ANATOMY AND PATHOPHYSIOLOGY OF COMPARTMENT SYNDROME
Acute compartment syndrome (ACS) represents a catastrophic orthopedic emergency characterized by increased interstitial pressure within a closed, non-yielding osteofascial envelope. This elevated pressure compromises the microcirculation of the tissues within that space, initiating a devastating ischemic cascade.
The pathophysiology of ACS is governed by the arteriovenous (AV) gradient theory. As intracompartmental pressure rises—whether from internal volume expansion (e.g., hemorrhage, edema, reperfusion injury) or external restriction (e.g., tight casts, circumferential burns)—venous outflow is obstructed. This venous hypertension further engorges the capillary beds, leading to fluid transudation into the interstitial space, thereby creating a vicious cycle of escalating pressure. Once the interstitial pressure surpasses the capillary perfusion pressure (typically when the gradient between diastolic blood pressure and compartment pressure falls below 30 mm Hg), capillary collapse occurs.
Clinical Pearl: Muscle and nerve ischemia begins well before arterial pulses are lost. The presence of a palpable distal pulse or normal capillary refill does not exclude the diagnosis of acute compartment syndrome. Pulselessness is a late, pre-terminal sign indicating that intracompartmental pressure has exceeded systolic blood pressure.
Irreversible myonecrosis and nerve damage can occur within 4 to 8 hours of sustained ischemia. Therefore, rapid clinical recognition and emergent surgical decompression via fasciotomy are paramount to preserving limb viability and function.
CLINICAL EVALUATION
The diagnosis of acute compartment syndrome is primarily clinical, demanding a high index of suspicion, particularly in high-risk scenarios such as tibial shaft fractures, crush injuries, vascular injuries, and prolonged limb compression.
The Classic Signs
The clinical presentation is classically described by the "6 Ps," though their reliability varies significantly:
* Pain out of proportion: The earliest and most sensitive clinical indicator. The pain is typically described as deep, unremitting, and poorly localized, failing to respond to standard opioid analgesia.
* Pain with passive stretch: Exquisite pain elicited by passive stretching of the muscles traversing the involved compartment. This is the most reliable physical examination finding.
* Paresthesia: Sensory deficits in the distribution of the nerves traversing the compartment. Hypesthesia should be meticulously evaluated using pinprick, light touch, and two-point discrimination.
* Palpable tenseness: The affected compartment feels "wood-like" or tense to palpation.
* Pallor and Pulselessness: Late signs indicating advanced arterial compromise.
* Paralysis: A late sign indicating irreversible neuromuscular damage.
Surgical Warning: The diagnosis of ACS may be severely delayed or obscured in polytrauma patients, individuals with altered sensorium (e.g., traumatic brain injury, intoxication), patients under continuous epidural anesthesia, or young children. In these populations, the threshold for invasive pressure monitoring must be exceedingly low.
Initial Non-Operative Interventions
Upon suspicion of ACS, immediate temporizing measures must be instituted while preparing for definitive surgical decompression:
1. Release of Constriction: Any circular constrictive bandages, splints, or casts must be completely removed. Splitting a cast and its underlying padding down to the skin can decrease compartment pressure by as much as 50% to 85%.
2. Limb Positioning: The limb must be placed precisely at the level of the heart.
* Biomechanics of Positioning: Placing the limb at heart level optimizes the arteriovenous gradient. Elevating the limb above the heart decreases arterial inflow without significantly augmenting venous outflow, thereby exacerbating local tissue ischemia. Conversely, placing the limb below the heart increases venous congestion.
If symptoms do not resolve within 30 to 60 minutes after these appropriate initial treatments, pressure measurement should be repeated. If results remain equivocal or clinical signs persist, emergent fasciotomy is indicated.
INVASIVE PRESSURE MONITORING
Because of the variability of clinical signs, the sensitivity and positive predictive value of the physical examination alone can be low. When clinical findings are equivocal, or when the patient is unreliable, intracompartmental pressure (ICP) measurement is the diagnostic gold standard.
Pressure Thresholds for Fasciotomy
Significant controversy exists regarding the exact absolute pressure threshold for performing fasciotomies. However, contemporary evidence-based practice relies on the Delta P (ΔP) concept:
* ΔP = Diastolic Blood Pressure – Intracompartmental Pressure
* A ΔP of less than 30 mm Hg is an absolute indication for immediate fasciotomy.
* Alternatively, an absolute compartmental pressure greater than 30 mm Hg in the presence of corroborating clinical findings is a widely accepted threshold for surgical intervention.
Measurement Techniques
A variety of invasive devices are available for the measurement of compartment pressures. Measurements should be taken within 5 cm of the zone of maximum injury or fracture site, as pressures dissipate further away from the epicenter of trauma.
