INTRODUCTION TO ACETABULAR FRACTURES
The management of acetabular fractures represents one of the most formidable challenges in orthopedic trauma surgery. Historically managed with prolonged skeletal traction, the modern era of acetabular fracture care was revolutionized by Emile Letournel and Robert Judet. Their meticulous anatomical studies and development of a comprehensive classification system paved the way for open reduction and internal fixation (ORIF) as the standard of care for displaced fractures.
With longer-term follow-up of operatively treated acetabular fractures, a critical biomechanical truth has emerged: even minor residual incongruencies within the weight-bearing dome of the acetabulum exponentially increase the risk of post-traumatic osteoarthritis. Consequently, the indications for surgical intervention have become more inclusive, prioritizing anatomical reduction, rigid fixation, and early mobilization.
THE LETOURNEL AND JUDET CLASSIFICATION
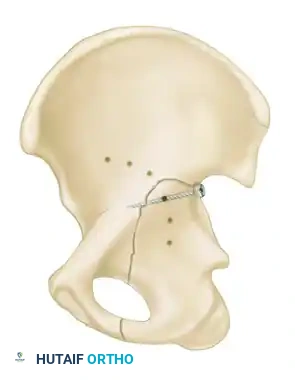
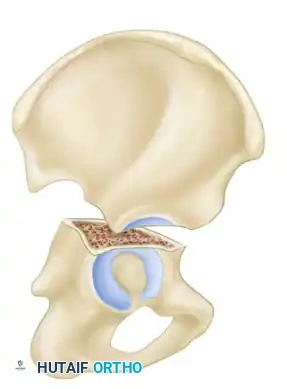
The Letournel and Judet classification system remains the universally accepted framework for categorizing acetabular fractures. It is predicated on the concept of the acetabulum being supported by an inverted "Y" consisting of an anterior column and a posterior column. The system divides fractures into two broad categories: Simple Fracture Types and Associated Fracture Types.
Simple Fracture Types
Simple fractures involve a single primary fracture line or isolate a single anatomical region of the acetabulum. There are five simple patterns:
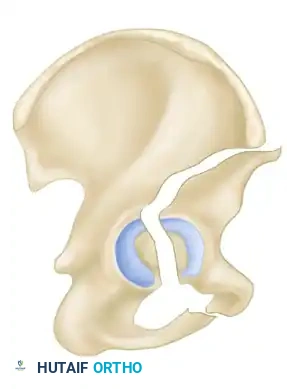
- Posterior Wall Fractures: The most common acetabular fracture, frequently associated with posterior hip dislocations. The fracture involves the posterior articular surface, compromising hip stability.
- Posterior Column Fractures: The fracture line begins at the greater sciatic notch, traverses the articular surface, and exits through the obturator ring (ischio-pubic ramus), detaching the entire posterior column.
- Anterior Wall Fractures: Rare injuries involving the anterior articular surface, typically exiting through the anterior border of the ilium.
- Anterior Column Fractures: The fracture line originates anywhere along the anterior border of the ilium (from the iliac crest to the anterior inferior iliac spine) and exits through the superior pubic ramus.
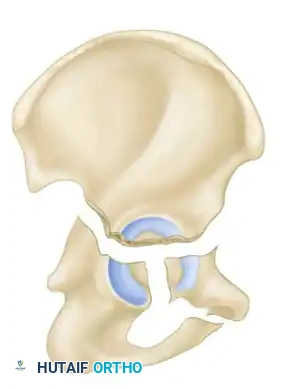
- Transverse Fractures: A single fracture line crosses both the anterior and posterior columns horizontally, dividing the innominate bone into a superior (iliac) segment and an inferior (ischiopubic) segment.
Associated Fracture Types
Associated fractures are complex patterns combining two or more simple fracture types. There are five associated patterns:
- Posterior Column and Posterior Wall: A posterior column fracture combined with a distinct posterior wall fragment.
- Transverse and Posterior Wall: A transverse fracture with an associated posterior wall fracture. This is a highly unstable pattern often requiring a posterior surgical approach.
