Introduction and Pathoanatomy
Congenital metatarsus adductus is one of the most frequently encountered pediatric foot anomalies, characterized primarily by the adduction of the forefoot in relation to a normal midfoot and hindfoot. This structural deviation is a leading cause of in-toeing in infants and young children. While it frequently presents as an isolated anomaly, it is also commonly observed in association with other congenital deformities, most notably congenital talipes equinovarus (clubfoot).
A critical clinical pearl for the practicing orthopedic surgeon is the established association between metatarsus adductus and developmental dysplasia of the hip (DDH). Epidemiological data indicates that 1% to 5% of individuals presenting with metatarsus adductus also harbor concurrent DDH or acetabular dysplasia. Consequently, a thorough clinical and, if indicated, ultrasonographic evaluation of the hips is mandatory in these patients.
Biomechanically, unresolved metatarsus adductus alters the normal weight-bearing axis of the foot. Late sequelae in untreated or residual cases include an increased risk of stress fractures of the lateral metatarsal bones. Theodorou et al. documented a direct association between metatarsus adductus deformity and lateral metatarsal stress fractures in adult patients (aged 25 to 61 years), attributing this pathology to altered foot biomechanics that place disproportionately greater loads across the lateral column during the terminal stance phase of gait.
Clinical Evaluation and Classification
The clinical presentation of metatarsus adductus ranges from a highly flexible, mild deformity to a rigid, structural anomaly. Physical examination must differentiate between dynamic adduction (often caused by an overactive or imbalanced anterior tibial tendon during gait) and fixed, rigid positioning of the forefoot on the midfoot.
In severe cases, examiners will frequently note a deep transverse crease on the medial border of the foot, indicating severe soft-tissue contracture, alongside a noticeable enlargement of the web space between the great and second toes.
Clinical Pearl: The rigidity or flexibility of the forefoot must be definitively determined before undertaking any surgical correction, particularly in older children. Dynamic deformities may respond to tendon transfers, whereas rigid deformities necessitate osteotomies.
The Bleck Classification System
Metatarsus adductus is clinically stratified into mild, moderate, or severe categories based on the heel bisector method described by Bleck. This is assessed by viewing the plantar aspect of the weight-bearing foot and drawing a longitudinal line bisecting the heel.

Fig. 1: The heel bisector defines the relationship of the heel to the forefoot. From left to right: normal (bisecting second and third toes), mild metatarsus adductus (bisecting third toe), moderate metatarsus adductus (bisecting third and fourth toes), and severe metatarsus adductus (bisecting fourth and fifth toes).
- Mild Metatarsus Adductus: The heel bisector line passes through the third toe. Clinically, the forefoot can be passively abducted to the midline of the foot and beyond.
- Moderate Metatarsus Adductus: The heel bisector line passes between the third and fourth toes. The forefoot possesses enough flexibility to allow passive abduction to the midline, but usually not beyond.
- Severe (Rigid) Metatarsus Adductus: The heel bisector line passes through the fourth or fifth toe. The forefoot is rigid and cannot be passively abducted to the midline.

Fig. 2: Clinical presentation of congenital metatarsus adductus. Left: Mild deformity. Right: Moderate deformity.

Fig. 3: Severe congenital metatarsus adductus. Note the deep medial transverse crease indicative of severe medial soft-tissue contracture.

