffness, the immediate and primary concern for a Type I injury is tendon viability, not intrinsic muscle contracture.
Question 32:
A 25-year-old rock climber presents with chronic pain and a noticeable 'bowstringing' of his long finger flexor tendons during active flexion, following a previous injury that was initially managed non-operatively. He reports a significant loss of grip strength. Which of the following anatomical structures is most likely compromised?
- A: The C1 and C2 pulleys.
- B: The A1 pulley.
- C: The A2 and A4 pulleys.
- D: The FDS decussation.
- E: The lumbrical muscle origin.
Explanation:
Correct Answer: C
Rationale:
The flexor pulley system consists of annular (A) and cruciate (C) pulleys that keep the flexor tendons closely apposed to the phalanges. This close apposition is crucial for maintaining the mechanical advantage of the flexor tendons, preventing 'bowstringing,' and ensuring efficient finger flexion.
- Option C (The A2 and A4 pulleys) is correct. The A2 pulley (over the proximal phalanx) and the A4 pulley (over the middle phalanx) are considered the most critical annular pulleys for preventing bowstringing and maintaining the mechanical efficiency of the flexor tendons. Rupture or compromise of these pulleys leads to the tendon lifting away from the bone during flexion (bowstringing), resulting in a significant loss of mechanical advantage and grip strength.
- Option A (The C1 and C2 pulleys) is incorrect. The cruciate pulleys (C1, C2, C3) are thinner and less critical for preventing bowstringing compared to the annular pulleys.
- Option B (The A1 pulley) is incorrect. The A1 pulley is located at the MCP joint and its rupture typically leads to trigger finger, not bowstringing along the length of the finger.
- Option D (The FDS decussation) is incorrect. The FDS decussation is where the FDS tendon splits to allow the FDP to pass through. While important for FDS function, its injury does not directly cause bowstringing of the entire flexor system.
- Option E (The lumbrical muscle origin) is incorrect. The lumbrical muscles originate from the FDP tendons and insert into the extensor mechanism. Their injury or dysfunction is associated with conditions like lumbrical plus phenomenon, not bowstringing.
Question 33:
Following a successful FDP repair for a Jersey finger, a patient is placed on an early active motion rehabilitation protocol. What is the primary goal of this protocol, and what common complication is it specifically designed to mitigate?
- A: To strengthen the FDP tendon; re-rupture.
- B: To reduce post-operative pain; nerve irritation.
- C: To prevent adhesion formation; stiffness and limited range of motion.
- D: To accelerate bone healing; non-union of the distal phalanx.
- E: To improve blood supply to the tendon; tendon necrosis.
Explanation:
Correct Answer: C
Rationale:
Early active motion protocols are a cornerstone of modern flexor tendon rehabilitation. They involve controlled, gentle active and passive movements of the repaired digit within a protective splint, starting soon after surgery.
- Option C (To prevent adhesion formation; stiffness and limited range of motion) is correct. The primary goal of early active motion is to promote tendon gliding within the flexor sheath and prevent the formation of restrictive adhesions between the repaired tendon and the surrounding tissues (e.g., flexor sheath, FDS tendon). Adhesions are the most common cause of post-operative stiffness and limited range of motion following flexor tendon repair. Controlled motion helps maintain a clear gliding surface.
- Option A (To strengthen the FDP tendon; re-rupture) is incorrect. While strengthening is a later goal, the immediate early active motion phase is not primarily for strengthening the tendon, but for promoting gliding. Excessive force during early motion can actually risk re-rupture, which the protocol aims to prevent by keeping forces low.
- Option B (To reduce post-operative pain; nerve irritation) is incorrect. While motion can help with swelling and indirectly pain, it's not the primary goal, and nerve irritation is not the main complication it mitigates.
- Option D (To accelerate bone healing; non-union of the distal phalanx) is incorrect. Early motion protocols are for tendon healing and gliding, not directly for accelerating bone healing. Non-union is a complication of bony avulsion repairs, but not the primary target of early motion.
- Option E (To improve blood supply to the tendon; tendon necrosis) is incorrect. While motion can improve local circulation, the primary blood supply to the tendon is critical at the time of repair (especially for Type I injuries). Early motion's main role is not to improve blood supply to prevent necrosis, but to prevent adhesions.
Question 34:
A 40-year-old patient presents with a chronic FDP rupture of the ring finger (6 months post-injury). When attempting to make a full fist, the patient exhibits paradoxical hyperextension of the DIP joint and hyperextension of the PIP joint of the affected finger. This specific clinical presentation is known as:
- A: Quadriga effect.
- B: Boutonniere deformity.