- T-Shaped Fractures: A transverse fracture with an additional vertical fracture line that splits the inferior ischiopubic segment, exiting through the obturator ring.
- Anterior Column and Posterior Hemitransverse: An anterior column fracture combined with a transverse fracture through the posterior column.
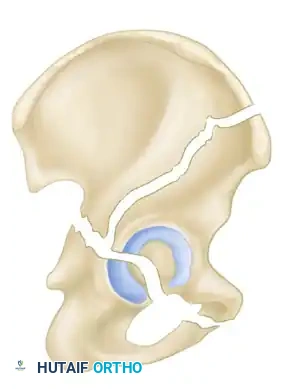
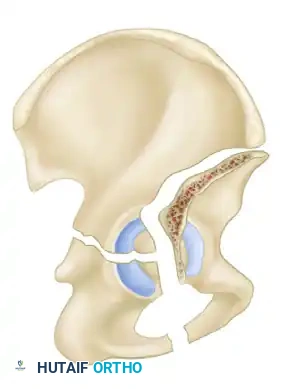
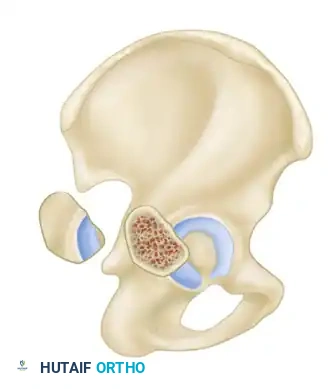
- Both-Column Fractures: The most complex pattern. All articular segments are detached from the intact posterior ilium (which remains attached to the sacrum).
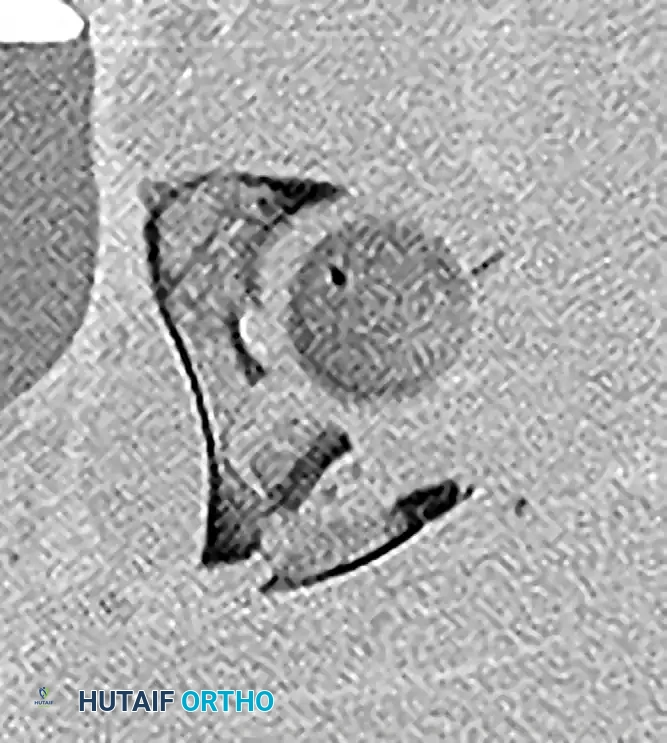
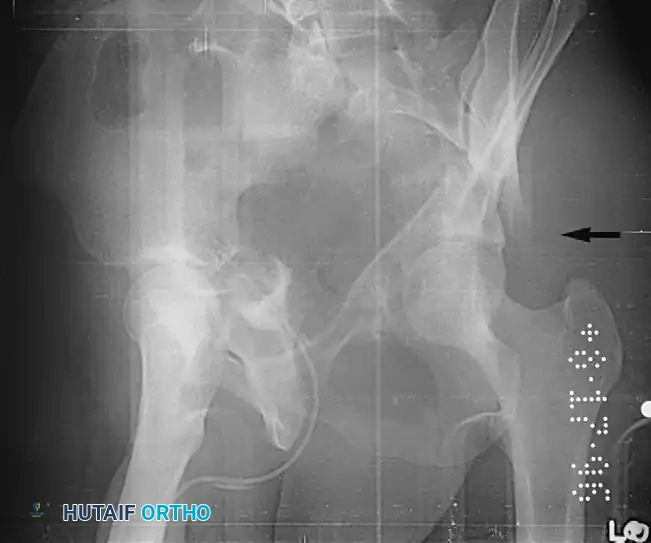
Clinical Pearl: The Spur Sign
In a both-column fracture, the intact portion of the ilium (attached to the sacroiliac joint) projects laterally relative to the medially displaced, fractured acetabular columns. On an obturator oblique radiograph, this intact bone appears as a sharp spike, known as the "Spur Sign." Its presence is pathognomonic for a both-column fracture.
