Comprehensive Introduction and Patho-Epidemiology
The management of unstable dorsal proximal interphalangeal (PIP) joint fracture-dislocations represents one of the most formidable challenges in hand surgery. These injuries, often dismissed initially by patients as simple "jammed fingers," possess a high potential for chronic morbidity, including debilitating stiffness, persistent instability, and early-onset post-traumatic arthrosis. When the structural integrity of the palmar lip of the middle phalanx is compromised beyond a critical threshold, the joint loses its primary restraint against dorsal translation. In these scenarios, simple closed reduction and splinting are universally doomed to failure, necessitating complex surgical intervention to restore the precise anatomical geometry of the articulation.
The hemi-hamate autograft reconstruction has emerged as the gold standard for addressing complex, unstable PIP dorsal fracture-dislocations, particularly those involving substantial articular comminution or those presenting in a delayed or chronic setting. Originally popularized by Hastings and colleagues, this procedure leverages the unique, serendipitous anatomical mirroring between the distal articular surface of the hamate and the palmar base of the middle phalanx. By harvesting a vascularized or non-vascularized osteochondral graft from the hamate and meticulously securing it to the middle phalanx, the surgeon can instantaneously re-establish the critical palmar cup, restore the volar plate attachment, and provide a stable biomechanical foundation for immediate post-operative mobilization.
Epidemiologically, these injuries predominantly afflict young, active individuals, frequently occurring during athletic endeavors involving high-velocity ball impacts (such as basketball, volleyball, or baseball) or during occupational trauma. The socio-economic impact of a stiff, painful PIP joint in a dominant hand cannot be overstated, as it severely compromises grip strength, fine motor dexterity, and overall hand kinematics. Consequently, the orthopedic surgeon must approach these injuries with a profound respect for the delicate balance of the PIP joint and a mastery of the micro-surgical and osteosynthesis techniques required to execute a hemi-hamate arthroplasty successfully.
The overarching goal of this definitive chapter is to provide an exhaustive, step-by-step masterclass on the hemi-hamate autograft reconstruction. We will dissect the nuanced patho-anatomy of PIP instability, rigorously define the indications for operative intervention, detail the meticulous surgical technique required for both graft harvest and recipient site preparation, and outline an aggressive yet safe rehabilitation protocol. Mastery of this procedure is an essential component of the armamentarium for any surgeon dedicated to the advanced reconstruction of the upper extremity.
Detailed Surgical Anatomy and Biomechanics
A profound, granular understanding of the PIP joint's functional anatomy is the absolute prerequisite for diagnosing and treating its pathology. The PIP joint is not merely a simple hinge; it is a highly constrained, complex bicondylar articulation engineered to provide an extensive arc of motion—typically exceeding 95 degrees of flexion—while maintaining absolute concentric reduction under massive compressive and shear loads.
Static Stabilizers and Articular Geometry
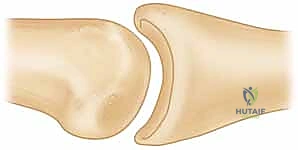
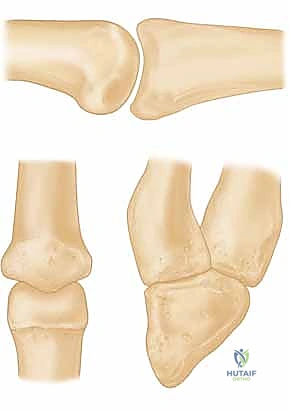
The static stability of the PIP joint is orchestrated by a synergistic complex comprising the articular geometry, the collateral ligament system, and the robust palmar (volar) plate. The proximal phalanx head is distinctly bicondylar, featuring a central intercondylar groove. Conversely, the base of the middle phalanx is biconcave, divided by a subtle median cartilaginous ridge. This specific geometry creates a "cup-shaped" configuration at the palmar lip of the middle phalanx, which acts as a profound bony buttress against dorsal translation of the middle phalanx relative to the proximal phalanx.
