Congenital Dislocation of the Patella: Comprehensive Surgical Management

Key Takeaway
Congenital dislocation of the patella is a rare, often bilateral pediatric deformity characterized by a fixed, irreducible lateral displacement of the patella. Early diagnosis via ultrasound or MRI is critical, as the unossified patella obscures radiographic evaluation in infancy. Surgical intervention, primarily involving extensive lateral release and medial plication, is mandated early to prevent progressive genu valgum, external tibial rotation, and severe flexion contractures.
INTRODUCTION TO CONGENITAL PATELLAR DISLOCATION
Congenital dislocation of the patella is a rare, profound pediatric orthopedic anomaly characterized by a fixed, irreducible lateral displacement of the patella present at birth. Unlike developmental or traumatic patellar instability, true congenital dislocation is deeply rooted in severe dysplastic changes of the entire extensor mechanism. The condition is frequently familial and bilateral, suggesting a strong genetic or developmental etiology.
While it can present as an isolated anomaly, it is highly associated with generalized syndromic conditions, most notably arthrogryposis multiplex congenita, Down syndrome, nail-patella syndrome, and Rubinstein-Taybi syndrome. Left untreated, the dislocated extensor mechanism acts as a deforming force across the growing knee joint, leading to progressive, severe secondary bony and soft-tissue deformities that severely compromise ambulatory function.
PATHOANATOMY AND BIOMECHANICS
The pathoanatomy of congenital patellar dislocation is complex and involves both soft-tissue contractures and secondary osseous dysplasia. The primary underlying pathological condition is a severe contracture of the quadriceps mechanism.
Soft Tissue Abnormalities
The vastus lateralis is typically severely contracted, fibrotic, or occasionally entirely absent in its normal muscular form, replaced by a dense fibrous band. The patella is displaced laterally and is often tethered directly to the anterior aspect of the iliotibial (IT) band. Because of this lateral tethering, the medial capsular structures and the medial patellofemoral ligament (MPFL) become chronically stretched, attenuated, and functionally incompetent. Furthermore, the insertion of the patellar tendon on the tibial tubercle is frequently lateralized, exacerbating the abnormal lateral vector force.
Osseous Deformities
The patella itself is often dysplastic, appearing small, misshapen, and situated in an abnormal, proximal, and lateral location within the quadriceps mechanism. The chronic lateral position of the extensor mechanism alters the normal compressive forces across the distal femur and proximal tibia. Consequently, the lateral femoral condyle fails to develop normally and becomes severely flattened, lacking the normal anterior prominence required to buttress the patella.
Biomechanical Consequences
Biomechanically, the lateralized extensor mechanism shifts posterior to the mechanical axis of the knee joint.
1. Flexion Contracture: Because the extensor mechanism lies posterior to the center of rotation of the knee, it paradoxically acts as a knee flexor rather than an extensor, leading to an obligate flexion contracture.
2. Genu Valgum: The lateral tethering creates a valgus moment across the growing physis, leading to progressive genu valgum.
3. External Tibial Rotation: The lateralized pull of the patellar tendon on the tibial tubercle acts as a persistent external rotator of the tibia on the femur.
Clinical Pearl: The severity of the secondary bony deformities (genu valgum, external tibial rotation, and condylar flattening) is directly proportional to the length of time the dislocation remains uncorrected. Early surgical intervention is therefore prophylactic against irreversible osseous dysplasia.
CLASSIFICATION: EILERT'S SYNDROMES
Eilert delineated two distinct clinical syndromes regarding pediatric patellar dislocation, which dictate both the clinical presentation and the timing of surgical intervention. Understanding the distinction between these two entities is paramount for the orthopedic surgeon.
1. Persistent (Congenital) Dislocation
This is the true congenital dislocation.
* Pathology: The patella is dislocated laterally and is fixed (persistent) in that location regardless of knee position.
* Onset: Obvious in infancy.
* Associations: Frequently associated with generalized syndromes (e.g., arthrogryposis).
* Clinical Findings: A knee flexion contracture is almost universally present. It produces severe functional disability, delaying or preventing normal ambulation.
* Treatment Timing: Mandates early surgical correction (as soon as the diagnosis is made and the child is medically optimized) to prevent progressive bony deformity.
2. Obligatory (Habitual) Dislocation
Eilert suggested the term "obligatory dislocation" is more accurate than the historical term "habitual dislocation."
