Carpal Tunnel Syndrome: Comprehensive Treatment and Surgical Release

Key Takeaway
Carpal tunnel syndrome (CTS) management ranges from conservative splinting and corticosteroid injections for mild cases to surgical decompression for advanced neuropathy. Prognostic factors such as age, symptom duration, and constant paresthesia dictate nonoperative success. When conservative measures fail or thenar atrophy is present, open or limited-incision carpal tunnel release is indicated to divide the transverse carpal ligament, restoring median nerve hemodynamics and preventing irreversible motor loss.
Comprehensive Introduction and Patho-Epidemiology
Carpal Tunnel Syndrome (CTS) represents the most ubiquitous compressive neuropathy of the upper extremity, accounting for approximately 90% of all entrapment neuropathies encountered in clinical orthopedic practice. The condition is characterized by a symptomatic compression of the median nerve as it traverses the rigid fibro-osseous confines of the carpal canal. Epidemiological data indicates that CTS affects approximately 3% to 6% of the general adult population, with a pronounced demographic predilection for females, who are affected at a rate nearly three times higher than their male counterparts. The peak incidence typically manifests in a bimodal distribution, with the highest prevalence occurring in the fifth and sixth decades of life, often correlating with perimenopausal hormonal shifts, and a secondary peak in the geriatric population.
The pathophysiological cascade of Carpal Tunnel Syndrome is fundamentally driven by a combination of mechanical compression and localized microvascular ischemia. The carpal tunnel is a tightly constrained anatomical compartment; normal resting interstitial hydrostatic pressure within the canal ranges from 2 to 10 mm Hg. In patients with CTS, baseline resting pressures are chronically elevated, often exceeding 30 mm Hg. This elevation in pressure surpasses the capillary perfusion pressure of the median nerve's vasa nervorum, leading to venular congestion and a subsequent breakdown of the blood-nerve barrier. The resultant transudation of fluid causes endoneurial edema, which further exacerbates the intracompartmental pressure, creating a deleterious positive feedback loop of ischemia and mechanical deformation.
As the ischemic insult persists, the median nerve undergoes a progressive and predictable sequence of histopathological changes. Initially, the condition is characterized by a reversible, dynamic ischemia that manifests clinically as intermittent paresthesias, particularly nocturnal awakening due to the natural tendency to sleep with the wrist in a flexed position. Prolonged compression, however, induces irreversible changes, including segmental demyelination (neurapraxia) and, ultimately, axonal degeneration (axonotmesis) with Wallerian degeneration distal to the site of compression. This advanced stage is clinically heralded by constant numbness, profound sensory loss, and irreversible thenar muscle atrophy. Furthermore, the surrounding flexor tenosynovium often undergoes a non-inflammatory fibrotic hypertrophy, which is the most common histological finding in idiopathic CTS, rather than an acute inflammatory tenosynovitis.
Understanding the occupational and systemic risk factors is paramount for the orthopedic surgeon. While repetitive occupational microtrauma, vibratory tool use, and sustained non-neutral wrist postures are frequently implicated in the exacerbation of symptoms, the etiology of idiopathic CTS is largely considered multifactorial, with genetic predisposition and anthropometric wrist dimensions playing significant roles. Systemic conditions that alter fluid balance or reduce the spatial capacity of the carpal canal—such as diabetes mellitus, hypothyroidism, rheumatoid arthritis, amyloidosis, and pregnancy—dramatically increase the relative risk of developing CTS. The diabetic nerve, in particular, is highly susceptible to compression due to the "double crush" phenomenon, wherein an underlying peripheral neuropathy lowers the threshold for symptomatic mechanical entrapment.