The palmar plate is a dense, fibrocartilaginous structure that forms the floor of the PIP joint. Proximally, it originates from the proximal phalanx via two flexible check-rein ligaments, allowing it to glide during flexion. Distally, it inserts firmly into the palmar base of the middle phalanx, just volar to the articular surface. This distal insertion is paramount; it not only prevents joint hyperextension but also serves as the critical anchor point for the accessory collateral ligaments.
The collateral ligament complex itself is bipartite. The proper collateral ligaments originate from the dorsal-lateral aspect of the proximal phalanx head and insert onto the palmar-lateral base of the middle phalanx. They are eccentrically mounted, remaining lax in extension and becoming maximally taut in full flexion. The accessory collateral ligaments fan out more volarly to insert directly into the lateral margins of the palmar plate, stabilizing the plate and suspending it like a hammock beneath the joint.
Dynamic Stabilizers and Kinematics
The dynamic stabilizers of the PIP joint—namely the extrinsic flexor and extensor tendon mechanisms—play a paradoxical role in the setting of trauma. Under normal physiological conditions, these tendons provide balanced compressive forces that maintain joint congruity. However, when the static restraints (the palmar lip and the palmar plate) are disrupted, these same dynamic forces become the primary drivers of pathological dorsal subluxation.
The central slip of the extensor digitorum communis inserts directly onto the dorsal base of the middle phalanx. When the palmar lip is fractured and the volar tether is lost, the unopposed pull of the central slip actively levers the middle phalanx dorsally. Simultaneously, the flexor digitorum superficialis (FDS), which bifurcates and inserts along the volar-lateral margins of the middle phalanx shaft, exerts a proximal and dorsal vector force when the joint is in a compromised state.
Therefore, the pathogenesis of dorsal fracture-dislocations is a biomechanical cascade: the loss of the palmar bony buttress and volar plate insertion removes the resistance to dorsal translation, while the intact central slip and FDS tendons actively pull the middle phalanx up and over the condyles of the proximal phalanx. Understanding this vector mismatch is critical, as it dictates that any successful surgical reconstruction must not only restore the bony anatomy but also neutralize these deforming forces to permit early active motion.
Classification and Pathogenesis of PIP Instability
To appropriately select patients for hemi-hamate reconstruction, the surgeon must differentiate between stable and unstable fracture patterns. This distinction is entirely dependent on the pathomechanics of the injury and the precise percentage of the articular surface that has been compromised.
Avulsion versus Impaction Shear Mechanisms
Middle phalangeal palmar lip fractures generally arise from two distinct biomechanical mechanisms, each producing a characteristic fracture pattern. The first is an avulsion mechanism, typically resulting from abrupt, forced hyperextension of the PIP joint. The immense tensile load is transmitted through the palmar plate, avulsing a bony fragment from the palmar base of the middle phalanx.
Avulsion fractures are generally non-comminuted, transverse, and involve a relatively small percentage of the articular surface (usually less than 30%). Because the dorsal articular concavity remains intact and sufficient palmar buttress is preserved, these injuries are overwhelmingly stable. They can typically be managed non-operatively with dorsal block splinting or, if displaced, with simple lag screw osteosynthesis. They rarely, if ever, require osteochondral grafting.
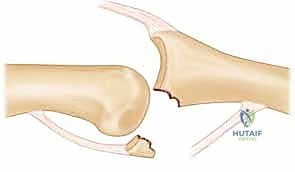
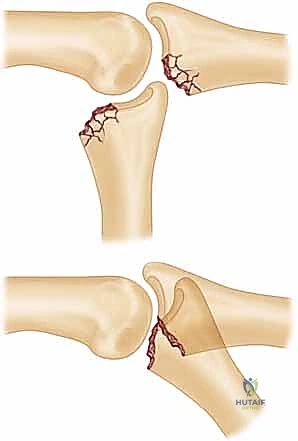
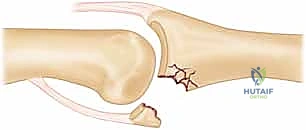
Conversely, the impaction shear mechanism is the primary culprit behind unstable fracture-dislocations requiring complex reconstruction. This occurs when a massive longitudinal axial load is applied to the digit while the PIP joint is in slight flexion. The force drives the palmar lip of the middle phalanx violently into the condyles of the proximal phalanx.