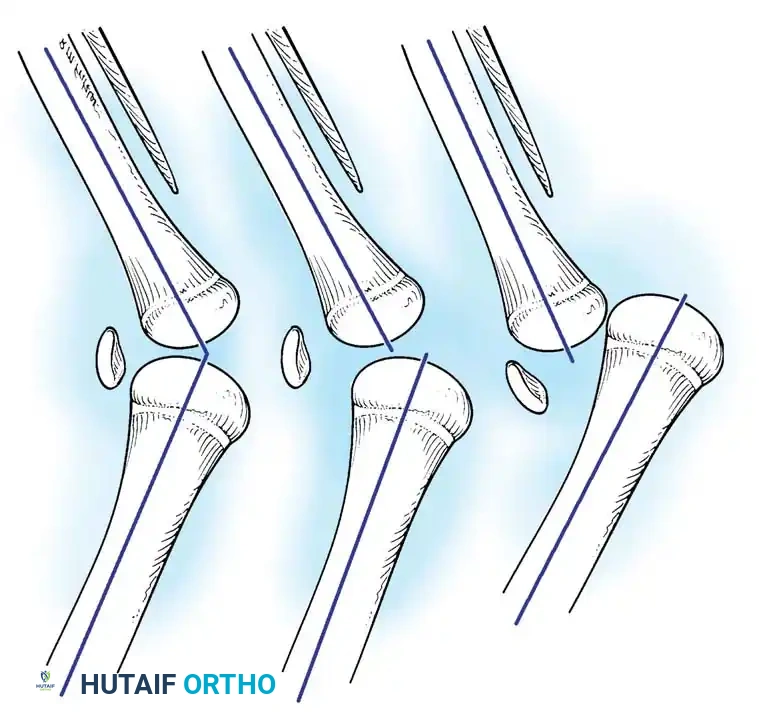
* Pathology: The patella dislocates laterally with knee flexion and reduces spontaneously with knee extension. The dislocation is an obligatory part of the knee's arc of motion.
* Onset: Usually presents later, typically between 5 and 10 years of age.
* Associations: Usually an isolated anomaly without syndromic association.
* Clinical Findings: The range of knee motion is usually normal. It may be well tolerated with surprisingly little functional disability in the early stages.
* Treatment Timing: Surgical correction can be delayed until the patient becomes symptomatic or begins to show signs of progressive functional decline.
CLINICAL EVALUATION AND IMAGING
Physical Examination
In neonates and infants, the diagnosis requires a high index of suspicion. The knee often presents with a flexion contracture and a valgus alignment. Palpation of the anterior knee reveals an empty trochlear groove, with the small, cartilaginous patella palpable on the lateral aspect of the lateral femoral condyle. Active extension is severely limited or absent.
Radiographic Evaluation
The diagnosis of congenital dislocation of the patella is notoriously difficult to make on standard radiographs before the patient is 3 to 4 years old. This is due to the lack of ossification of the patella, which remains entirely cartilaginous in infancy.
As seen in older children (Fig. 26-65), the anteroposterior (AP) view will demonstrate the fixed lateral dislocation. Crucially, on the lateral radiograph, the patella often appears "absent" because it is superimposed over the lateral femoral condyle, rather than sitting anteriorly in the trochlea.
Advanced Imaging
- Ultrasound: Several authors advocate for the use of high-resolution ultrasonography in neonates and infants. Ultrasound can clearly define the position of the cartilaginous patella relative to the trochlea dynamically, confirming the diagnosis without ionizing radiation.
- Magnetic Resonance Imaging (MRI): MRI is the gold standard for preoperative planning. It clearly delineates the cartilaginous patella lying lateral to the femur, quantifies the degree of vastus lateralis and IT band contracture, and assesses the morphology of the trochlea and lateral femoral condyle.
Surgical Warning: Do not delay surgery in a symptomatic infant with a fixed flexion contracture simply because the patella is not visible on plain radiographs. Utilize ultrasound or MRI to confirm the diagnosis and proceed with early soft-tissue release.
SURGICAL MANAGEMENT
The primary objective of surgery is the complete release of the contracted structures on the lateral side of the patella to allow tension-free reduction into the trochlear groove, combined with medial plication to stabilize the construct. Operative techniques must be tailored to the patient's age, skeletal maturity, and the severity of the pathoanatomy.
Indications and Timing
For true persistent congenital dislocation, surgery should be performed as soon as the diagnosis is confirmed and the infant is cleared for anesthesia (often between 6 and 12 months of age). Delaying surgery guarantees the progression of valgus, flexion, and external rotation deformities. For obligatory dislocation, surgery is indicated when the child develops pain, instability, or gait deterioration.
Step-by-Step Surgical Technique
1. Positioning and Approach
- The patient is positioned supine on the operating table. A sterile tourniquet is applied to the proximal thigh.
- A longitudinal midline or slightly anterolateral incision is utilized, extending from the distal third of the femur to just distal to the tibial tubercle.
- Full-thickness fasciocutaneous flaps are elevated medially and laterally to expose the entire extensor mechanism.
2. Extensive Lateral Release
- Identification: The laterally displaced patella and its tethering structures are identified. The vastus lateralis and IT band will be seen blending into the lateral border of the patella.
- Release: An extensive lateral release is mandatory. This is not a simple retinacular release; it requires a deep, structural release of the lateral capsule, the iliotibial band, and the lateral portion of the quadriceps tendon.
