Comprehensive Introduction and Patho-Epidemiology
The evolution of hip preservation surgery has been defined by a continuous refinement of our understanding regarding the complex interplay between acetabular morphology, femoral version, and capsulolabral integrity. While hip arthroscopy has revolutionized the management of isolated femoroacetabular impingement (FAI) and labral pathology, its application in the setting of unrecognized or underappreciated structural instability has led to a rising cohort of patients presenting with catastrophic iatrogenic deterioration. The clinical scenario of "complex instability" often emerges when arthroscopic interventions—particularly labral resection or overzealous rim trimming—are erroneously applied to hips harboring underlying dysplastic features or severe torsional abnormalities.
Consider the classic, highly challenging demographic: a young adult female, typically in her early thirties with a normal body mass index, presenting with progressive, debilitating hip pain following a prior arthroscopic procedure. In these patients, the initial arthroscopy often involved a labral resection rather than repair, fundamentally compromising the hip's primary fluid seal and secondary static stabilizer. The underlying pathoanatomy frequently reveals a triad of structural deficiencies: residual anterolateral acetabular dysplasia, excessive femoral anteversion, and subsequent anterolateral articular cartilage delamination. When the labrum—which hypertrophies in dysplastic hips to bear aberrant axial loads—is resected, the femoral head is permitted to translate anteriorly and laterally, accelerating chondral sheer and capsular attenuation.

Epidemiologically, borderline and frank acetabular dysplasia (defined by a Lateral Center Edge Angle [LCEA] of less than 25° and 20°, respectively) combined with femoral torsion abnormalities represent a significant proportion of the young adult hip pain population. High femoral anteversion (often exceeding 35° to 40°) exacerbates anterior uncoverage. During dynamic activities such as synchronized swimming, skiing, or general fitness, the hip is subjected to extreme ranges of motion. In forced extension and external rotation, the anteriorly directed femoral head lacks both the bony containment of a normal anterior acetabular wall and the soft-tissue restraint of the resected labrum. This results in profound microinstability, clinically manifesting as a positive apprehension test and a subjective feeling of the hip "giving way."

Surgical Hip Dislocation (SHD), pioneered by Reinhold Ganz and colleagues, remains the gold standard and the definitive "beyond arthroscopy" intervention for these complex, multi-planar deformities. SHD provides unparalleled, 360-degree visualization of the femoral head and acetabulum while preserving the critical extra-osseous blood supply to the femoral head. In the setting of failed arthroscopy with complex instability, SHD allows the surgeon to perform comprehensive intra-articular work—such as labral reconstruction using allograft or autograft and meticulous osteochondroplasty—while serving as the foundational approach for concomitant structural realignments, including Periacetabular Osteotomy (PAO) and femoral derotation osteotomy.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the vascular, osseous, and capsuloligamentous anatomy of the hip is the absolute prerequisite for performing a safe and effective surgical hip dislocation. The most critical anatomical structure in this operation is the medial circumflex femoral artery (MFCA). The MFCA originates from the profunda femoris and courses posteriorly, passing between the pectineus and iliopsoas, and then between the obturator externus and quadratus femoris. Its deep branch crosses the posterior aspect of the obturator externus tendon to enter the trochanteric fossa, giving rise to the retinacular vessels that travel along the posterosuperior femoral neck. The Ganz trochanteric flip osteotomy is explicitly designed to protect this vascular leash by keeping the external rotators (specifically the obturator externus and internus) intact, thus preventing tension or disruption of the MFCA during anterior dislocation.
From an osseous perspective, the normal adult hip relies on a delicate balance of version and coverage. The acetabulum is typically anteverted approximately 15° to 20°, with a normal LCEA between 25° and 39°, and a roof inclination angle approaching zero. The proximal femur normally exhibits 10° to 15° of anteversion. In our complex instability cohort, this relationship is severely distorted. A patient may present with an LCEA of 18° (frank dysplasia) and a roof inclination of 20° (a steep, up-sloping sourcil), leading to a severely diminished weight-bearing surface area. When this is compounded by high femoral anteversion—such as 36° measured on MRI—the femoral head is driven anteriorly. This creates a functional anterior uncoverage that is exponentially worse than the radiographic coronal measurements imply.
Biomechanically, the hip joint stability is maintained by the bony architecture, the labrum, the capsule, and the dynamic musculature. In the dysplastic hip, the bony architecture is deficient, placing an enormous, unnatural demand on the labrum and the iliofemoral ligament. The labrum functions not only to deepen the socket but to maintain a negative intra-articular pressure (the fluid seal), which distributes synovial fluid and reduces cartilage consolidation under load. When a surgeon performs an arthroscopic labral resection in a dysplastic hip, the fluid seal is permanently destroyed. The femoral head immediately begins to micro-subluxate anterolaterally during the gait cycle.
This microinstability leads to a highly specific pattern of cartilage failure. The anterolateral acetabular cartilage experiences massive shear forces, leading to chondral delamination and full-thickness loss. Concurrently, the anterior capsule and iliofemoral ligament become stretched and incompetent. Clinically, this is why the patient experiences a positive apprehension sign in forced extension and external rotation; the anterior restraints are completely absent. Furthermore, the patient may exhibit a positive impingement test (pain in flexion and internal rotation) not necessarily due to a CAM lesion, but because the unstable femoral head translates abnormally within the joint, causing the femoral neck to abut the anterior acetabular rim prematurely (impingement-induced instability or instability-induced impingement).
Exhaustive Indications and Contraindications
The decision to proceed with a surgical hip dislocation, particularly when combined with complex osteotomies, requires meticulous patient selection. The procedure is highly demanding and carries significant morbidity if performed on the wrong candidate. The primary indication is complex intra-articular pathology that cannot be adequately addressed via arthroscopy, especially when combined with structural deformities requiring open realignment.