INDICATIONS FOR NONOPERATIVE TREATMENT
While ORIF is the gold standard for displaced fractures, nonoperative management is highly successful when strict radiographic and clinical criteria are met.
Nondisplaced and Minimally Displaced Fractures
Fractures traversing the weight-bearing dome that exhibit less than 2 mm of displacement can be managed nonoperatively. Treatment consists of strict non-weight-bearing or touch-down weight-bearing (TDWB) precautions for 6 to 12 weeks.
Radiographs must be obtained immediately after the patient is mobilized from bed to chair, and serially thereafter, to ensure no secondary displacement occurs. In equivocal cases, a repeat CT scan is mandated to verify the maintenance of reduction.
Fractures Outside the Weight-Bearing Dome
If a fracture is significantly displaced but the involved articular region is prognostically unimportant, nonoperative treatment may be considered. This is determined using Roof Arc Measurements on the three standard Judet views (AP, Iliac Oblique, Obturator Oblique).
Historically, Matta established that a roof arc measurement of >45 degrees on all three views indicated the fracture exited outside the critical weight-bearing dome. However, Vrahas et al. refined these criteria based on cadaveric biomechanical studies, proposing the following acceptable minimum roof arcs:
* Anterior Roof Arc: 25 degrees
* Medial Roof Arc: 45 degrees
* Posterior Roof Arc: 70 degrees
As a general surgical heuristic, displaced fractures exiting the posterior column above the upper border of the ischial spine, or exiting the anterior column high through the iliac wing, typically require ORIF.
Dynamic Fluoroscopic Stress Testing
Posterior wall fractures demand special consideration. Large fragments (>50% of the posterior wall) invariably lead to posterior hip instability and mandate fixation. However, smaller fragments (<50%) exist in a gray area.
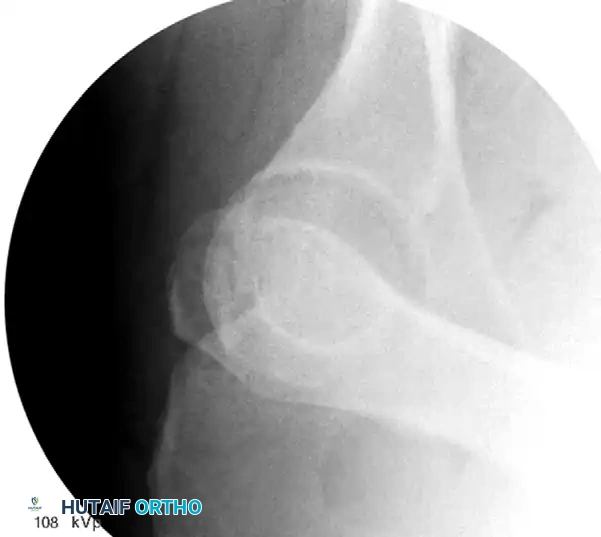
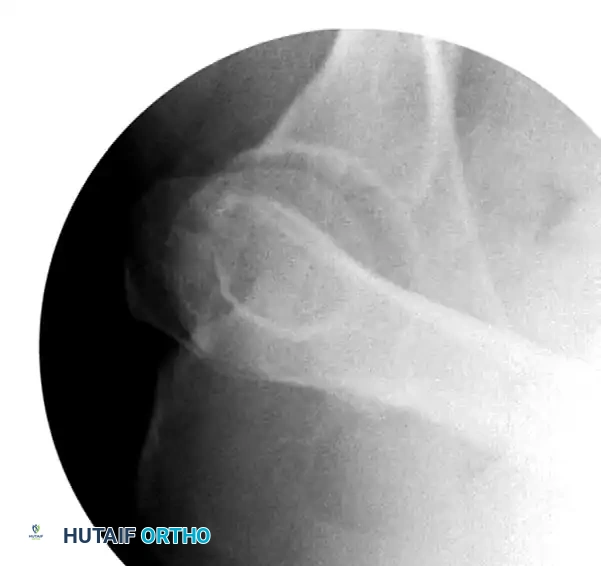
Tornetta popularized dynamic fluoroscopic stress testing for these indeterminate fractures. Under deep sedation or general anesthesia, the patient is positioned supine. The hip is flexed to 90 degrees, and a posteriorly directed axial force is applied while visualizing the joint under fluoroscopy in the obturator oblique view.