- C: Swan neck deformity.
- D: Lumbrical plus phenomenon.
- E: Mallet finger.
Explanation:
Correct Answer: D
Rationale:
The described clinical presentation is characteristic of the lumbrical plus phenomenon.
- Option D (Lumbrical plus phenomenon) is correct. This occurs when the FDP tendon is ruptured, slack, or excessively shortened (e.g., due to overtensioned repair or chronic retraction). When the patient attempts to flex the finger (activating the FDP muscle belly), the lumbrical muscle, which originates from the FDP tendon and inserts into the extensor mechanism, is pulled proximally. This tension on the lumbrical causes it to act as an extensor of the DIP joint and can also contribute to PIP joint hyperextension, resulting in paradoxical DIP extension (or hyperextension) when the patient tries to make a fist.
- Option A (Quadriga effect) is incorrect. The quadriga effect refers to the restriction of flexion in adjacent, uninjured fingers due to overtensioning or shortening of one FDP tendon, as they share a common muscle belly. It does not involve paradoxical DIP extension.
- Option B (Boutonniere deformity) is incorrect. A boutonniere deformity is characterized by PIP joint flexion and DIP joint hyperextension, typically due to a central slip rupture of the extensor mechanism.
- Option C (Swan neck deformity) is incorrect. A swan neck deformity is characterized by PIP joint hyperextension and DIP joint flexion, often seen in conditions like rheumatoid arthritis or due to FDS laxity.
- Option E (Mallet finger) is incorrect. A mallet finger is a flexion deformity of the DIP joint due to rupture or avulsion of the extensor tendon at its insertion on the distal phalanx.
Question 35:
A 55-year-old manual laborer presents 4 months after sustaining a Jersey finger injury (Type I) to his long finger. He has no active DIP flexion and significant tendon retraction into the palm. Direct primary repair is deemed impossible due to the chronic nature and extensive tendon shortening. What is the most appropriate surgical management strategy for this patient?
- A: Primary FDP advancement with a bone anchor.
- B: Non-operative management with intensive hand therapy.
- C: Immediate DIP joint arthrodesis.
- D: Staged tendon reconstruction using a silicone rod followed by tendon grafting.
- E: Flexor digitorum superficialis (FDS) tenodesis to the distal phalanx.
Explanation:
Correct Answer: D
Rationale:
For chronic FDP ruptures (typically beyond 3-4 weeks, and certainly at 4 months) where significant tendon retraction and shortening have occurred, direct primary repair or FDP advancement (which is suitable for acute injuries with small gaps, usually <1 cm) is generally not feasible without excessive tension. Excessive tension leads to complications like the quadriga effect or re-rupture.
- Option D (Staged tendon reconstruction using a silicone rod followed by tendon grafting) is correct. This is the gold standard for managing chronic FDP ruptures with significant tendon loss or retraction. In the first stage, a silicone rod (Hunter rod) is inserted into the flexor sheath to create a smooth, gliding pseudosheath. After several months, in a second stage, the silicone rod is removed, and an autogenous tendon graft (e.g., palmaris longus, plantaris) is threaded through the pseudosheath and attached to the distal phalanx and the FDP muscle belly, restoring active flexion.
- Option A (Primary FDP advancement with a bone anchor) is incorrect. FDP advancement is for acute injuries with minimal retraction. At 4 months, the tendon would be too retracted and shortened for this technique without excessive tension.
- Option B (Non-operative management with intensive hand therapy) is incorrect. Non-operative management will not restore active DIP flexion in a complete, chronic FDP rupture.
- Option C (Immediate DIP joint arthrodesis) is incorrect. While arthrodesis is a salvage procedure for failed repairs or in specific cases (e.g., severe arthritis, very low functional demand), it is generally not the first-line treatment for a chronic FDP rupture, especially in a manual laborer who might benefit from some active motion.
- Option E (Flexor digitorum superficialis (FDS) tenodesis to the distal phalanx) is incorrect. FDS tenodesis can provide some active DIP flexion or prevent hyperextension, but it typically offers less robust motion and strength compared to a staged FDP reconstruction. It might be considered for older patients with lower functional demands or as a simpler alternative, but staged reconstruction is generally preferred for restoring more complete function in a manual laborer.
Question 36:
A surgeon performs a primary FDP repair for a Type I Jersey finger. Post-operatively, the patient complains that when attempting to make a full fist with the repaired finger, the adjacent middle and small fingers are unable to fully flex at their DIP joints. What is the most likely cause of this specific complication?
- A: Adhesions within the flexor sheath of the repaired finger.
- B: Re-rupture of the FDP tendon in the repaired finger.