Detailed Surgical Anatomy and Biomechanics
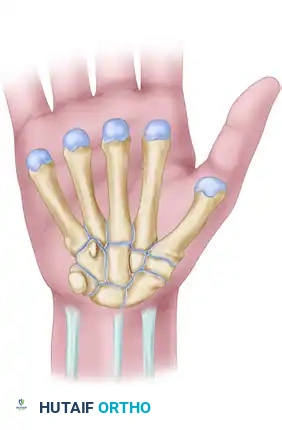
A profound, three-dimensional understanding of the flexor retinaculum and its surrounding neurovascular structures is the absolute prerequisite for safe surgical execution. The carpal tunnel is a rigid fibro-osseous conduit situated at the volar aspect of the wrist. Its dorsal, radial, and ulnar borders are formed by the concave arch of the carpal bones. Specifically, the radial border is defined by the scaphoid tubercle and the ridge of the trapezium, while the ulnar border is demarcated by the pisiform and the hook of the hamate. The volar roof of this tunnel is formed by the robust flexor retinaculum, a complex, tripartite structure that restrains the flexor tendons and protects the median nerve.
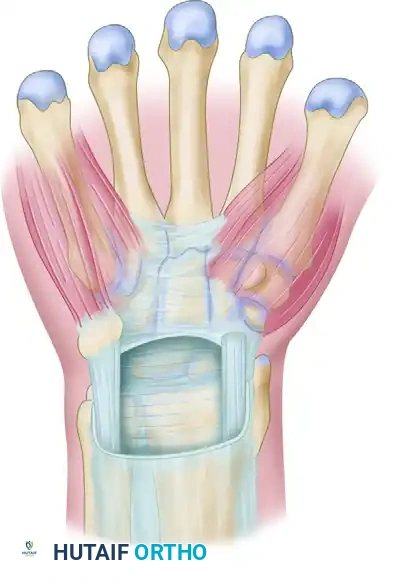
The flexor retinaculum is not a single homogeneous ligament but rather an amalgamation of three distinct anatomical and functional segments. The proximal portion consists of the deep investing fascia of the forearm, which courses deep to the flexor carpi ulnaris and flexor carpi radialis. The middle portion, the transverse carpal ligament (TCL) proper, is a dense, thick aponeurosis spanning between the thenar and hypothenar eminences. It is the primary mechanical restraint preventing bowstringing of the flexor tendons. The distal portion comprises an aponeurotic extension between the thenar and hypothenar musculature. The proximal limit of the retinaculum roughly aligns with the distal aspect of the pisiform, while the distal limit extends just beyond the hook of the hamate.

Within this unyielding anatomical space lie ten critical structures: the four tendons of the flexor digitorum superficialis (FDS), the four tendons of the flexor digitorum profundus (FDP), the flexor pollicis longus (FPL) tendon, and the median nerve. The median nerve typically lies superficial and slightly radial to the FDS tendons within the canal. The spatial arrangement of the FDS tendons is highly specific, with the tendons to the middle and ring fingers lying volar to those of the index and small fingers. The median nerve itself is highly vulnerable to compression against the unyielding volar surface of the transverse carpal ligament, particularly during dynamic wrist movements.
The branching pattern of the median nerve exhibits significant anatomical variance, which poses a substantial risk during surgical release. The recurrent motor branch, which innervates the critical thenar musculature (abductor pollicis brevis, opponens pollicis, and the superficial head of the flexor pollicis brevis), classically branches from the radial aspect of the median nerve just distal to the TCL (extraligamentous). However, according to the Lanz classification, variations include a subligamentous course (branching within the tunnel and running deep to the ligament before turning superficially) and a transligamentous course (piercing directly through the substance of the TCL). Additionally, the palmar cutaneous branch of the median nerve, which provides sensation to the base of the thenar eminence, typically branches 5 to 6 cm proximal to the radial styloid and courses between the palmaris longus and flexor carpi radialis before passing superficial to the TCL. Iatrogenic injury to this branch results in a debilitating neuroma.
Exhaustive Indications and Contraindications
The decision-making algorithm for the management of Carpal Tunnel Syndrome must be rigorously stratified based on the chronicity of symptoms, the severity of neurological impairment, and the patient's functional demands. Nonoperative management is universally recognized as the first-line intervention for mild to moderate idiopathic CTS. This includes nocturnal wrist splinting in a neutral position to minimize intracanalicular hydrostatic pressure, nonsteroidal anti-inflammatory drugs, and ergonomic modifications. Corticosteroid injections into the carpal tunnel serve both a therapeutic and diagnostic purpose; a robust, albeit temporary, response to an injection strongly correlates with a favorable outcome following eventual surgical decompression.