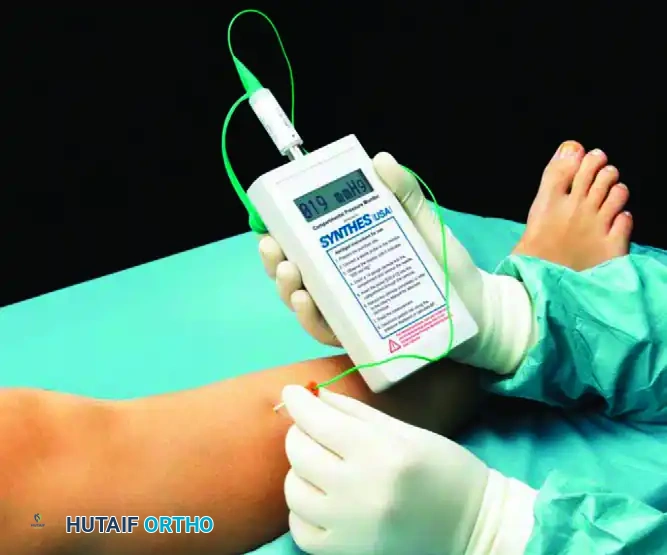
1. Synthes Hand-Held Compartment Pressure Monitor
This is a commercially available, self-contained digital monitor that provides rapid, accurate, and reproducible continuous or spot measurements.
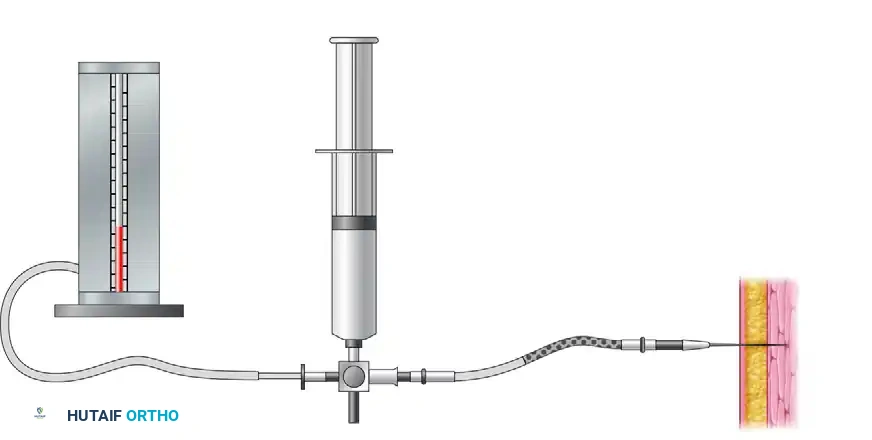
2. The Whitesides Apparatus
A classic, cost-effective method utilizing a three-way stopcock, a mercury manometer (or modern blood pressure monitor), a syringe, and saline. Tissue pressure is measured by determining the amount of pressure within the closed system required to overcome the pressure within the closed compartment and inject a minute amount of saline.
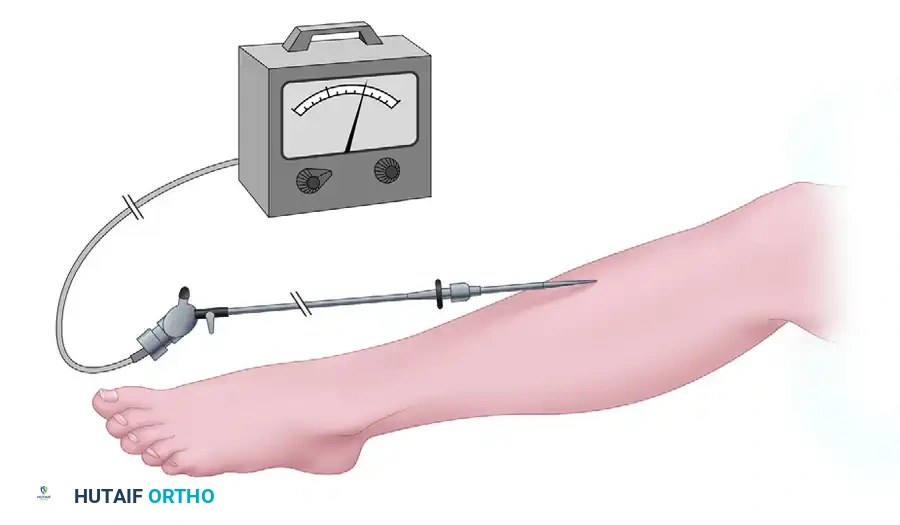
3. Wick Catheter Technique
The wick catheter allows for continuous monitoring of compartment pressures, which is particularly useful in the intensive care setting for obtunded polytrauma patients.