Patients presenting with failed prior arthroscopy, iatrogenic instability, and an absent labrum in the setting of borderline or frank dysplasia are prime candidates. In these cases, the surgeon must reconstruct the labrum (using fascia lata, semitendinosus, or allograft) and correct the bony deformity. Another major indication is the presence of severe torsional abnormalities (e.g., femoral anteversion >30° or severe retroversion) that require a derotational femoral osteotomy. Furthermore, large, globally extending CAM lesions, severe slipped capital femoral epiphysis (SCFE) deformities, and Perthes-like deformities with coxa magna are classic indications for SHD.
Conversely, strict contraindications exist. Advanced osteoarthritis is an absolute contraindication; hips with Tönnis grade 2 or 3 changes, joint space narrowing less than 2mm, or extensive cystic changes in both the femoral head and acetabulum will predictably fail and should be directed toward total hip arthroplasty (THA). Advanced chronological age (typically >45-50 years, though physiological age is more critical) and severe osteopenia or osteoporosis are relative to absolute contraindications due to the risk of trochanteric non-union and poor bone healing at osteotomy sites.
| Parameter | Favorable Indications for SHD | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Joint Space / OA | Tönnis Grade 0 or 1; Joint space > 2mm | Tönnis Grade 2 or 3; Joint space < 2mm | Diffuse chondral thinning on MRI without bone-on-bone |
| Pathomorphology | Complex CAM, SCFE, Perthes, High Anteversion | Global head necrosis, severe flattening | Borderline dysplasia without instability symptoms |
| Previous Surgery | Failed arthroscopy, iatrogenic labral absence | Prior joint infection, severe arthrofibrosis | Multiple prior open hip surgeries with severe scarring |
| Patient Factors | Young, active, compliant with strict rehab | Non-compliant, active smoking, severe obesity | Age > 45 years, moderate osteopenia |
| Instability | Apprehension, microinstability, capsular laxity | Charcot arthropathy, connective tissue disorders | Generalized benign hypermobility syndrome |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of success in complex hip reconstruction. The clinical examination must meticulously document the patient's range of motion, provocative signs, and neurological status. A positive anterior impingement test (flexion, adduction, internal rotation) coupled with a positive apprehension test (extension, external rotation) strongly suggests a combination of structural impingement and anterior instability. The patient's gait should be analyzed for an abductor lurch or an internally rotated foot progression angle, which is a classic compensatory mechanism for high femoral anteversion.