If the femoral head subluxates posteriorly, the hip is dynamically unstable, and ORIF is required. If concentric reduction is maintained under stress, the patient can be treated nonoperatively with progressive mobilization.
Secondary Congruence in Both-Column Fractures
A unique phenomenon observed exclusively in both-column fractures is "secondary congruence." Because all articular fragments are detached from the axial skeleton, they can occasionally settle concentrically around the medially displaced femoral head.
If the articular cartilage space is preserved and the femoral head remains concentrically enveloped by the fragments (despite medialization of the entire joint complex), nonoperative treatment via skeletal traction can yield surprisingly excellent long-term functional results.

Soft Tissue Contraindications: The Morel-Lavallée Lesion
An open wound or systemic infection is an absolute contraindication to immediate ORIF. Furthermore, surgeons must be highly vigilant for the Morel-Lavallée lesion—a closed, degloving injury caused by severe shear forces that separate the subcutaneous fat from the underlying fascia lata.
Operating directly through a Morel-Lavallée lesion carries an unacceptably high postoperative infection rate (up to 12%). If this lesion is present, surgery must be delayed until the soft tissues recover, or an alternative surgical approach (e.g., anterior rather than posterior) must be utilized. Percutaneous screw fixation may also be considered as a damage-control or definitive alternative in these scenarios.
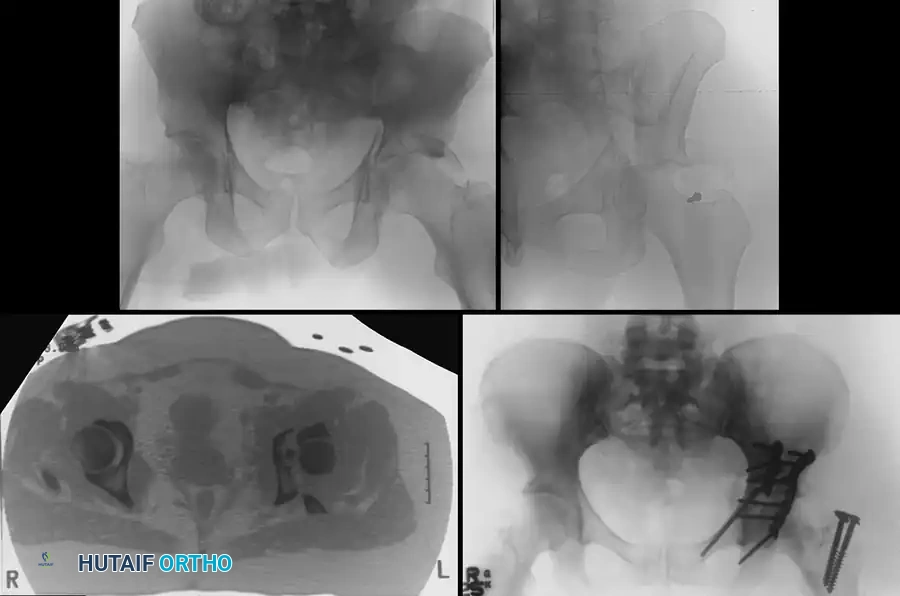
INDICATIONS FOR OPERATIVE TREATMENT (ORIF)
The primary goal of operative intervention is the anatomical restoration of the articular surface to prevent post-traumatic arthrosis, alongside rigid internal fixation to allow early mobilization.