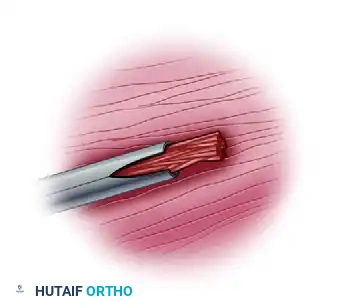
Close-up view of the wick catheter tip, designed to prevent tissue occlusion during continuous pressure monitoring.
Emerging Technologies: Noninvasive methods, such as ultrasonography (measuring submicrometer displacement of the fascial wall) and infrared imaging (detecting temperature differentials), are currently under investigation. While ultrasound has shown a diagnostic sensitivity of 77% and specificity of 93% in healthy models, neither modality has supplanted invasive pressure monitoring as the clinical standard of care.
ACUTE COMPARTMENT SYNDROME OF THE LOWER LEG
The lower leg is the most common anatomical site for acute compartment syndrome, frequently associated with tibial shaft fractures. Animal studies have demonstrated an increased propensity for the development of ACS when reamed intramedullary nailing is utilized; thus, nonreamed nailing or careful pressure monitoring is advised in high-risk tibial fractures.
Anatomy of the Lower Leg Compartments
The lower leg is divided into four distinct, rigid osteofascial compartments:
1. Anterior Compartment: Contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius. Neurovascular structures: Deep peroneal nerve and anterior tibial artery.
2. Lateral Compartment: Contains the peroneus longus and brevis. Neurovascular structures: Superficial peroneal nerve.
3. Superficial Posterior Compartment: Contains the gastrocnemius, soleus, and plantaris. Neurovascular structures: Sural nerve.
4. Deep Posterior Compartment: Contains the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. Neurovascular structures: Tibial nerve and posterior tibial artery.
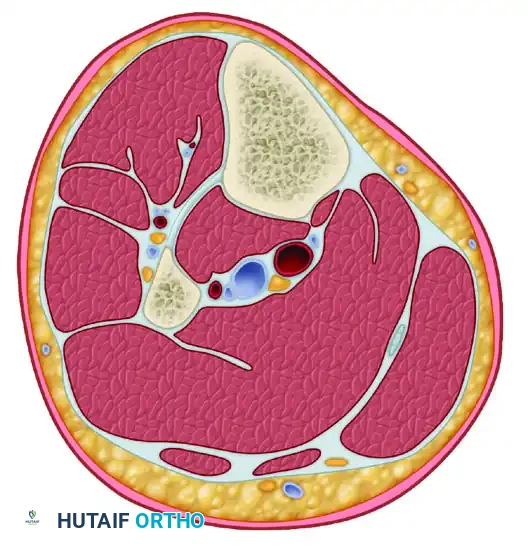
Transverse section through the middle portion of the left leg illustrating the four distinct osteofascial compartments.
Surgical Technique: Double-Incision Four-Compartment Fasciotomy
The gold standard for lower leg ACS is the double-incision four-compartment fasciotomy. This approach ensures complete decompression of all compartments while maximizing skin bridges to prevent necrosis.
Anterolateral Incision:
1. Positioning: The patient is positioned supine. A tourniquet is applied but not inflated unless catastrophic hemorrhage occurs, as tourniquet ischemia confounds the assessment of muscle viability.
2. Incision: Make a longitudinal incision approximately 15 to 20 cm in length, centered halfway between the tibial crest and the fibular shaft.
3. Anterior Compartment Release: Identify the anterior intermuscular septum. Incise the fascia of the anterior compartment longitudinally. Use dissecting scissors to extend the fascial release proximally to the tibial tubercle and distally to the extensor retinaculum.
4. Lateral Compartment Release: Identify the superficial peroneal nerve, which exits the lateral compartment fascia in the distal third of the leg. Protect the nerve. Incise the lateral compartment fascia longitudinally, posterior to the intermuscular septum, extending the release fully proximal and distal.
Posteromedial Incision:
1. Incision: Make a second longitudinal incision, 15 to 20 cm in length, approximately 2 cm posterior to the posteromedial margin of the tibia.
2. Superficial Posterior Compartment Release: Identify and protect the saphenous nerve and long saphenous vein. Incise the fascia over the gastrocnemius-soleus complex longitudinally to decompress the superficial posterior compartment.
3. Deep Posterior Compartment Release: Retract the superficial posterior compartment musculature posteriorly. Detach the soleus bridge from the posterior tibia to expose the fascia of the deep posterior compartment. Incise this fascia longitudinally.
* Pitfall: Failure to adequately release the deep posterior compartment is the most common cause of persistent ischemia and subsequent Volkmann's ischemic contracture in the lower extremity. Ensure the release extends distally behind the medial malleolus if necessary.