This shear-impaction force obliterates the palmar lip, resulting in profound comminution. The articular fragments are frequently driven deep into the soft cancellous metaphysis of the middle phalanx. This mechanism destroys the critical palmar cup and often involves 40% to 80% of the articular surface, rendering the joint catastrophically unstable and entirely unamenable to simple primary repair or pinning.
Clinical Evaluation and Radiographic Assessment
The clinical presentation of an unstable PIP fracture-dislocation is pathognomonic. The digit is globally swollen, exquisitely tender, and often rests in a visibly deformed, semi-flexed posture. The middle phalanx may appear dorsally translated relative to the proximal phalanx. A thorough neurovascular examination is mandatory, though true neurovascular compromise is exceedingly rare unless there is an associated open injury or massive soft tissue degloving.
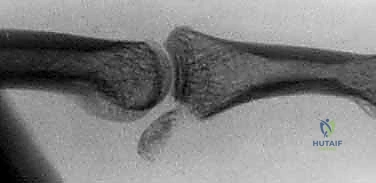
High-quality, true lateral and posteroanterior (PA) radiographs are the cornerstone of diagnostic imaging. The lateral view must be scrutinized meticulously. The surgeon must assess the percentage of the articular surface involved in the fracture. The biomechanical threshold for instability is widely accepted as 40% to 50% articular involvement; at this point, the joint will inevitably subluxate dorsally. However, clinical instability can be observed with as little as 30% involvement depending on the specific geometry of the fracture line.
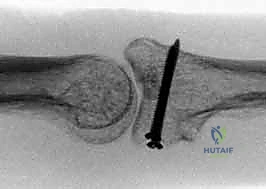
The most critical radiographic finding is the "V-sign" on the lateral projection. In a concentrically reduced PIP joint, the joint space between the proximal and middle phalanges should appear as parallel lines. If the middle phalanx is dorsally subluxated, the joint space diverges dorsally, creating a V-shaped radiolucency.
The presence of a V-sign, no matter how subtle, indicates persistent dorsal instability. If left uncorrected, the articular cartilage will rapidly undergo shear degradation, leading to intractable pain and rapid-onset osteoarthritis. The hemi-hamate reconstruction is specifically designed to eradicate this V-sign by restoring the palmar buttress.
Exhaustive Indications and Contraindications
The decision to proceed with a hemi-hamate autograft reconstruction must be made judiciously. It is a technically demanding, salvage-type procedure reserved for specific, severe injury patterns where simpler methods of internal fixation or dynamic traction are destined to fail.
| Category | Specific Criteria | Rationale |
|---|---|---|
| Primary Indications | Acute dorsal fracture-dislocations with >50% articular loss. | The palmar buttress is completely lost; primary screw fixation is impossible due to comminution. |
| Chronic dorsal fracture-dislocations (>4-6 weeks old). | Fracture fragments have resorbed or malunited; the joint cannot be concentrically reduced without reconstructing the palmar lip. | |
| Failed previous surgical interventions. | Cases where dynamic external fixation (e.g., Suzuki frame) or primary pinning failed to maintain concentric reduction. | |
| Severe impaction-shear injuries with metaphyseal bone loss. | The hamate graft provides both structural articular cartilage and cancellous bone to fill the metaphyseal void. | |
| Absolute Contraindications | Active local or systemic infection. | High risk of deep joint infection and catastrophic graft failure. |
| Volar (Palmar) PIP fracture-dislocations. | The pathoanatomy is reversed; the dorsal lip is fractured, and the hamate graft is not designed for dorsal reconstruction. | |
| Severe degenerative osteoarthritis of the PIP joint. | The proximal phalanx head is already destroyed; hemi-arthroplasty will fail. Total joint arthroplasty or arthrodesis is required. | |
| Relative Contraindications | Patient non-compliance or inability to participate in intense rehabilitation. | Post-operative stiffness is the primary enemy; without rigorous therapy, the procedure will result in a stiff, non-functional finger. |
| Concomitant severe soft tissue crush injuries. | Poor soft tissue envelope increases the risk of wound breakdown and graft avascular necrosis. | |
| Pre-existing hamate pathology (e.g., CMC arthritis). | Harvesting the graft may exacerbate existing wrist pain or instability. |
The ideal candidate is a highly motivated patient with an isolated, severe dorsal fracture-dislocation who understands the rigorous postoperative demands. The surgeon must explicitly counsel the patient that while the procedure will restore stability and alleviate pain, a return to a completely "normal" joint with 100 degrees of motion is highly unlikely, and some degree of permanent stiffness is to be expected.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of a successful hemi-hamate reconstruction. The surgeon must not only understand the defect at the PIP joint but also possess a flawless mental map of the donor site anatomy at the carpometacarpal (CMC) joint.
Imaging Modalities and Pre-Surgical Templating
While plain radiographs are usually sufficient for diagnosis, a fine-cut Computed Tomography (CT) scan of the affected digit is highly recommended for complex or chronic cases. A CT scan provides a three-dimensional understanding of the articular comminution, the depth of the metaphyseal impaction, and the exact size of the bony defect that needs to be grafted. This allows the surgeon to mentally template the size of the required hamate graft prior to making an incision.
Furthermore, standard posteroanterior, lateral, and oblique radiographs of the ipsilateral wrist should be obtained to ensure there is no pre-existing degenerative joint disease at the 4th and 5th CMC joints, which would preclude harvesting the hamate graft. The distal articular surface of the hamate features a central ridge that divides the facets for the 4th and 5th metacarpals; this ridge perfectly mimics the median ridge of the middle phalanx base, making it an ideal anatomical substitute.
Anesthesia, Positioning, and Tourniquet Application
The procedure is typically performed under regional anesthesia (axillary or supraclavicular brachial plexus block) combined with intravenous sedation, though general anesthesia may be utilized based on patient preference or specific medical comorbidities. The patient is positioned supine with the operative extremity extended on a radiolucent hand table.
A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination of the limb using an Esmarch bandage is performed, and the tourniquet is inflated to standard upper extremity pressures (typically 250 mmHg or 100 mmHg above systolic blood pressure). A sterile field is prepped and draped to include the entire hand, wrist, and distal forearm. Intraoperative fluoroscopy (mini C-arm) must be positioned to allow for effortless, unobstructed imaging in both the PA and true lateral planes throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the hemi-hamate autograft reconstruction is divided into three distinct phases: preparation of the recipient site (the PIP joint), harvesting of the donor graft (the hamate), and the definitive osteosynthesis and soft tissue reconstruction.
Volar Approach to the PIP Joint
The PIP joint is approached via a palmar zigzag (Brunner) incision centered over the joint, extending from the mid-proximal phalanx to the mid-middle phalanx. Meticulous elevation of the skin flaps is performed, taking great care to identify and protect the neurovascular bundles bilaterally. The flexor tendon sheath is exposed.
The C1 and A3 pulleys are incised to allow retraction of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. The tendons are retracted laterally using a Penrose drain or specialized tendon retractors, exposing the underlying volar plate. The volar plate is typically found to be avulsed from its distal insertion on the middle phalanx.
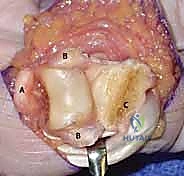
The accessory collateral ligaments are sharply released from the margins of the volar plate, and the joint is "shotgunned" (hyperextended) to provide a panoramic view of the articular surfaces of both the proximal and middle phalanges.
Preparation of the Middle Phalanx Defect
Once the joint is fully exposed, the extent of the articular destruction becomes readily apparent. All comminuted, devitalized cartilaginous and bony fragments are meticulously debrided using a combination of fine rongeurs, curettes, and a high-speed burr.