Fracture Characteristics Mandating Surgery
- Displacement: Any fracture with ≥2 mm of displacement within the weight-bearing dome (defined by roof arc measurements <45 degrees).
- Instability: Posterior wall fractures involving >50% of the articular surface, or those demonstrating instability on dynamic stress testing.
- Subluxation: Any resting subluxation of the femoral head noted on static AP or Judet radiographs.
Surgical Warning:
Never accept a fracture that "appears to reduce in traction" if it involves the weight-bearing dome. These fractures have a high propensity for secondary displacement once traction is removed, leading to catastrophic articular wear.
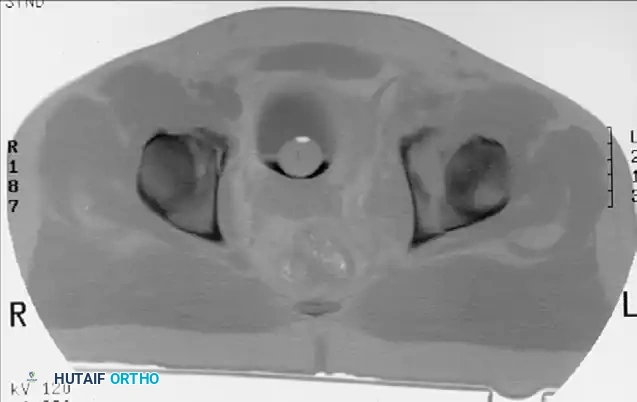
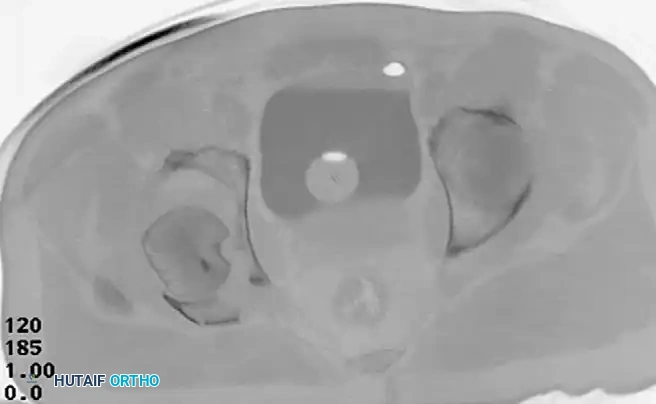
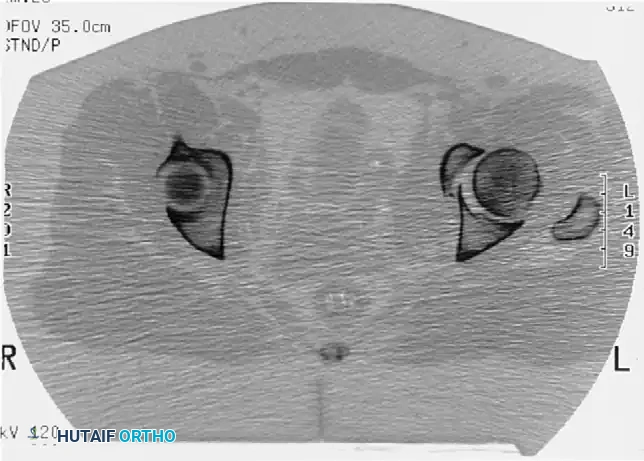
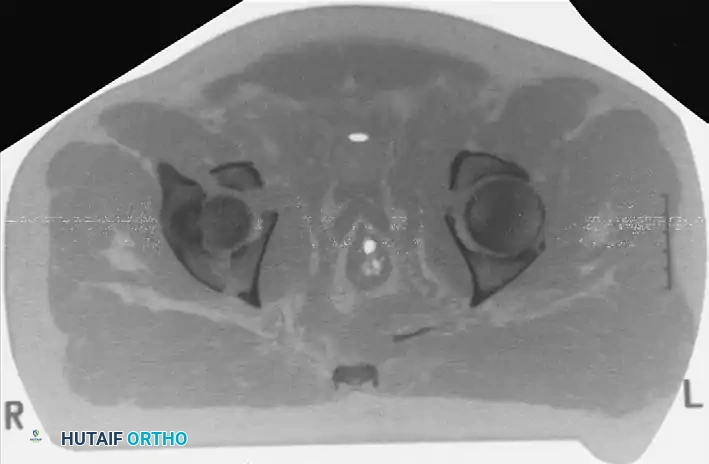
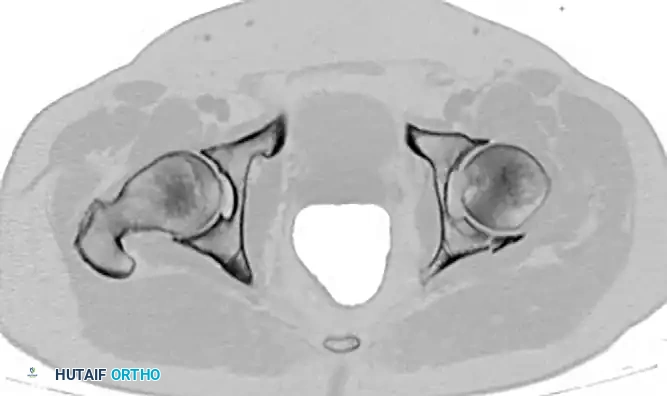
Incarcerated Intra-Articular Fragments
Following the closed reduction of a hip dislocation, a post-reduction CT scan is mandatory. While small avulsions of the ligamentum teres sequestered deep in the cotyloid fossa may be observed, any osteochondral fragment lodged between the articulating surfaces of the femoral head and the acetabular dome necessitates urgent surgical excision and joint irrigation.
Considerations in the Elderly Patient
Historically, ORIF was performed in the elderly to preserve bone stock for future reconstructive surgery. Today, this paradigm has shifted. In elderly patients with severe comminution, osteopenia, or pre-existing osteoarthritis, achieving anatomical reduction is often impossible.