- C: Excessive tension on the repaired FDP tendon.
- D: Lumbrical plus phenomenon in the repaired finger.
- E: Insufficient strength of the FDS tendons in the adjacent fingers.
Explanation:
Correct Answer: C
Rationale:
The described complication is a classic presentation of the quadriga effect.
- Option C (Excessive tension on the repaired FDP tendon) is correct. The quadriga effect occurs because the FDP tendons of the middle, ring, and small fingers share a common muscle belly (or are closely intertwined proximally). If one FDP tendon (in this case, the repaired ring finger FDP) is repaired with excessive tension or advanced too much, it restricts the full excursion of the entire FDP muscle group. When the patient attempts to flex the repaired finger, the overtensioned FDP prevents the adjacent, otherwise healthy FDP tendons from fully flexing their respective DIP joints.
- Option A (Adhesions within the flexor sheath of the repaired finger) is incorrect. Adhesions would primarily limit the range of motion (both flexion and extension) of the repaired finger itself, not specifically restrict flexion in the adjacent fingers.
- Option B (Re-rupture of the FDP tendon in the repaired finger) is incorrect. Re-rupture would result in a complete loss of active DIP flexion in the repaired finger, not restricted flexion in adjacent fingers.
- Option D (Lumbrical plus phenomenon in the repaired finger) is incorrect. Lumbrical plus phenomenon involves paradoxical DIP extension of the repaired finger when attempting to flex, not restricted flexion in adjacent fingers.
- Option E (Insufficient strength of the FDS tendons in the adjacent fingers) is incorrect. The FDS tendons primarily flex the PIP joints. The complaint is about DIP joint flexion, which is controlled by the FDP.
Question 37:
A 22-year-old athlete sustains a Type I Jersey finger injury. The FDP tendon is found to be retracted into the palm. What specific anatomical structures are most critical for providing blood supply to the FDP tendon in the distal finger, and why is their disruption a major concern in this injury type?
- A: The A2 and A4 pulleys; they provide direct arterial branches.
- B: The flexor sheath; it contains a rich vascular plexus.
- C: The vincula tendinum; they are mesotendinous structures supplying the tendon.
- D: The lumbrical muscles; they directly vascularize the FDP.
- E: The digital neurovascular bundles; they run adjacent to the tendon.
Explanation:
Correct Answer: C
Rationale:
The blood supply to the flexor tendons within the fibro-osseous sheath is crucial for their viability and healing. This supply comes primarily from specific mesotendinous structures.
- Option C (The vincula tendinum; they are mesotendinous structures supplying the tendon) is correct. The vincula tendinum (vincula longa and vincula brevia) are delicate mesotendinous folds that connect the flexor tendons to the phalanges and the flexor sheath. They carry small arteries that provide the primary blood supply to the FDP and FDS tendons as they pass through the flexor sheath. In a Type I Jersey finger, the FDP tendon avulses without a bony fragment and retracts significantly into the palm. This retraction often strips the tendon of its vincula, leading to a loss of its intrinsic blood supply and placing it at high risk of necrosis, which is why urgent repair is critical.
- Option A (The A2 and A4 pulleys; they provide direct arterial branches) is incorrect. The A2 and A4 pulleys are crucial mechanical structures that prevent bowstringing and maintain mechanical advantage, but they are not the primary source of blood supply to the tendon substance itself.
- Option B (The flexor sheath; it contains a rich vascular plexus) is incorrect. While the flexor sheath provides a low-friction environment and contains some vascularity, the direct supply to the tendon comes via the vincula, not directly from the sheath itself as a primary source.
- Option D (The lumbrical muscles; they directly vascularize the FDP) is incorrect. The lumbrical muscles originate from the FDP tendons but do not provide the primary blood supply to the FDP tendon itself along its course in the finger.
- Option E (The digital neurovascular bundles; they run adjacent to the tendon) is incorrect. The digital neurovascular bundles run on the sides of the fingers and supply the skin, nerves, and bone, but they do not directly vascularize the FDP tendon within its sheath.
Question 38:
A 19-year-old patient presents with an acute Jersey finger of the ring finger. Surgical repair is planned. Which of the following surgical incisions is most commonly preferred for accessing the flexor tendons in the finger and why?
- A: A straight longitudinal volar incision; it provides direct access.
- B: A midaxial incision along the side of the finger; it avoids neurovascular structures.
- C: A transverse volar incision at the level of the PIP joint; it minimizes scarring.
- D: A zigzag incision (Brunner's incision) over the volar aspect; it prevents flexion contracture.
- E: A dorsal approach with splitting of the extensor mechanism; it offers better visualization.