The goal of the recipient site preparation is to create a geometrically precise, rectangular defect at the palmar base of the middle phalanx. A microsagittal saw or a sharp, fine osteotome is used to create a flat, transverse base in the subchondral bone, perpendicular to the long axis of the middle phalanx. The lateral margins of the defect are squared off to provide a stable, flush bed for the incoming graft.

The dimensions of this prepared defect are precisely measured using a sterile caliper (width, depth, and height). These measurements will dictate the exact size of the graft to be harvested from the hamate. It is imperative to leave the dorsal cortex and the dorsal half of the articular cartilage pristine and undisturbed, as this will serve as the dorsal buttress against which the graft will be compressed.
Hamate Autograft Harvest Technique
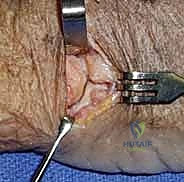
Attention is then directed to the ipsilateral wrist. A longitudinal or slightly curved incision is made over the dorsal aspect of the 4th and 5th carpometacarpal joints, just distal to the pisiform. The extensor retinaculum is incised, and the extensor digitorum communis tendons to the ring and small fingers are retracted laterally.

The dorsal capsule of the 4th and 5th CMC joints is incised longitudinally and elevated subperiosteally to expose the distal articular surface of the hamate. The surgeon must clearly identify the central cartilaginous ridge of the hamate, which separates the articular facets for the 4th and 5th metacarpal bases. This ridge is the anatomical analog to the median ridge of the middle phalanx.