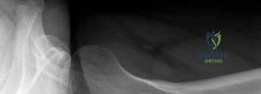
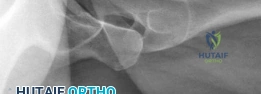
Radiographic assessment must be exhaustive. A standardized anteroposterior (AP) radiograph of the pelvis, centered over the symphysis pubis with neutral pelvic tilt and rotation, is mandatory. On this view, the LCEA, Tönnis roof inclination angle, and extrusion index are calculated. For instance, an LCEA of 18° and a roof inclination of 20° confirm severe lateral and superior uncoverage. A false profile view of the Lequesne and de Sèze is critical for assessing anterior coverage (anterior center-edge angle) and anterior joint space. Dunn 45° and 90° views, or a cross-table lateral, are utilized to evaluate the femoral head-neck junction for CAM morphology.
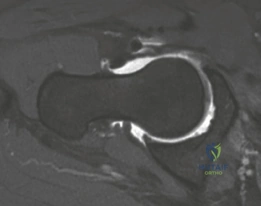
Advanced imaging is non-negotiable in the revision setting. A high-resolution MRI or MR arthrogram of the hip is required to assess the articular cartilage, the integrity of the ligamentum teres, and the state of the remaining labrum or capsular scar tissue. Anterolateral loss of joint cartilage is a frequent finding in dysplastic hips post-labral resection. Furthermore, a CT scan or MRI utilizing torsional sequences from the hip through the knee is essential to quantify femoral version. A measured femoral anteversion of 36° dictates that a derotational femoral osteotomy (DFO) must be incorporated into the surgical plan to restore normal biomechanics and prevent recurrent anterior subluxation post-operatively.
Patient positioning depends on the planned concomitant procedures. If an isolated SHD with a proximal femoral derotation osteotomy is planned, the patient is placed in the lateral decubitus position on a radiolucent table, utilizing a beanbag and rigid pelvic positioners. The leg must be draped free to allow full manipulation. However, if a Periacetabular Osteotomy (PAO) is required to correct the acetabular dysplasia (e.g., LCEA of 18°), the patient is typically positioned supine or in a "floppy lateral" position. The floppy lateral allows the surgeon to roll the patient backward to perform the anterior approaches required for the PAO after the SHD and femoral work are completed. Fluoroscopy must be easily accessible and unimpeded in all planes.
Step-by-Step Surgical Approach and Fixation Technique
The Ganz surgical hip dislocation is a highly orchestrated procedure that demands meticulous tissue handling. The approach begins with a straight lateral incision centered over the greater trochanter. The subcutaneous tissues are divided, and the fascia lata is incised in line with the skin incision. The interval between the gluteus maximus and the tensor fasciae latae (the Gibson interval) is developed. The gluteus maximus is retracted posteriorly, exposing the posterior border of the gluteus medius and the short external rotators.

The critical step is the digastric trochanteric flip osteotomy. The posterior border of the gluteus medius is identified, and the interval between the medius and piriformis is developed. The osteotomy is initiated at the posterosuperior tip of the greater trochanter, ensuring that the piriformis tendon remains attached to the stable proximal femur, while the gluteus medius, gluteus minimus, and vastus lateralis remain attached to the mobile trochanteric fragment. The osteotomy is directed distally and anteriorly, exiting just proximal to the vastus ridge. The thickness of the trochanteric fragment should be approximately 1.5 cm. Once the osteotomy is complete, the mobile fragment is flipped anteriorly. The underlying gluteus minimus is meticulously elevated off the hip capsule.

With the trochanter flipped, the superior, anterior, and posterior aspects of the hip capsule are exposed. To protect the retinacular vessels, which run along the posterosuperior neck, the capsulotomy must be performed with extreme care. A Z-shaped capsulotomy is standard for the right hip (reverse Z for the left). The longitudinal limb is made along the anterosuperior axis of the femoral neck, staying well away from the posterosuperior retinacular vessels. The proximal limb runs along the acetabular rim, and the distal limb runs inferiorly. Heavy sutures are placed in the capsular flaps for later repair.