Explanation:
Correct Answer: D
Rationale:
The choice of surgical incision for flexor tendon repair in the finger is critical to ensure adequate exposure while minimizing complications, particularly flexion contractures.
- Option D (A zigzag incision (Brunner's incision) over the volar aspect; it prevents flexion contracture) is correct. The Brunner's zigzag incision is the most commonly preferred and safest approach for accessing the flexor tendons and sheath in the finger. This incision provides excellent exposure of the underlying structures while avoiding the creation of a long, linear scar that would be prone to contracting across the flexion creases, thereby preventing a flexion contracture.
- Option A (A straight longitudinal volar incision; it provides direct access) is incorrect. While it provides direct access, a straight longitudinal volar incision is contraindicated in the finger due to the very high risk of developing a severe and debilitating flexion contracture as the scar matures.
- Option B (A midaxial incision along the side of the finger; it avoids neurovascular structures) is incorrect. A midaxial incision is typically used for bony procedures, joint access, or accessing the neurovascular bundles, but it does not provide optimal direct access to the flexor tendons within their sheath. It also runs close to the neurovascular bundles.
- Option C (A transverse volar incision at the level of the PIP joint; it minimizes scarring) is incorrect. While transverse incisions can minimize scarring, a single transverse incision would provide very limited exposure for a flexor tendon repair that often spans multiple zones.
- Option E (A dorsal approach with splitting of the extensor mechanism; it offers better visualization) is incorrect. A dorsal approach is used for extensor tendon injuries, dorsal bony injuries, or joint fusions. It does not provide access to the flexor tendons, which are on the volar aspect of the finger.
Question 39:
A 16-year-old patient undergoes FDP repair for a Type I Jersey finger of the small finger. The surgeon notes that the small finger FDP tendon appears smaller in diameter and somewhat more friable than typically seen in other digits. What is the most likely long-term implication of this observation, specifically for the small finger?
- A: Increased risk of quadriga effect.
- B: Higher incidence of lumbrical plus phenomenon.
- C: Greater propensity for persistent stiffness and poorer functional outcomes.
- D: Reduced risk of re-rupture due to less tension.
- E: Faster healing time due to smaller size.
Explanation:
Correct Answer: C
Rationale:
While FDP avulsion injuries can occur in any digit, the small finger is often cited as having unique challenges and potentially poorer outcomes.
- Option C (Greater propensity for persistent stiffness and poorer functional outcomes) is correct. The FDP tendon of the small finger is often anatomically smaller in diameter and can be inherently weaker or more friable compared to the FDP tendons of the other digits. This smaller caliber and potentially poorer tissue quality can make surgical repair more challenging, lead to less robust repairs, and contribute to a higher rate of persistent stiffness, less overall range of motion, and generally poorer functional outcomes (e.g., grip strength, dexterity) even with technically successful repairs and diligent rehabilitation.
- Option A (Increased risk of quadriga effect) is incorrect. The quadriga effect is related to excessive tension in the repair, not specifically to the small finger's inherent tendon quality.
- Option B (Higher incidence of lumbrical plus phenomenon) is incorrect. Lumbrical plus is related to FDP slackness or overtensioning, not specifically to the small finger's intrinsic tendon quality.
- Option D (Reduced risk of re-rupture due to less tension) is incorrect. A smaller, weaker tendon would likely have an increased risk of re-rupture if not repaired adequately, not a reduced risk.
- Option E (Faster healing time due to smaller size) is incorrect. Tendon healing is a biological process that is not significantly accelerated by smaller tendon size; rather, smaller size can make the repair more delicate.
Question 40:
A 35-year-old patient presents with a suspected Jersey finger. On physical examination, you stabilize the patient's adjacent fingers (long and small) in full extension and ask them to actively flex the PIP joint of the ring finger. The patient is able to flex the PIP joint against resistance. What information does this specific maneuver provide?
- A: It confirms a complete FDP rupture.
- B: It rules out a central slip rupture.
- C: It assesses the integrity and function of the FDS tendon.
- D: It indicates an intact lumbrical muscle.
- E: It suggests a partial FDP tear.
Explanation:
Correct Answer: C
Rationale:
This maneuver is a classic test to isolate and assess the function of the Flexor Digitorum Superficialis (FDS) tendon.
- Option C (It assesses the integrity and function of the FDS tendon) is correct. The FDS tendons for the middle, ring, and small fingers share a common muscle belly (or are closely related proximally), as do the FDP tendons. To isolate the FDS of a specific finger, the adjacent fingers must be held in full extension. This maneuver prevents the FDP of the tested finger from acting (as the FDP of the adjacent fingers would also be activated, causing unwanted flexion). If the patient can then actively flex the PIP joint of the tested finger against resistance, it confirms the integrity and function of the FDS tendon for that digit.