In these cases, two modern strategies are employed:
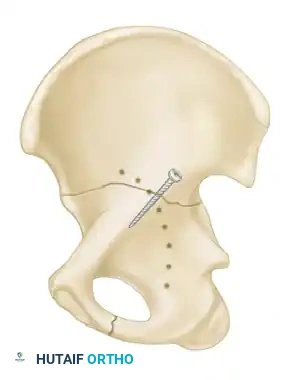
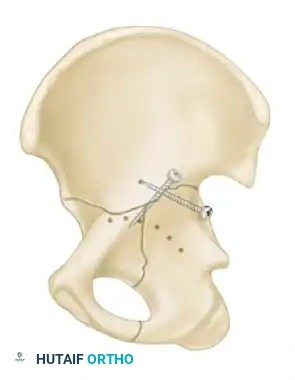
1. Percutaneous Fixation: Limited column fixation using percutaneous fluoroscopic techniques to prevent gross displacement, allowing the fracture to heal in a stable position prior to a delayed Total Hip Arthroplasty (THA).
2. Acute Total Hip Arthroplasty: Primary THA combined with limited internal fixation (to stabilize the acetabular shell) is increasingly advocated for elderly patients with poor prognostic fracture patterns, allowing immediate full weight-bearing.

SURGICAL TIMING AND OPTIMIZATION
Acetabular fractures are rarely extreme orthopedic emergencies, with a few critical exceptions. Urgent surgical intervention is required in the presence of:
* Irreducible hip dislocations.
* Progressive neurologic deficits (e.g., evolving sciatic nerve palsy).
* Vascular compromise.
* Open pelvic/acetabular fractures.
In the absence of these emergencies, surgery should be delayed for 3 to 5 days. This window allows for the optimization of the patient's hemodynamic status, resolution of intrapelvic bleeding, and detailed preoperative planning (including 3D CT reconstructions and the assembly of an experienced surgical team). During this delay, the hip should be maintained in skeletal traction to protect the articular cartilage from pressure necrosis.