Using the caliper measurements obtained from the finger, the dimensions of the required graft are mapped onto the dorsal-distal hamate. An oscillating microsagittal saw is used to harvest the osteochondral graft. The cuts must be made with extreme precision to avoid fragmenting the graft or damaging the remaining CMC joint surface.
The harvested graft includes the articular cartilage (with the central ridge) and a substantial block of underlying cancellous bone. Following harvest, the donor site defect in the hamate can be left empty or packed with bone wax or local bone graft; it rarely causes significant long-term morbidity.
Graft Contouring, Insertion, and Osteosynthesis
The harvested hamate graft is brought to the back table for final contouring. Using a high-speed burr or fine rongeurs, the cancellous bone of the graft is sculpted to perfectly match the rectangular defect created in the middle phalanx. The graft must fit flush against the dorsal articular step-off and the lateral cortical margins.

The graft is then press-fit into the middle phalanx defect. The articular surface of the graft must be perfectly flush with, or slightly recessed (less than 0.5 mm) relative to, the native dorsal articular cartilage of the middle phalanx. A proud graft will result in a mechanical block to flexion and rapid joint destruction.

Once the optimal position is confirmed, the graft is provisionally secured using one or two 0.028-inch or 0.035-inch Kirschner wires driven from palmar to dorsal.

Definitive osteosynthesis is achieved using two low-profile titanium lag screws (typically 1.0 mm, 1.2 mm, or 1.3 mm in diameter).

The near cortex (the graft) is over-drilled to create a gliding hole, and the far cortex (the dorsal middle phalanx) is under-drilled to create a thread hole. The screws are inserted and carefully tightened to provide rigid interfragmentary compression. The screw heads must be countersunk beneath the cartilage surface to prevent impingement on the proximal phalanx head during flexion.

Following rigid fixation, the PIP joint is reduced. The reduction is assessed both clinically and fluoroscopically. The joint must exhibit smooth, concentric motion throughout a full arc of flexion and extension, with absolutely no dorsal subluxation (the V-sign must be eradicated).

Finally, the volar plate must be repaired to restore the soft tissue restraint against hyperextension. Suture anchors or transosseous sutures are used to secure the distal margin of the volar plate directly to the palmar aspect of the newly reconstructed middle phalanx base.
The flexor tendons are allowed to fall back into position, the tendon sheath is loosely reapproximated if possible, and the skin is closed meticulously.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, hemi-hamate reconstruction is fraught with potential complications. The surgeon must be acutely aware of these risks and prepared to manage them aggressively.
| Complication | Estimated Incidence | Etiology and Pathogenesis | Salvage / Management Strategy |
|---|---|---|---|
| Joint Stiffness (Most Common) | 30% - 50% | Adhesions of the flexor/extensor mechanisms, capsular contracture, prolonged immobilization. | Aggressive hand therapy, dynamic splinting. Surgical tenolysis and capsulotomy if refractory after 6 months. |
| Graft Resorption / Nonunion | 5% - 10% | Avascular necrosis of the graft, inadequate rigid fixation, thermal necrosis during harvest. | Prolonged immobilization. If symptomatic and unstable, conversion to PIP arthrodesis or silicone arthroplasty. |
| Recurrent Instability / Subluxation | 5% - 15% | Undersized graft, failure to repair the volar plate, premature aggressive extension therapy. | Revision surgery with larger graft (rare), or salvage arthrodesis. Strict adherence to dorsal blocking splint protocols. |
| Hardware Prominence / Impingement | 10% - 20% | Failure to adequately countersink screw heads, graft subsidence. | Hardware removal after radiographic confirmation of absolute bony union (typically >3-4 months post-op). |
| Donor Site Morbidity (CMC Joint) | < 5% | Over-harvesting causing CMC instability, localized hematoma, cutaneous nerve neuroma. | Usually self-limiting. Activity modification. Rarely requires CMC arthrodesis. |
Stiffness remains the most ubiquitous and frustrating complication. Because the procedure involves extensive soft tissue dissection and intra-articular work, the propensity for scar formation is immense. The surgeon must balance the need for early motion to prevent stiffness against the need to protect the graft and volar plate repair from excessive tensile forces. If catastrophic failure occurs (e.g., complete graft resorption with recurrent dislocation), the ultimate salvage procedure is a PIP joint arth