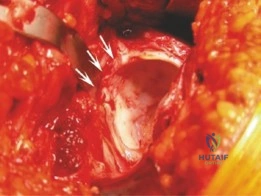
Dislocation of the femoral head is achieved by flexion, adduction, and external rotation of the leg. The ligamentum teres, if intact, is sharply transected using specialized curved scissors. Once dislocated, the femoral head and acetabulum are inspected. In our index case, significant anterolateral cartilage loss and an absent labrum are encountered. The acetabular rim is prepared, and a labral reconstruction is performed. An allograft (e.g., semitendinosus) or autograft (iliotibial band) is tubularized and secured to the acetabular rim using multiple knotless suture anchors. This restores the critical fluid seal and anterior bumper. Concurrently, any abnormal CAM morphology on the femoral head-neck junction is addressed via osteochondroplasty using high-speed burrs and curved osteotomes, ensuring spherical congruence.
If the patient requires a derotational femoral osteotomy to correct the 36° anteversion, it is performed at this stage. A subtrochanteric osteotomy is executed, the femur is externally rotated to achieve a normalized anteversion of approximately 15°, and rigid fixation is achieved using a pre-contoured locking plate or a blade plate. Following the intra-articular and femoral work, the hip is reduced. The capsule is meticulously closed; a watertight closure is essential to prevent post-operative macro-instability and restore the proprioceptive function of the capsule. Finally, the greater trochanter is reduced and fixed using two or three fully threaded 4.5 mm cortical screws directed medially and slightly proximally toward the lesser trochanter.
Complications, Incidence Rates, and Salvage Management
Despite its elegance, surgical hip dislocation is a major open joint procedure with a distinct complication profile. The most feared complication, avascular necrosis (AVN) of the femoral head, is historically the primary reason surgeons avoided open hip dislocation. However, with strict adherence to the Ganz technique—specifically the protection of the external rotators and the precise placement of the capsulotomy—the incidence of iatrogenic AVN is remarkably low, documented at less than 1% in high-volume tertiary centers.

Trochanteric non-union or delayed union is a more common complication, occurring in 1% to 3% of cases. It is often related to inadequate fixation, poor bone quality, or premature active abduction during the rehabilitation phase. Patients present with persistent lateral hip pain, a profound abductor lurch, and weakness. Management involves revision internal fixation, often augmented with bone grafting and tension band wiring. Heterotopic ossification (HO) occurs in up to 10% of patients, though clinically significant, motion-limiting HO (Brooker Class III or IV) is rare. Routine prophylaxis with non-steroidal anti-inflammatory drugs (e.g., Indomethacin or Celecoxib for 3-4 weeks post-operatively) is mandatory.
Nerve injury, particularly to the sciatic nerve, is a risk during the posterior retraction required for the approach or secondary to hematoma formation. The incidence is approximately 1-2%, and it is usually a transient neurapraxia that resolves with conservative management and time. Progressive osteoarthritis is the ultimate mode of failure. In patients with unrecognized high-grade chondral damage at the time of surgery, the joint may continue to degenerate despite perfect structural correction. When the hip progresses to Tönnis grade 3 or the patient experiences intractable pain, the salvage procedure is a Total Hip Arthroplasty (THA). Fortunately, prior SHD does not significantly compromise the outcomes of subsequent THA, though hardware removal (trochanteric screws, osteotomy plates) may add complexity to the arthroplasty.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention & Salvage Management |
|---|---|---|---|
| Avascular Necrosis (AVN) | < 1.0% | Disruption of MFCA or retinacular vessels | Meticulous capsulotomy; Salvage: THA |
| Trochanteric Non-union | 1.0% - 3.0% | Poor fixation, early active abduction | 3-screw fixation, strict rehab; Salvage: Revision ORIF + graft |
| Heterotopic Ossification | 5.0% - 10.0% | Muscle trauma, inadequate prophylaxis | Gentle tissue handling, NSAIDs; Salvage: Surgical excision if mature |
| Sciatic Nerve Neurapraxia | 1.0% - 2.0% | Overzealous posterior retraction, hematoma | Careful retractor placement; Salvage: Observation, AFO for foot drop |
| Progression to Osteoarthritis | 10.0% at 10 yrs | Pre-existing chondral damage, undercorrection | Strict patient selection; Salvage: Total Hip Arthroplasty (THA) |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following a surgical hip dislocation, particularly when combined with labral reconstruction and femoral or acetabular osteotomies, is inherently conservative and requires profound patient compliance. The protocol is divided into four distinct phases, spanning a minimum of six to nine months before a return to high-impact sports or extreme ranges of motion (e.g., synchronized swimming or skiing) can be considered.