Fig. 4: Radiographic appearance of severe metatarsus adductus, demonstrating significant medial deviation of the metatarsal shafts relative to the midfoot.
Associated Forefoot Anomalies: Congenital Hallux Varus
In certain complex presentations, severe metatarsus adductus with an enlarged first web space may present concurrently with or mimic congenital hallux varus. When the great toe is severely adducted and structurally tethered, specific soft-tissue reconstruction is required. The Farmer procedure and its alternatives are utilized to correct the first web space contracture and realign the hallux.
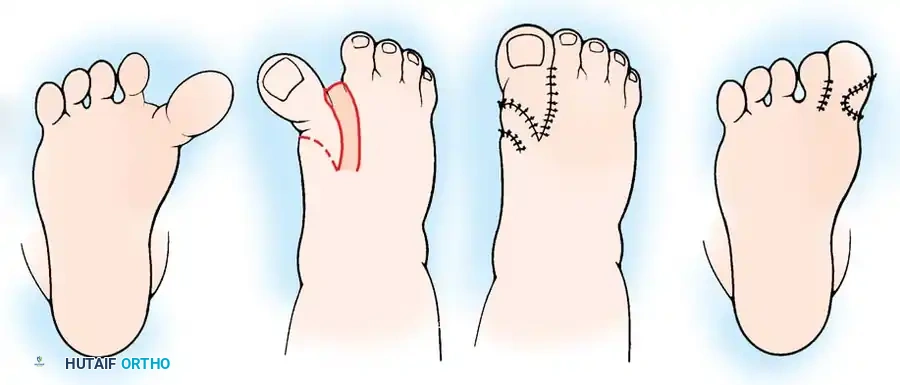
Fig. 5: The Farmer procedure for congenital hallux varus, utilizing a rotational skin flap to deepen the first web space and correct the medial tethering.
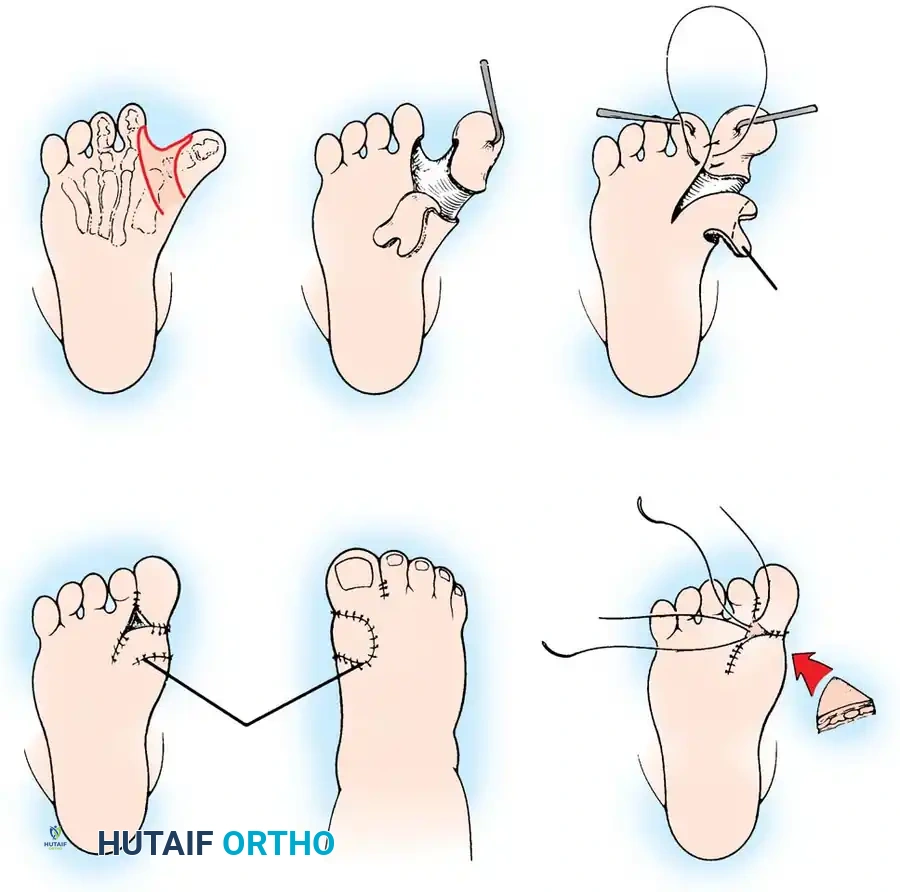
Fig. 6: Alternative Farmer procedure for congenital hallux varus, demonstrating the incision, capsular release, flap transposition, and application of a full-thickness skin graft.
Conservative Management
The natural history of mild metatarsus adductus is highly favorable, with the vast majority of cases resolving spontaneously without intervention.
For moderate or severe deformities, the gold standard of initial treatment is serial stretching and casting. This is most effective when initiated early in infancy. The protocol typically involves below-knee plaster casting, changed every 1 to 2 weeks, for a total duration of 6 to 12 weeks, or until the foot demonstrates clinical flexibility. Katz et al. demonstrated high efficacy with this approach, reporting successful correction in 65 infants with moderate or severe deformities treated with below-knee casting.
Surgical Indications and Decision Making
Surgical intervention is strictly reserved for cases where conservative treatment has failed, and the child has passed the appropriate age for serial casting.
Primary Indications for Surgery:
* Persistent pain related to altered biomechanics.
* Objectionable cosmetic appearance causing psychosocial distress.
* Significant difficulty in fitting standard footwear due to residual rigid forefoot adduction.
The choice of surgical procedure is highly dependent on the patient's age and the specific pathoanatomy of the deformity.
Age-Based Treatment Algorithm
- Infancy to 2 Years: Serial stretching and casting. Surgery is contraindicated.
- 2 to 4 Years: Tarsometatarsal capsulotomies (Heyman, Herndon, and Strong procedure). Note: This is increasingly rare due to high complication rates.
- 4 Years and Older: Multiple metatarsal osteotomies (Berman and Gartland procedure) OR Medial cuneiform opening wedge / lateral cuboid closing wedge osteotomies (McHale and Lenhart procedure).
Surgical Warning: The Heyman-Herndon-Strong procedure (mobilization of the tarsometatarsal and intermetatarsal joints via capsular release) was historically recommended for children aged 3 to 8 years. However, Stark, Johnson, and Winter reported a 41% overall failure rate and a 51% incidence of painful dorsal prominences. Complications include subluxation of the metatarsal bases and iatrogenic injury to the articular cartilage. Consequently, bony osteotomies are now vastly preferred for rigid deformities in children over 4 years of age.
Surgical Technique: Dome-Shaped Osteotomies of Metatarsal Bases (Berman and Gartland)
For children 4 years of age and older presenting with residual, rigid metatarsus adductus, multiple metatarsal osteotomies are the procedure of choice. Berman and Gartland described dome-shaped osteotomies at the bases of all five metatarsals. The dome shape provides inherent stability and allows for multiplanar correction without shortening the metatarsals.
If the foot is fully mature or if medial soft-tissue structures are severely contracted, a laterally based closing wedge osteotomy may be required. However, correcting alignment without shortening the lateral border can place excessive tension on the medial skin and the neurovascular bundle posterior to the medial malleolus.