However, conservative management is destined to fail in specific clinical scenarios. The landmark study by Kaplan, Glickel, and Eaton identified strict prognostic factors predicting the failure of nonoperative treatment: age older than 50 years, symptom duration exceeding 10 months, constant paresthesia, coexisting stenosing flexor tenosynovitis, and a positive Phalen test result in less than 30 seconds. The presence of three or more of these factors renders conservative treatment practically futile, necessitating a direct transition to surgical planning. Surgical division of the deep transverse carpal ligament is definitively indicated for patients with persistent, progressive signs and symptoms that are refractory to these conservative measures, or those presenting with acute, space-occupying pathology within the carpal canal.
Absolute indications for immediate or expedited surgical release include the presence of objective motor weakness, visible thenar muscle atrophy, or profound sensory loss (e.g., an inability to distinguish two points at a separation of 5 mm). In these advanced cases, the primary objective of surgery shifts from pure symptom resolution to the cessation of progressive axonal death and the prevention of irreversible hand dysfunction. Acute Carpal Tunnel Syndrome, often precipitated by distal radius fractures, perilunate dislocations, or acute hemorrhage, represents a surgical emergency requiring immediate decompression to prevent catastrophic ischemic necrosis of the median nerve.
| Category | Specific Clinical Scenarios | Rationale / Notes |
|---|---|---|
| Absolute Indications | Thenar muscle atrophy | Indicates advanced motor axonotmesis; surgery halts progression. |
| Profound sensory loss (Abnormal 2PD) | Indicates advanced sensory axonal loss; high risk of permanent deficit. | |
| Acute CTS (e.g., post-trauma, fracture) | Compartment syndrome of the carpal canal; requires emergent release. | |
| Failure of >6 months of conservative tx | Chronic fibrotic changes require mechanical decompression. | |
| Relative Indications | Constant (non-intermittent) paresthesia | Suggests transition from dynamic ischemia to fixed nerve compression. |
| Space-occupying lesions (ganglion, tumor) | Mechanical obstruction that will not resolve with conservative care. | |
| Patient preference after transient injection relief | Injection proves diagnosis; surgery offers definitive, durable cure. | |
| Contraindications | Pure Cervical Radiculopathy (C6/C7) | Proximal compression mimicking CTS; wrist release provides no benefit. |
| Active local volar wrist infection | Risk of deep space seeding and flexor tendon sheath infection. | |
| Asymptomatic incidental finding on EMG | Surgery is indicated for symptomatic relief, not solely for electrical abnormalities. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical evaluation and objective diagnostic staging are critical to ensure optimal surgical outcomes and to manage patient expectations. The clinical diagnosis is established through a battery of provocative tests. Durkan's carpal compression test is currently recognized as the most sensitive and specific clinical maneuver, involving direct hydrostatic compression over the carpal tunnel to elicit paresthesia within 30 seconds. Phalen's wrist flexion test and Tinel's sign provide supplementary diagnostic confirmation. Objective sensory evaluation must include Semmes-Weinstein monofilament testing to assess the threshold of slowly adapting fibers, which is highly sensitive for early nerve impairment, and static two-point discrimination to evaluate innervation density and axonal loss in advanced disease.
Electrodiagnostic studies (EMG/NCS) remain the gold standard for confirming the diagnosis, staging the severity of the neuropathy, and ruling out proximal lesions such as cervical radiculopathy or thoracic outlet syndrome. Sensory nerve conduction studies are typically the first to show abnormalities, with a latency greater than 3.5 milliseconds across the wrist or a conduction velocity asymmetry of greater than 0.5 m/s compared to the contralateral limb considered diagnostic. Motor conduction latency exceeding 4.5 milliseconds indicates more advanced disease. Electromyography (EMG) is reserved for identifying active denervation in the thenar muscles, characterized by fibrillation potentials, positive sharp waves, or increased insertional activity, which strongly correlates with a poorer prognosis for complete motor recovery. High-resolution ultrasonography has also emerged as a valuable preoperative tool; a median nerve cross-sectional area (CSA) greater than 10 to 12 mm² at the level of the pisiform is highly indicative of CTS.
Preoperative templating and incision planning are heavily reliant on superficial anatomical landmarks. The standard open approach utilizes Kaplan's cardinal line—a line drawn from the apex of the interdigital fold between the thumb and index finger toward the ulnar side of the hand, parallel to the proximal palmar crease. The longitudinal incision is planned along the axis of the radial border of the ring finger, intersecting Kaplan's line. This specific vector is chosen to safely parallel the median nerve while remaining distinctly ulnar to the palmar cutaneous branch, thereby minimizing the risk of iatrogenic neuroma formation.
Patient positioning and anesthetic choice have evolved significantly. The procedure is typically performed with the patient supine and the operative extremity extended on a radiolucent hand table. While regional blocks or general anesthesia with a proximal pneumatic tourniquet were historically standard, the advent of WALANT (Wide Awake Local Anesthesia No Tourniquet) has revolutionized carpal tunnel surgery. Using a meticulously injected solution of 1% lidocaine with 1:100,000 epinephrine buffered with sodium bicarbonate, surgeons can achieve profound local anesthesia and excellent hemostasis without the ischemic pain of a tourniquet. This allows for intraoperative active motion testing, ensuring complete release of the flexor retinaculum and confirming unimpeded flexor tendon gliding before closure.
Step-by-Step Surgical Approach and Fixation Technique
In the context of carpal tunnel surgery, the term "fixation technique" does not refer to osteosynthesis or the implantation of hardware, but rather to the definitive surgical "fixation" or resolution of the pathology through the meticulous, irreversible division of the transverse carpal ligament and the stabilization of the decompressed neural environment. Whether utilizing a standard open approach, a limited-incision technique, or an endoscopic method, the fundamental, non-negotiable objective remains identical: the complete, visually confirmed division of the flexor retinaculum from its proximal fascial origin to its distal aponeurotic insertion.
The surgical execution begins with the planned longitudinal incision in the palm, typically measuring 3 to 4 centimeters in the standard open approach, or 1.5 to 2 centimeters in limited approaches. The skin and dense subcutaneous palmar fat are incised. Careful blunt dissection is utilized to identify and longitudinally divide the palmar aponeurosis. At this stage, self-retaining retractors are placed to provide tension on the soft tissues. The superficial palmar arch, located distal to the transverse carpal ligament, must be anticipated and protected. The transverse fibers of the flexor retinaculum are then clearly identified. It is imperative to clear the superficial areolar tissue off the ligament to ensure precise visualization of the ligamentous fibers.
The actual ligamentous release is typically initiated proximally and extended distally. A small incision is made in the proximal portion of the transverse carpal ligament, and a blunt elevator or a specialized carpal tunnel director is passed deep to the ligament to protect the underlying median nerve. Using a scalpel or dissecting scissors, the ligament is carefully divided longitudinally. The surgeon must maintain a slightly ulnar bias during the cut—aiming toward the hook of the hamate—to maximize the distance from the recurrent motor branch of the median nerve, which typically lies radially. As the ligament is divided, the surgeon will observe the immediate herniation or "pouting" of the underlying epineural fat and the median nerve, visually confirming the release of compartmental pressure.
Following the complete division of the transverse carpal ligament, the distal antebrachial fascia must also be released proximally for at least 2 to 3 centimeters to prevent a secondary proximal compression site. The carpal canal is then thoroughly explored. The median nerve is inspected for areas of pseudoneuroma, hourglass constriction, or anomalous branching. The canal is swept with a blunt dissector to ensure no distal fascial bands remain intact. Evidence-based literature strictly contraindicates internal neurolysis or epineurotomy, as these procedures offer no clinical benefit and drastically increase the risk of iatrogenic intrafascicular scarring. Once hemostasis is meticulously achieved—often aided by the deflation of the tourniquet if one was used—the wound is irrigated. Only the skin is closed, typically with non-absorbable horizontal mattress sutures; the flexor retinaculum is intentionally left open to allow for the volumetric expansion of the carpal canal, which heals via secondary intention with an increased cross-sectional area.
Complications, Incidence Rates, and Salvage Management
While carpal tunnel release is one of the most frequently performed and highly successful procedures in orthopedic surgery, it is not devoid of complications. The most common postoperative morbidity is "pillar pain," characterized by a deep, aching tenderness in the thenar and hypothenar eminences adjacent to the surgical release. Pillar pain occurs in up to 25% of patients postoperatively. While the exact etiology remains debated—theories include alteration of carpal arch biomechanics, micromotion of the carpal bones, or neuromatous pain from small divided nerve branches—it is typically self-limiting, resolving spontaneously within 3 to 6 months with conservative management and targeted scar desensitization.
A far more concerning complication is the incomplete release of the transverse carpal ligament, which represents the most frequent cause of persistent postoperative symptoms requiring revision surgery. Incomplete release almost universally occurs at the extreme distal aspect of the ligament, where the aponeurotic fibers blend with the hypothenar and thenar musculature, or proximally at the level of the antebrachial fascia. Endoscopic techniques, particularly in the hands of inexperienced operators, carry a statistically higher risk of incomplete release compared to the standard open approach. Revision surgery for incomplete release requires a formal, extended open approach to carefully identify the native anatomy amidst postoperative scarring.
Iatrogenic nerve injury is the most devastating complication, albeit rare, with an incidence of less than 0.5%. Laceration of the median nerve proper, the recurrent motor branch, or the palmar cutaneous branch results in profound functional and sensory deficits. The palmar cutaneous branch is particularly vulnerable if the surgical incision deviates too radially from the ring finger axis. Injury to this branch results in a painful neuroma that severely limits grip and palm loading. Salvage management for neuromas often involves proximal resection and burying the nerve stump deep into the pronator quadratus muscle belly.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Strategy |
|---|---|---|---|
| Pillar Pain | 15% - 25% | Limited incision techniques; avoid aggressive retraction. | Reassurance, NSAIDs, localized massage, desensitization therapy. Resolves in 3-6 months. |
| Incomplete Release | 1% - 2% | Direct visual confirmation of distal and proximal extents; sweeping the canal. | Formal open revision surgery with neurolysis and complete ligamentous division. |
| Palmar Cutaneous Neuroma | < 1% | Strict adherence to Kaplan's line; avoid radial deviation of the incision. | Excision of neuroma and proximal transposition of the nerve stump into muscle. |
| Recurrent Motor Branch Injury | < 0.2% | Ulnar-biased incision of the TCL; extreme caution with distal release. | Immediate microsurgical primary repair or nerve grafting; delayed opponensplasty. |
| Complex Regional Pain Syndrome | 2% - 5% | Meticulous hemostasis; early postoperative active mobilization. | Aggressive hand therapy, gabapentinoids, stellate ganglion blocks, Vitamin C prophylaxis. |
| Recurrent CTS (True Recurrence) | 1% - 3% | Complete primary release; early tendon gliding to prevent scarring. | Revision neurolysis with hypothenar fat pad flap or pronator quadratus flap to wrap the nerve. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following carpal tunnel release is designed to balance the protection of the healing surgical wound with the imperative need for early mobilization to prevent flexor tendon adhesions and median nerve tethering. The protocol is generally divided into three distinct phases, tailored to the patient's tissue healing response and functional demands. Phase 1, the acute postoperative phase (0 to 14 days), begins immediately following surgery. A bulky, non-compressive soft dressing is applied to restrict excessive wrist motion while intentionally leaving the digits completely free. Rigid wrist immobilization via splinting is broadly discouraged in modern protocols, as it has been shown to increase the risk of stiffness and offers no advantage in symptom resolution or wound healing.
During Phase 1, early active digital mobilization is not merely encouraged; it is strictly required. Patients are instructed to perform composite finger flexion and extension, as well as specific intrinsic and extrinsic tendon gliding exercises, multiple times a day. These exercises facilitate the differential gliding of the FDS and FDP tendons, preventing them from adhering to the healing transverse carpal ligament and the median nerve. Median nerve gliding exercises are also initiated to ensure the nerve maintains its longitudinal excursion within the expanded carpal canal, preventing the formation of restrictive perineural fibrosis. Elevation of the extremity and active shoulder and elbow range of motion are emphasized to mitigate distal edema.
Phase 2, the intermediate phase (2 to 6 weeks), commences following suture removal at approximately 10 to 14 days. The primary focus shifts to scar management and progressive restoration of wrist biomechanics. Aggressive scar massage using emollient creams is initiated to soften the dermal healing and desensitize the palmar incision, which is crucial for mitigating pillar pain. Silicone gel sheeting may be utilized for hypertrophic scars. Progressive active and active-assisted wrist range of motion exercises are introduced. Patients are allowed to use the hand for light, non-resistive activities of daily living, but forceful gripping and heavy lifting remain restricted to prevent wound dehiscence and excessive inflammatory responses.
Phase 3, the strengthening and return-to-work phase (6 to 12 weeks), focuses on functional restoration. Progressive grip and pinch strengthening are initiated using putty and hand dynamometers. Work-conditioning programs may be necessary for manual laborers or those returning to high-impact occupations. It is critical to educate the patient regarding the expected timeline of recovery: while nocturnal paresthesias and radicular pain typically resolve within days of the procedure, the recovery of advanced sensory deficits (abnormal two-point discrimination) and the reversal of thenar atrophy can take 6 to 12 months, and in severe, chronic cases, may never fully normalize due to permanent axonal loss.
Summary of Landmark Literature and Clinical Guidelines
The surgical and nonoperative management of Carpal Tunnel Syndrome is supported by an extensive, robust body of orthopedic literature and formalized clinical practice guidelines. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guideline on the Management of Carpal Tunnel Syndrome provides evidence-based recommendations that heavily influence modern practice. The guidelines strongly support the use of local corticosteroid injections and nocturnal splinting for mild to moderate disease, while providing strong evidence that surgical release is the definitive treatment for patients failing conservative management or presenting with severe clinical or electrodiagnostic deficits.
The foundational principles of patient selection were definitively established by Kaplan, Glickel, and Eaton in their seminal 1990 study published in the Journal of Bone and Joint Surgery. By meticulously analyzing 331 patients, they quantified the prognostic factors that predict the failure of nonoperative treatment. Their identification of age, symptom duration, constant paresthesia, trigger digits, and rapid Phalen's positivity as critical failure markers remains the benchmark for triaging patients toward early surgical intervention, preventing the irreversible neurological damage associated with prolonged, futile conservative care.
The debate between open and endoscopic carpal tunnel release has generated voluminous comparative literature. Landmark randomized controlled trials by Agee et al. and Trumble et al. have demonstrated that while endoscopic release (whether single-portal or two-portal techniques) offers statistically significant advantages in early postoperative grip strength and a faster return to work (typically by 1 to 2 weeks) due to the preservation of the superficial palmar aponeurosis and subcutaneous tissues, the long-term outcomes at 6 and 12 months are virtually indistinguishable from standard open release. Both techniques yield equivalent, excellent rates of symptom resolution and patient satisfaction, provided the transverse carpal ligament is completely divided.
Furthermore, literature regarding adjunctive procedures during carpal tunnel release has definitively shaped modern surgical technique. Studies evaluating the efficacy of epineurotomy, internal neurolysis, and flexor tenosynovectomy have consistently demonstrated no significant clinical benefit over simple ligamentous release in idiopathic CTS. In fact, internal neurolysis has been shown to increase the risk of intraneural scarring and diminish functional outcomes. Consequently, current academic consensus strictly advises against these adjunctive maneuvers, advocating for