- The IT band must be sharply detached from the patella and the lateral retinaculum. In severe cases, a fractional lengthening or Z-plasty of the vastus lateralis tendon may be required.
- The release must extend proximally enough to mobilize the entire quadriceps mechanism and distally to the lateral border of the patellar tendon.
- Assessment: Following the lateral release, the patella should be easily reducible into the trochlear groove without undue tension. If tension persists, further proximal release of the lateral structures is required.
3. Medial Plication and VMO Advancement
- The stretched, redundant medial capsule is incised longitudinally.
- In Younger Children: Extensive lateral release combined with simple medial capsular plication (vest-over-pants suturing) is often sufficient to obtain and maintain patellofemoral congruency.
- In Older Children: Advancement of the vastus medialis obliquus (VMO) is usually necessary. The VMO is mobilized, advanced distally and laterally, and sutured to the superomedial border of the patella to tighten the muscle, improve its dynamic medializing vector, and restore active terminal extension.
4. Distal Realignment Procedures
Depending on the degree of lateralization of the tibial tubercle and the skeletal maturity of the patient, distal realignment may be required to correct the Q-angle.
- Skeletally Immature Patients: Tibial tubercle osteotomy is strictly contraindicated due to the risk of proximal tibial physeal arrest (resulting in recurvatum deformity).
- Roux-Goldthwait Procedure: The lateral half of the patellar tendon is detached from the tibial tubercle, routed beneath the intact medial half, and sutured to the medial soft tissues (sartorius insertion or medial periosteum). Gao et al. reported satisfactory results in 88 patients utilizing extensive lateral release, medial plication, and this lateral-half patellar tendon transfer.
- Entire Patellar Tendon Transfer: Gordon and Schoenecker described transferring the entire patellar tendon medially using soft-tissue anchors or periosteal suturing in skeletally immature patients. Langenskiöld and Ritsilä also reported successful treatment of 18 congenitally dislocated knees utilizing lateral release and medial soft-tissue transfer of the patellar tendon.
- Skeletally Mature Patients: A formal medializing tibial tubercle osteotomy (e.g., Elmslie-Trillat or Fulkerson osteotomy) is performed. The tubercle is transferred medially to normalize the tibial tubercle-trochlear groove (TT-TG) distance and fixed with cortical screws.
Pitfall: Failure to adequately release the lateral structures (especially the IT band tether) is the most common cause of recurrent dislocation. The medial plication should act as a check-rein, not as the primary force pulling a tight patella into the groove. If the medial sutures are under high tension, the lateral release is inadequate.
Management of the Dysplastic Trochlea
In long-standing cases, the trochlear groove may be severely dysplastic or flat. However, in young children, once the patella is reduced and stabilized, the compressive forces of the patella during growth will often stimulate remodeling of the cartilaginous trochlea. Routine trochleoplasty is generally avoided in young children due to the risk of damaging the distal femoral physis and articular cartilage, though it may be considered in older, skeletally mature patients with severe, symptomatic trochlear dysplasia.
POSTOPERATIVE PROTOCOL
Meticulous postoperative care is essential to maintain the reduction while allowing the soft tissues to heal.
- Immobilization: Immediately postoperatively, the knee is immobilized in a long-leg cast or a rigid cylinder cast in full extension. This protects the medial plication and VMO advancement from early tension.
- Duration: The cast is maintained for approximately 6 weeks. During this time, weight-bearing status is determined by the stability of the repair and whether a bony distal realignment was performed (typically toe-touch or non-weight-bearing for osteotomies; weight-bearing as tolerated for soft-tissue only procedures).
- Rehabilitation: Upon cast removal at 6 weeks, aggressive physical therapy is initiated.
- Active and passive range-of-motion (ROM) exercises are begun to combat arthrofibrosis, which is a significant risk following extensive knee releases.
- Quadriceps strengthening, particularly targeting the VMO, is emphasized to maintain dynamic medial stability.
- Night splinting in extension may be utilized for an additional 4 to 6 weeks if a flexion contracture threatens to recur.
OUTCOMES AND COMPLICATIONS
When performed early and comprehensively, surgical correction yields excellent functional results. At an average 5-year follow-up, Gordon and Schoenecker reported that all patients experienced pain relief and a marked increase in activity tolerance following lateral release, VMO advancement, and appropriate distal realignment.
Potential Complications:
* Recurrence: Usually due to inadequate lateral release or failure to address a lateralized tibial tubercle.
* Arthrofibrosis and Stiffness: Extensive soft-tissue dissection can lead to scarring. Early, supervised ROM after the initial 6-week immobilization period is critical.
* Over-constriction: Excessive medial plication can lead to iatrogenic medial patellar subluxation or increased patellofemoral contact pressures, leading to early chondromalacia.
* Physeal Arrest: A catastrophic complication if a bony tibial tubercle transfer is erroneously performed in a skeletally immature patient. Always utilize soft-tissue transfers (Roux-Goldthwait or similar) until the proximal tibial physis is closed.
You Might Also Like