Fig. 7: Clinical presentation of rigid metatarsus adductus in an 8-year-old child prior to surgical intervention.

Fig. 8: Preoperative radiograph of the same 8-year-old child, demonstrating fixed adduction at the tarsometatarsal joints.
Step-by-Step Procedure
- Positioning and Preparation: The patient is placed supine on the operating table. A well-padded thigh tourniquet is applied. Fluoroscopy must be available.
- Surgical Approach: Approach all five metatarsal bases dorsally. Make two longitudinal dorsal incisions:
- Medial Incision: Placed between the first and second metatarsals.
- Lateral Incision: Placed overlying the fourth metatarsal.
- Dissection: Carefully dissect through the subcutaneous tissues. Meticulously protect the extensor tendons and branches of the superficial peroneal nerve. Preserve the superficial dorsal venous network as much as possible to prevent postoperative edema.
- Exposure: Subperiosteally expose the proximal metaphysis of each of the five metatarsals.
- Osteotomy: Using a small power drill or a specialized crescentic oscillating saw blade, create a dome-shaped osteotomy in each metatarsal base.
- Crucial Detail: The apex of the dome must point proximally.
- Pitfall Avoidance: Strictly avoid the physis at the base of the first metatarsal, which is located proximally.
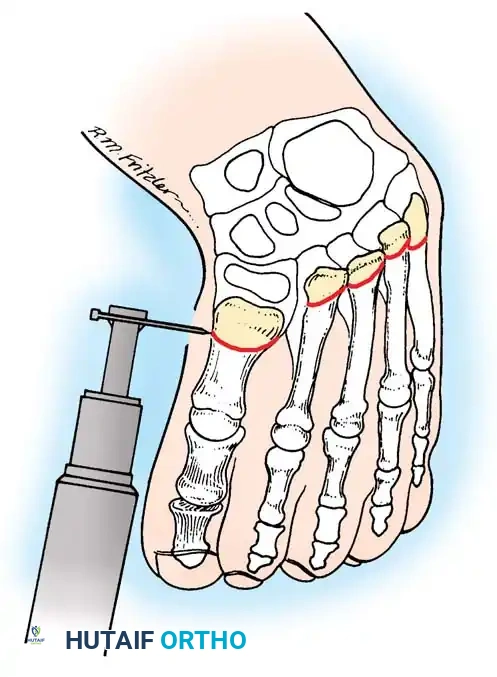
Fig. 9: Berman and Gartland technique. A dome-shaped osteotomy is completed at the base of each metatarsal using a power drill or crescentic saw, with the apex directed proximally.
- Correction and Wedge Resection: Manipulate the forefoot into abduction. If adequate correction cannot be obtained solely by rotating the dome osteotomies (due to severe lateral column shortening), resect small wedges of bone based laterally at the osteotomy sites as needed.
- Fixation: Align the metatarsals and transfix the foot in the corrected, plantigrade position. Insert small, smooth Steinmann pins (or heavy Kirschner wires) proximally through the shafts of the first and fifth metatarsals, crossing the osteotomy sites into the respective cuneiforms and cuboid.
- Ensure there is no dorsal or volar angulation, and prevent overriding of the osteotomy fragments.
- Radiographic Confirmation: Before closure, utilize fluoroscopy to check pin placement, osteotomy apposition, and overall forefoot alignment. The anteroposterior talus–first metatarsal angle should be corrected to 0 to 10 degrees.