- Option A (It confirms a complete FDP rupture) is incorrect. This test assesses FDS function, not FDP rupture. FDP rupture is assessed by the inability to actively flex the DIP joint.
- Option B (It rules out a central slip rupture) is incorrect. A central slip rupture affects the extensor mechanism at the PIP joint, leading to a boutonniere deformity. This test is for flexor function.
- Option D (It indicates an intact lumbrical muscle) is incorrect. While the lumbricals are intrinsic muscles, this test specifically isolates FDS function.
- Option E (It suggests a partial FDP tear) is incorrect. This test does not directly assess the FDP tendon.
Question 41:
A 48-year-old patient undergoes surgical repair of a Type III Jersey finger, where a large bony avulsion fragment was reattached to the distal phalanx. Four weeks post-operatively, X-rays show no signs of healing at the bone-to-bone interface, and the patient reports persistent pain and tenderness over the distal phalanx. What is the most likely complication in this scenario?
- A: Re-rupture of the FDP tendon.
- B: Lumbrical plus phenomenon.
- C: Non-union of the bony fragment.
- D: Quadriga effect.
- E: Adhesions within the flexor sheath.
Explanation:
Correct Answer: C
Rationale:
A Type III Jersey finger involves a bony avulsion fragment from the distal phalanx. When this fragment is reattached, the healing of the bone-to-bone interface is crucial for a successful outcome.
- Option C (Non-union of the bony fragment) is correct. The scenario describes a lack of radiographic healing at the bone-to-bone interface and persistent pain/tenderness, which are classic signs of a non-union of the reattached bony fragment. This is a specific complication associated with avulsion fractures where bone healing is required.
- Option A (Re-rupture of the FDP tendon) is incorrect. Re-rupture would present as a loss of active DIP flexion, not primarily as persistent pain and lack of bone healing on X-ray, although it could be a secondary complication if the bone fixation fails.
- Option B (Lumbrical plus phenomenon) is incorrect. Lumbrical plus is related to FDP tendon length/tension and presents with paradoxical DIP extension, not bone healing issues.
- Option D (Quadriga effect) is incorrect. The quadriga effect is related to excessive tension in the FDP repair, restricting adjacent finger flexion, not bone healing.
- Option E (Adhesions within the flexor sheath) is incorrect. Adhesions would cause stiffness and limited range of motion, but not specifically a lack of bone healing on X-ray or persistent pain at the bone site.
Question 42:
A 65-year-old patient with a history of poorly controlled diabetes and peripheral neuropathy sustains an acute Type I Jersey finger. He is scheduled for surgical repair. Compared to a healthy, non-diabetic patient, what is the most significant increased risk factor for a poor outcome in this patient?
- A: Increased risk of quadriga effect.
- B: Higher likelihood of lumbrical plus phenomenon.
- C: Significantly impaired wound healing and increased infection risk.
- D: Inability to tolerate early active motion protocols.
- E: Greater chance of associated nerve injury.
Explanation:
Correct Answer: C
Rationale:
Systemic comorbidities can significantly impact the prognosis and outcome of flexor tendon repairs.
- Option C (Significantly impaired wound healing and increased infection risk) is correct. Poorly controlled diabetes, especially when accompanied by peripheral neuropathy, is a major risk factor for complications in surgical procedures, including flexor tendon repair. Diabetes impairs wound healing due to microvascular disease (reduced blood flow), neuropathy (impaired sensation and trophic changes), and compromised immune function. This leads to a substantially increased risk of surgical site infection, delayed tendon healing, and overall poorer functional outcomes.
- Option A (Increased risk of quadriga effect) is incorrect. The quadriga effect is primarily related to surgical technique (excessive tension in the repair), not directly to diabetes.
- Option B (Higher likelihood of lumbrical plus phenomenon) is incorrect. Lumbrical plus phenomenon is related to FDP tendon length/tension, not directly to diabetes.
- Option D (Inability to tolerate early active motion protocols) is incorrect. While neuropathy might affect sensation and compliance, the primary issue is biological healing, not necessarily tolerance of motion protocols, which are carefully controlled.
- Option E (Greater chance of associated nerve injury) is incorrect. While peripheral neuropathy is present, it doesn't inherently increase the chance of an associated nerve injury from the initial trauma or during surgery more than in a healthy individual. The concern is more about the healing process.
⚠️ Unanswered Questions
You have unanswered questions in this module. Are you sure you want to submit?
You Might Also Like