SURGICAL APPROACHES AND POSITIONING
Selecting the correct surgical approach is the most critical decision in acetabular fracture surgery. The approach is dictated by the fracture pattern, the column requiring the most manipulation, and the presence of soft tissue injuries.
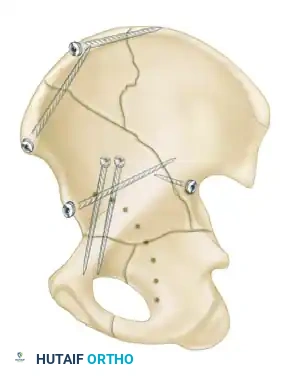
The Kocher-Langenbeck Approach
- Indications: Posterior wall, posterior column, and certain transverse fractures.
- Positioning: Prone or lateral decubitus. Prone positioning allows for easier reduction of the posterior column using gravity, while lateral positioning is preferred if the patient has severe pulmonary contusions or requires simultaneous access to the anterior column.
- Interval: The gluteus maximus is split in line with its fibers. The short external rotators (piriformis, obturator internus, gemelli) are tagged and released at their femoral insertions to expose the retroacetabular surface and the greater sciatic notch.
- Nerve Protection: The sciatic nerve must be identified and meticulously protected throughout the procedure. Keeping the hip extended and the knee flexed reduces tension on the nerve.
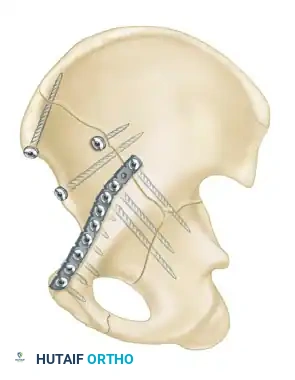
The Ilioinguinal Approach
- Indications: Anterior column, anterior wall, and anterior-dominant both-column fractures.
- Positioning: Supine on a radiolucent table.
- Technique: This is an entirely extrapelvic approach that utilizes three distinct surgical windows to access the anterior column from the SI joint to the pubic symphysis.
- Lateral Window: Between the iliac crest and the iliopsoas muscle.
- Middle Window: Between the iliopsoas/femoral nerve and the external iliac vessels.
- Medial Window: Medial to the external iliac vessels and lateral to the rectus abdominis.
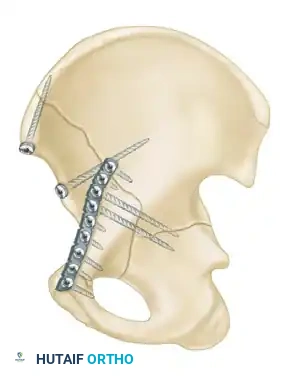
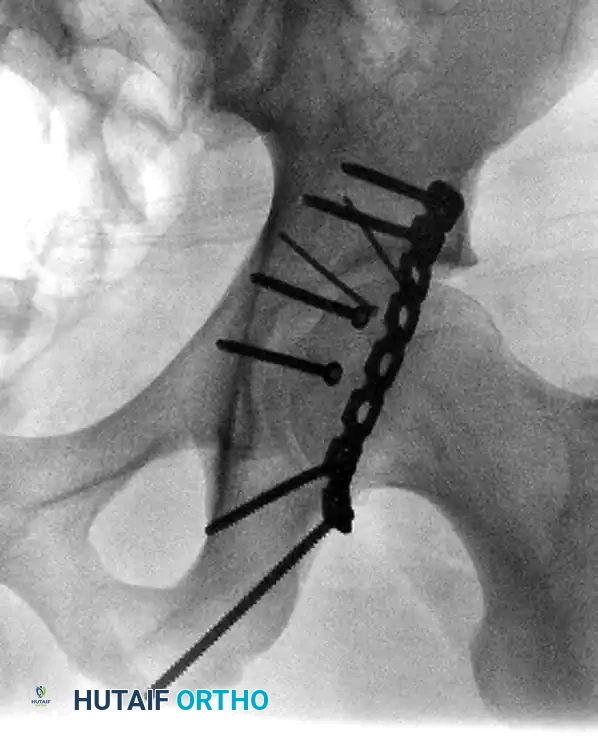
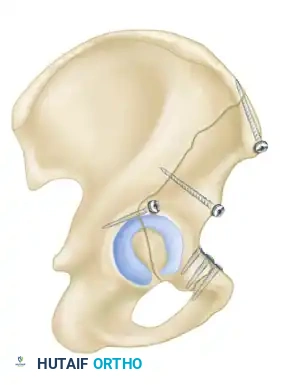
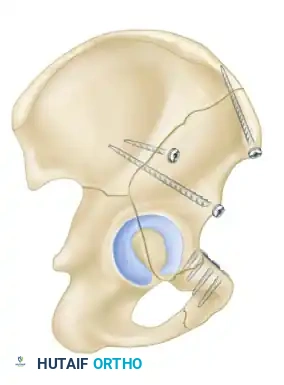
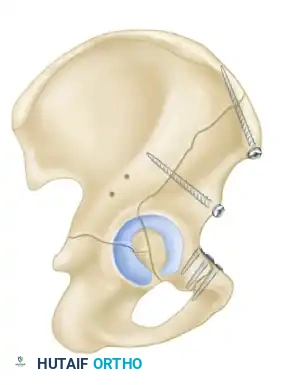
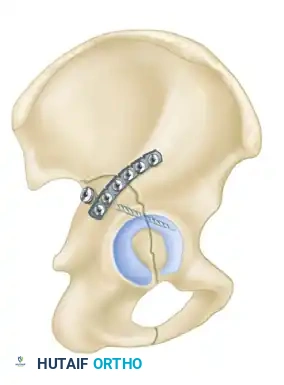
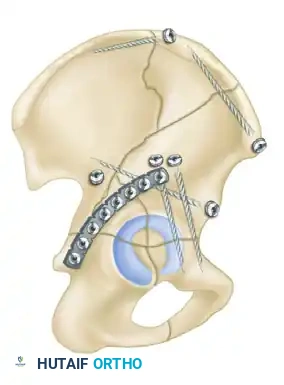
- Biomechanics: This approach allows for the placement of long reconstruction plates along the pelvic brim (iliopectineal line) to buttress the anterior column.