Fig. 10: Intraoperative radiograph showing completed dome osteotomies with Steinmann pins inserted to hold the corrected position.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the incisions in layers.
Postoperative Protocol (Berman-Gartland)
- Immediate Post-Op: A well-padded, short leg cast is applied with the foot held in the corrected position. The limb is elevated to minimize swelling.
- 6 Weeks: The initial cast and the Steinmann pins are removed in the clinic. Radiographs are obtained to assess early callus formation.
- 6 to 12 Weeks: Weight-bearing is initiated in a short leg walking cast or a rigid controlled ankle motion (CAM) boot for an additional 3 to 6 weeks until radiographic union is complete.

Fig. 11: Postoperative clinical appearance demonstrating excellent correction of the forefoot alignment.

Fig. 12: Postoperative radiograph confirming healing of the metatarsal osteotomies and restoration of the normal talus-first metatarsal angle.
Surgical Technique: Cuneiform and Cuboid Osteotomies (McHale and Lenhart)
For complex midfoot deformities characterized by severe shortening of the medial column and a prominent lateral border (often described as a "bean-shaped" foot), McHale and Lenhart described a powerful midfoot correction. This involves an opening wedge osteotomy of the medial cuneiform combined with a closing wedge osteotomy of the cuboid. This technique corrects the deformity at the apex of the midfoot curve without violating the tarsometatarsal joints.
Step-by-Step Procedure
- Positioning: The anesthetized patient is placed supine. A thigh tourniquet is utilized.
- Lateral Approach (Cuboid): Make a small longitudinal incision directly over the cuboid.
- Cuboid Osteotomy: Perform a closing wedge osteotomy of the cuboid. Remove a 7- to 10-mm wedge of bone with its base oriented dorsolaterally. Preserve this bone wedge carefully, as it will be used as the graft for the medial side.
- Medial Approach (Cuneiform): Approach the medial cuneiform either by extending a medial incision or by making a dedicated 2-cm longitudinal incision medially over the medial cuneiform.
- Cuneiform Osteotomy: Perform a transverse osteotomy through the mid-substance of the medial cuneiform.
- Surgical Pearl: Leave the insertion of the anterior tibial tendon attached to the distal fragment of the medial cuneiform to maintain dynamic control of the medial column.
- Graft Insertion: Insert a vertebral lamina spreader into the medial cuneiform osteotomy and gently distract it. Take the bone wedge previously harvested from the cuboid and insert it into the medial cuneiform defect. The base of the wedge should face straight medially.
- Assessment of Correction: Evaluate the clinical correction. If the lateral border of the foot remains prominent (indicating uncorrected midfoot supination or adduction), return to the lateral side and resect a larger wedge of bone from the cuboid.
- Fixation: Fix the foot in the corrected position using two smooth Kirschner wires:
- Lateral Pin: Start in the calcaneus, pass through the cuboid osteotomy, and exit through the base of the fifth metatarsal.
- Medial Pin: Insert through the first web space, pass down the shaft of the first metatarsal, through the grafted medial cuneiform, through the navicular, and anchor into the talus.
- Radiographic Confirmation: Confirm pin placement and bony alignment via fluoroscopy.
- Adjunctive Procedures: After correcting the midfoot, the lateral three toes may occasionally remain in passively uncorrectable flexion due to relative lengthening of the flexor tendons. If this occurs, perform simple percutaneous flexor tenotomies.
- Closure: Close the wounds in layers. Apply a short leg cast with thick cotton padding to accommodate anticipated postoperative swelling.
Postoperative Protocol (McHale-Lenhart)
- 2 Weeks: The patient is seen in the clinic. The initial surgical cast is removed, wounds are inspected, and sutures are removed. A more form-fitting, non-weight-bearing short leg cast is applied.
- 6 Weeks: The Kirschner wires are removed in the clinic. A weight-bearing short leg cast is applied.
- 8 to 12 Weeks: The weight-bearing cast is maintained until definitive bony union at both the cuneiform and cuboid osteotomy sites is evident on radiographs. Once union is confirmed, the patient is transitioned to supportive footwear.
Conclusion
The management of congenital metatarsus adductus requires a nuanced understanding of foot biomechanics and a careful assessment of deformity rigidity. While conservative serial casting remains the cornerstone of treatment for infants, rigid deformities in older children demand precise surgical intervention. By mastering both the Berman-Gartland metatarsal osteotomies and the McHale-Lenhart midfoot osteotomies, the orthopedic surgeon can effectively restore plantigrade alignment, alleviate pain, and prevent the long-term sequelae of lateral column overload.
📚 Medical References
- Anderson D, Schoenecker P: Combined lateral column shortening and medial column lengthening in the treatment of severe forefoot adductus. Paper presented at the First International Congress on Clubfeet, Milwaukee, Sept 1990.
- Asirvatham R, Stevens PM: Idiopathic forefoot-adduction deformity: medial capsulotomy and abductor hallucis lengthening for resistant and severe deformities, J Pediatr Orthop 17:496, 1997.
- Berman A, Gartland JJ:
