INTRODUCTION TO ACUTE COMPARTMENT SYNDROME
Acute compartment syndrome (ACS) represents one of the most critical surgical emergencies in orthopaedics and trauma surgery. It is defined by an elevation of interstitial pressure within a closed osteofascial compartment that compromises microvascular perfusion, ultimately leading to tissue ischemia, myonecrosis, and irreversible neurological deficit if left untreated. The fundamental biomechanical pathophysiology involves a disruption of the local arteriovenous gradient; as intracompartmental pressure rises, venous outflow is obstructed, leading to further engorgement, exudation of fluid into the interstitial space, and a catastrophic cycle of escalating pressure that eventually collapses the arterial capillary beds.
Early diagnosis and emergent surgical decompression via fasciotomy remain the absolute standard of care. The threshold for intervention is universally guided by the clinical picture combined with intracompartmental pressure monitoring, typically utilizing a Delta P (diastolic blood pressure minus compartment pressure) of less than 30 mm Hg as an absolute indication for immediate release.
🚨 SURGICAL WARNING: Time is tissue. A comprehensive review of fasciotomy outcomes demonstrates that 68% of patients treated within 12 hours of symptom onset achieve normal function. In stark contrast, only 8% of patients treated more than 12 hours after symptom onset regain normal function. Delayed fasciotomy not only guarantees severe functional deficits but also significantly increases the risk of life-threatening complications such as rhabdomyolysis, acute renal failure, and the need for amputation.
EPIDEMIOLOGY AND RISK FACTORS
The etiology of compartment syndrome is diverse, though the most common cause remains blunt soft tissue injury and high-energy trauma. Over a 10-year retrospective analysis at a major Level I trauma center, 288 (2.8%) of 10,315 patients presenting with extremity trauma required therapeutic fasciotomy for compartment syndrome.
The necessity for fasciotomy varies significantly based on the mechanism and morphology of the injury:
* Motor Vehicle Accidents: < 1% incidence.
* Closed Fractures: 2% incidence.
* Gunshot Wounds: Approximately 9% incidence.
* Combined Vascular Injuries: Up to 42% incidence, representing the highest risk cohort due to ischemia-reperfusion injury.
Independent predictors for the development of ACS include male sex and age younger than 55 years, likely due to larger baseline muscle mass confined within unyielding fascial envelopes. Furthermore, an increasingly prevalent risk factor in contemporary trauma practice is the use of systemic anticoagulation therapy in elderly patients, which can precipitate spontaneous or low-energy compartment syndromes secondary to uncontained intramuscular hemorrhage.
Even with timely and flawlessly executed fasciotomies, patients frequently experience long-term sequelae. These include altered sensation, chronic dependent swelling, neuropathic pain, functional motor deficits, and significant cosmetic concerns related to the fasciotomy scars and subsequent skin grafting.
FASCIOTOMY FOR ACUTE COMPARTMENT SYNDROME OF THE THIGH
The thigh is anatomically divided into three distinct compartments: anterior, posterior, and medial. Because the thigh compartments possess a larger volume and greater compliance than those of the leg, thigh compartment syndrome is relatively rare. However, when it occurs, it is typically the result of massive blunt trauma, femur fractures, or prolonged compression.
Preoperative Preparation and Positioning
- Positioning: The patient is placed in the supine position on a radiolucent operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg slightly, providing optimal access to the lateral aspect of the thigh.
- Preparation: Prepare and drape the entire lower extremity in a standard sterile fashion, ensuring exposure from the iliac crest proximally to the knee joint distally. Free draping of the limb is essential to allow for manipulation during the procedure.
Surgical Technique: Thigh Decompression (Tarlow et al.)
The standard approach for thigh decompression utilizes a single extensive lateral incision to access both the anterior and posterior compartments, with a secondary medial incision reserved for specific medial compartment involvement.
-
Step 1: The Skin Incision
Make a longitudinal lateral incision beginning just distal to the intertrochanteric line and extending distally to the lateral epicondyle of the femur. This extensive incision is mandatory to ensure complete release of the fascial envelope.
-
Step 2: Releasing the Anterior Compartment
Deepen the dissection through the subcutaneous tissues to expose the glistening white fibers of the iliotibial band. Make a straight, longitudinal incision directly in line with the skin incision through the iliotibial band and the underlying fascia lata. This maneuver effectively decompresses the anterior compartment.
-
Step 3: Accessing the Posterior Compartment
Carefully reflect the vastus lateralis muscle off the lateral intermuscular septum. Retract the muscle belly medially and anteriorly.💡 CLINICAL PEARL: During the reflection of the vastus lateralis, you will encounter multiple perforating branches from the profunda femoris artery. It is critical to meticulously identify, clamp, and coagulate or ligate all perforating vessels to prevent massive postoperative hemorrhage, which could paradoxically recreate a hematoma-driven compartment syndrome.
-
Step 4: Releasing the Posterior Compartment
Once the lateral intermuscular septum is clearly visualized, make a 1.5-cm initiating incision through the septum. Using heavy Metzenbaum scissors, extend this fascial release proximally and distally for the entire length of the surgical incision to fully decompress the posterior compartment.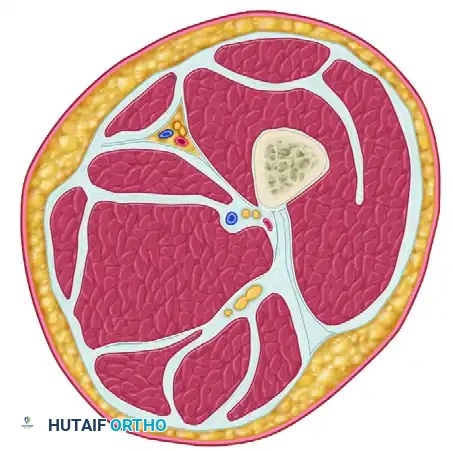
-
Step 5: Evaluating the Medial Compartment
After the anterior and posterior compartments have been thoroughly released, it is imperative to measure the intracompartmental pressure of the medial (adductor) compartment using a handheld manometer or arterial line setup. If the pressure remains elevated (Delta P < 30 mm Hg), a separate longitudinal medial incision must be made to release the adductor fascial envelope.
FASCIOTOMY FOR ACUTE COMPARTMENT SYNDROME OF THE LEG
The lower leg is the most common anatomical site for acute compartment syndrome. It consists of four rigid compartments: Anterior, Lateral, Superficial Posterior, and Deep Posterior.
Historically, some institutions managed leg ACS with selective releases based on continuous pressure monitoring. For instance, protocols where orthopaedic residents checked patients every 2 hours and repeated measurements if symptomatology changed showed that only 8% of patients strictly required a posterior release. However, the immense clinical resources required to follow patients this closely—and the catastrophic medicolegal and functional consequences of a missed deep posterior compartment syndrome—make this approach impractical for most centers.
🚨 SURGICAL WARNING: The contemporary gold standard and safest approach for the vast majority of patients is the prophylactic and therapeutic release of all four compartments during the index operation.
Surgical Technique: Four-Compartment Decompression (Davey, Rorabeck, and Fowler)
This technique utilizes a single, highly expansile lateral incision to access all four compartments of the lower leg. While a two-incision technique (anterolateral and posteromedial) is also widely accepted, the single lateral approach described by Davey et al. is highly effective when performed with precise anatomical knowledge.
-
Step 1: The Lateral Skin Incision
Make a generous lateral skin incision beginning proximally at the level of the fibular neck and extending distally to approximately 3 to 4 cm proximal to the lateral malleolus.
-
Step 2: Anterior and Lateral Compartment Release
Undermine the skin anteriorly to expose the fascia overlying the anterior and lateral compartments. Identify the anterior intermuscular septum dividing these two compartments. Perform a longitudinal fasciotomy of the anterior compartment, taking care to protect the superficial peroneal nerve, which exits the lateral compartment to become subcutaneous in the distal third of the leg. Subsequently, perform a longitudinal fasciotomy of the lateral compartment.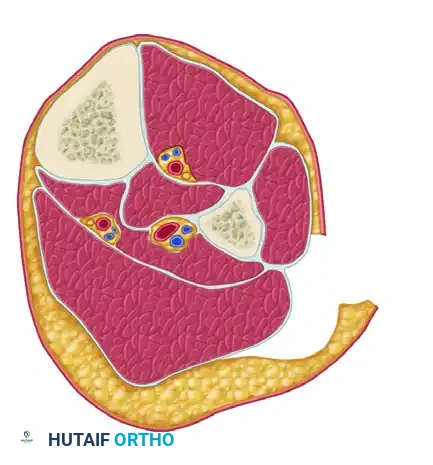
-
Step 3: Superficial Posterior Compartment Release
Undermine the skin posteriorly from the primary incision to expose the fascia of the superficial posterior compartment (containing the gastrocnemius and soleus muscles). Perform a longitudinal fasciotomy to release this compartment.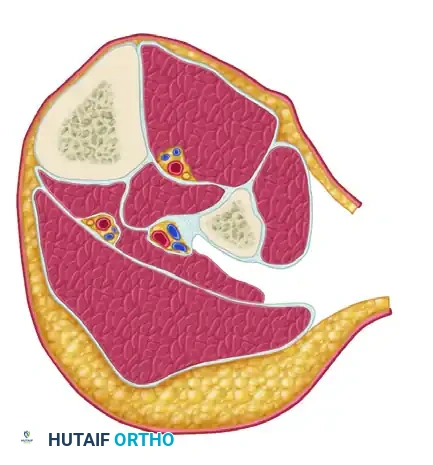
-
Step 4: Deep Posterior Compartment Release
This is the most technically demanding step. Develop the interval between the superficial posterior compartment and the lateral compartment. Identify the fibula. The flexor hallucis longus (FHL) muscle must be dissected subperiosteally off the posterior aspect of the fibula and retracted posteromedially. Once retracted, identify the deep fascial attachment of the tibialis posterior muscle to the fibula. Incise this fascia longitudinally to completely decompress the deep posterior compartment.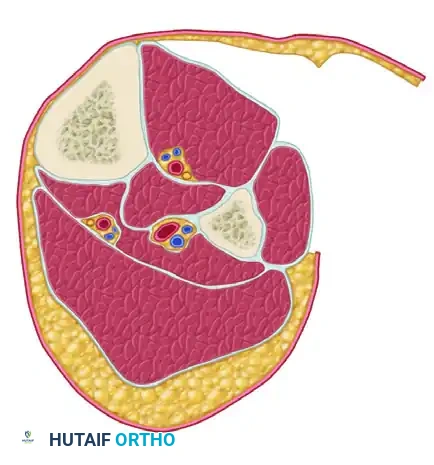
POSTOPERATIVE MANAGEMENT AND WOUND CARE
The completion of the fasciotomy is only the first phase of managing acute compartment syndrome. Meticulous postoperative care is critical to preventing infection, managing fluid shifts, and achieving definitive soft tissue coverage.
Immediate Postoperative Care
Following decompression, the wounds must never be closed acutely. The muscle will inevitably swell further due to reperfusion hyperemia.
* Pack the wounds open with sterile, moist saline gauze and apply a large, bulky, non-constricting dressing.
* Alternatively, and increasingly preferred in modern trauma bays, a Negative Pressure Wound Therapy (NPWT) device (e.g., VAC dressing) can be applied at 50 to 75 mm Hg continuous pressure. NPWT helps manage the significant exudate, reduces interstitial edema, and prevents skin edge retraction.
The "Second Look" Operation
At 48 to 72 hours post-index procedure, the patient must be returned to the operating room for a planned second look.
* Viability Assessment: The muscle beds are irrigated and meticulously inspected for viability using the "4 C's": Color, Consistency, Contractility, and Capacity to bleed.
* Adjunctive Diagnostics: Intravenous fluorescein dye combined with a Wood's light examination can be highly beneficial in evaluating borderline muscle viability. Non-fluorescing, necrotic muscle must be aggressively debrided to prevent systemic toxicity and deep infection.
Definitive Closure
- If there is absolutely no evidence of muscle necrosis and the swelling has subsided sufficiently, the skin may be loosely closed using a delayed primary closure technique or vessel loops (the "shoelace" technique) to gradually approximate the margins.
- If closure cannot be accomplished without tension, the debridement and NPWT application are repeated after another 48- to 72-hour interval.
- Ultimately, most extensive fasciotomy wounds will require definitive coverage with a Split-Thickness Skin Graft (STSG) once a healthy, granulating wound bed is established.
CONCLUSION
Fasciotomy for acute compartment syndrome is a limb-saving and potentially life-saving intervention. Orthopaedic surgeons must maintain a high index of suspicion, particularly in high-energy trauma, vascular injuries, and anticoagulated patients. Mastery of the expansile anatomical approaches to the thigh and the four compartments of the leg ensures adequate decompression. Coupled with aggressive postoperative wound management and timely second-look debridements, these surgical techniques provide the best possible chance for preserving limb function and mitigating the devastating complications of ischemic contracture.
📚 Medical References
- Acute compartment syndrome of the thigh in a football athlete: a case report and the role of vacuum-assisted wound closure dressing, J Orthop Trauma 19:749, 2005.
- Leversedge SJ, Casey PJ, Seiler JG 3rd, Xerogeanes JW: Endoscopically assisted fasciotomy: description of technique and in vitro assessment of lower-leg compartment decompression, Am J Sports Med 30:272, 2002.
- Lohrer H, Nauck T: Endoscopically assisted release for exertional compartment syndromes of the lower leg, Arch Orthop Trauma Surg Feb 6, 2007.
- Luk KDK, Pun WK: Unrecognized compartment syndrome in a patient with tourniquet palsy, J Bone Joint Surg 69B:97, 1987.
- Martens MA, Backaert M, Vermaut G, et al: Chronic leg pain in athletes due to a recurrent compartment syndrome, Am J Sports Med 12:148, 1984.
- Matsen FA III: Pathophysiology of compartment syndromes, Instr Course Lect 38:463, 1989.
- Matsen FA III, Wyss CR, King RV, et al: Factors affecting the tolerance of muscle circulation and function for increased tissue pressure, Clin Orthop Relat Res 155:224, 1981.
- Mouhsine E, Garofalo R, Moretti B, et al: Two minimal incision fasciotomy for chronic exertional compartment syndrome of the lower leg, Knee Surg Sports Traumatol Arthrosc 14:193, 2006.
- Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: a cause of shin splints, Am J Sports Med 10:201, 1982.
- Mubarak SJ, Hargens AR: Compartment syndromes and Volkmann’s contracture. In Saunder’s monographs in clinical orthopaedics, vol 3, Philadelphia, 1981, Saunders. Mubarak SJ, Owen CA: Compartmental syndrome and its relation to the crush syndrome, a spectrum of disease: a review of 11 cases of prolonged limb compression, Clin Orthop Relat Res 113:81, 1975.
- Nkele C, Aindow J, Grant L: Study of pressure of the normal anterior tibial compartment in different age groups using the slit-catheter method, J Bone Joint Surg 70A:98, 1988.
- Olson SA, Glasgow RR: Acute compartment syndrome in lower extremity musculoskeletal trauma, J Am Acad Orthop Surg 13:436, 2005.
- Pedowitz RA, Hargens AR, Mubarak SJ, et al: Modifi ed criteria for the objective diagnosis of chronic compartment syndrome of the leg, Am J Sports Med 18:35, 1990.
- Pell RF IV, Khanuja HS, Cooley GR: Leg pain in the running athlete, J Am Acad Orthop Surg 12:396, 2004.
- Petrik ME, Stambough JL, Rothman RH: Posttraumatic gluteal compartment syndrome: a case report, Clin Orthop Relat Res 231:127, 1988.
- Prayson MJ, Chen JL, Hampers D, et al: Baseline compartment pressure measurements in isolated