The Modified Stoppa Approach
- Indications: Medial displacement of the quadrilateral surface, anterior column fractures, and certain both-column fractures.
- Positioning: Supine.
- Technique: A transverse Pfannenstiel incision is made, and the surgeon works intrapelvically, deep to the rectus abdominis and along the pelvic brim. This approach provides direct visualization of the quadrilateral plate and allows for the application of medial buttress plates to prevent medial subluxation of the femoral head. It is frequently combined with a lateral window (from the ilioinguinal approach) for complete anterior column access.

POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of acetabular fracture surgery relies heavily on strict adherence to postoperative protocols.
- Weight-Bearing Status: Patients are typically restricted to touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) on the operative extremity for 8 to 12 weeks, depending on bone quality and fracture comminution. Early passive and active-assisted range of motion (ROM) of the hip is encouraged to nourish the articular cartilage and prevent capsular contracture.
- Deep Vein Thrombosis (DVT) Prophylaxis: Pelvic trauma carries a massive risk for venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) should be initiated postoperatively and continued for a minimum of 4 to 6 weeks.
- Heterotopic Ossification (HO) Prophylaxis: HO is a frequent complication, particularly following the Kocher-Langenbeck approach due to the stripping of the gluteal musculature. Prophylaxis is mandatory and typically consists of either a single dose of localized radiation therapy (700-800 cGy) within 72 hours of surgery, or a 6-week course of oral Indomethacin.
By adhering to strict biomechanical principles, utilizing precise surgical approaches, and respecting the delicate soft tissue envelope, orthopedic surgeons can restore articular congruity and maximize long-term functional outcomes in patients with complex acetabular fractures.
Associated Surgical & Radiographic Imaging