Phase 1: Maximum Protection (Weeks 0 to 6)
The primary goals in the initial phase are the protection of the trochanteric osteotomy, the capsular repair, and any reconstructed labral tissue. Weight-bearing is strictly limited to toe-touch (approx. 20 lbs) using crutches. Active abduction is absolutely contraindicated to prevent displacement of the greater trochanter. Range of motion is initiated immediately using continuous passive motion (CPM) machines or circumduction exercises, but flexion is typically limited to 90°, and external rotation is restricted to neutral to protect the anterior capsular closure. Isometrics for the quadriceps, hamstrings, and gluteus maximus are encouraged.
Phase 2: Early Mobilization and Strengthening (Weeks 6 to 12)
At the six-week mark, radiographic confirmation of trochanteric and osteotomy site healing is obtained. Once bridging callus is visualized, the patient is gradually transitioned to weight-bearing as tolerated. Crutches are weaned as the patient demonstrates a non-antalgic, trendelenburg-free gait. Active abduction is initiated, starting in the supine position and progressing to standing. Closed kinetic chain exercises, such as mini-squats and leg presses (limited depth), are introduced. Stationary cycling with low resistance is utilized to enhance synovial fluid diffusion and improve range of motion.
Phase 3: Advanced Strengthening and Proprioception (Months 3 to 5)
With full weight-bearing established and normalized gait mechanics, the focus shifts to restoring core stability, pelvic control, and dynamic balance. Advanced abductor strengthening is prioritized to combat the profound atrophy that often accompanies chronic hip dysplasia and prolonged modified weight-bearing. Single-leg stance activities, balance board training, and dynamic step-ups are incorporated. The patient begins light straight-line jogging and elliptical training. Range of motion should be nearing symmetry with the contralateral side, though terminal extremes may still provoke mild discomfort.
Phase 4: Return to Sport and High-Level Function (Months 6+)
The final phase is highly individualized based on the patient's specific athletic goals. For a patient wishing to return to synchronized swimming and skiing, extreme demands will be placed on the capsuloligamentous complex and the newly reconstructed labrum. Sport-specific agility drills, plyometrics, and cutting maneuvers are introduced under the supervision of a physical therapist. A functional movement screen and objective isokinetic strength testing (requiring >85% symmetry compared to the uninjured limb) are recommended before full medical clearance is granted. The patient must understand that while the structural instability has been corrected, the joint has experienced significant prior trauma, and long-term joint preservation requires ongoing muscular maintenance.
Summary of Landmark Literature and Clinical Guidelines
The foundation of open hip preservation surgery rests upon the landmark 2001 publication by Ganz, Gill, Gautier, et al., in Clinical Orthopaedics and Related Research, which detailed the surgical technique and vascular safety of the surgical hip dislocation. This paper fundamentally shifted the paradigm, proving that the hip could be safely dislocated without inducing avascular necrosis, provided the deep branch of the medial circumflex femoral artery was protected via the digastric trochanteric flip osteotomy.
In the context of the specific pathology discussed in this chapter—failed arthroscopy in the dysplastic hip—the literature has become increasingly definitive. Studies by Parvizi et al. and Matsuda et al. have rigorously documented the high failure rates of isolated arthroscopy in patients with borderline or frank acetabular dysplasia. They highlighted that arthroscopic labral debridement or resection in an under-covered hip removes the essential "O-ring" seal and the primary anterior stabilizer, leading to rapid, catastrophic microinstability and accelerated chondrolysis. These findings have culminated in modern clinical guidelines that strongly contraindicate isolated arthroscopic labral resection in the setting of structural instability.
Furthermore, the impact of femoral version on hip biomechanics has been extensively studied by researchers such as Clohisy and Lerch. High femoral anteversion (as seen in our 36° index case) is now recognized as a major independent driver of anterior hip instability and impingement. The current consensus dictates that three-dimensional deformities require three-dimensional solutions. When a patient presents with the triad of dysplasia, high anteversion, and an incompetent labrum, comprehensive open reconstruction—utilizing surgical hip dislocation for intra-articular repair, combined with appropriate osseous realignments (PAO and DFO)—represents the only biomechanically sound strategy to achieve long-term joint preservation and clinical success.