ACUTE COMPARTMENT SYNDROME OF THE THIGH
Compartment syndrome of the thigh is significantly less frequent than that of the lower leg due to the larger volume and potential capacity of the thigh's myofascial compartments. However, when it occurs, it is associated with profound morbidity. Studies indicate that up to 17% of patients may require amputation, and over 50% suffer long-term functional deficits.
Etiology and Risk Factors
The most common causes are high-energy blunt trauma (with or without femoral fracture) and vascular injuries. Other etiologies include polytrauma, prolonged limb compression (e.g., drug overdose positioning), military antishock trousers, penetrating gunshot wounds, and severe quadriceps contusions. Factors associated with poor functional outcomes include high injury severity scores, prolonged intervals to decompression, and age older than 30 years.
Anatomy of the Thigh Compartments
The thigh is divided into three distinct compartments by intermuscular fascial extensions, all encased by the robust fascia lata:
1. Anterior Compartment: Contains the quadriceps muscle group, sartorius, femoral nerve, saphenous nerve, and femoral artery/vein. This compartment is surrounded by the stiffest walls (fascia lata and iliotibial tract) and is the most vulnerable to trauma.
2. Medial Compartment: Contains the adductor muscle group, profunda femoris artery, obturator artery, and obturator nerve.
3. Posterior Compartment: Contains the hamstrings (biceps femoris, semimembranosus, semitendinosus) and the sciatic nerve.
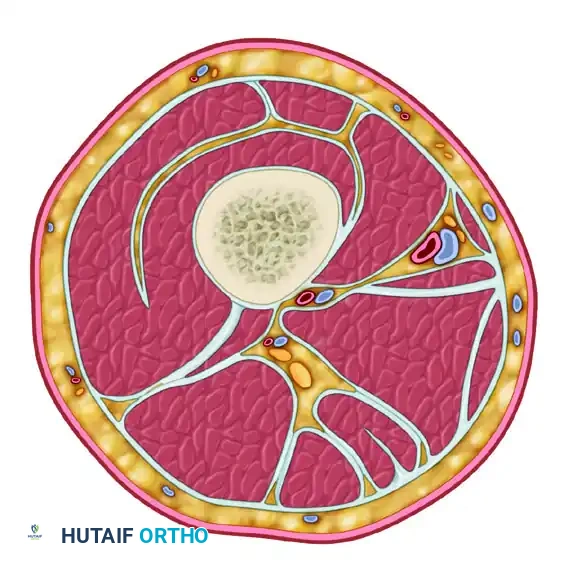
Transverse section illustrating the anterior, medial, and posterior compartments of the thigh.
Compartment-Specific Diagnostic Criteria
Clinical evaluation must isolate the involved compartments to guide surgical decompression. The following criteria (adapted from Mithoefer et al.) dictate compartment-specific findings:
- Anterior Compartment:
- Pain with passive stretch: Passive knee flexion with the hip in extension.
- Motor deficit: Weakness in knee extension.
- Sensory deficit: Anterior thigh (femoral nerve distribution).
- Posterior Compartment:
- Pain with passive stretch: Passive knee extension with the hip in flexion.
- Motor deficit: Weakness in knee flexion, plantar flexion, and dorsiflexion (sciatic nerve distribution).
- Medial Compartment:
- Pain with passive stretch: Passive hip abduction with the knee in extension.
- Motor deficit: Weakness in hip adduction.
- Sensory deficit: Proximal-medial thigh (obturator nerve cutaneous branch).
Surgical Technique: Thigh Fasciotomy
Decompression of the thigh typically requires a single, extensive lateral incision to access the anterior and posterior compartments, which are most commonly involved.
- Incision: Make a longitudinal incision along the lateral aspect of the thigh, extending from the greater trochanter to the lateral epicondyle of the femur.
- Anterior Decompression: Incise the iliotibial band and the fascia lata longitudinally along the entire length of the incision to decompress the anterior compartment.
- Posterior Decompression: Retract the vastus lateralis anteriorly. Identify the lateral intermuscular septum. Incise the septum longitudinally to decompress the posterior compartment. Care must be taken to identify and ligate any perforating branches of the profunda femoris artery to prevent catastrophic hemorrhage.
- Medial Decompression (If Indicated): If the medial compartment is involved (rare), a separate anteromedial incision is made over the adductor musculature, taking care to protect the saphenous neurovascular bundle.
POSTOPERATIVE PROTOCOLS AND COMPLICATIONS
Wound Management
Following fasciotomy, the surgical wounds must never be closed primarily.
* Initial Dressing: The wounds are typically managed with sterile, non-adherent dressings or, preferably, Negative Pressure Wound Therapy (NPWT / VAC dressings) set at -75 to -125 mm Hg. NPWT helps manage exudate, reduces tissue edema, and promotes continuous fascial traction.
* Second Look: A planned return to the operating room is scheduled for 48 to 72 hours post-decompression for wound irrigation, debridement of any evolving necrotic muscle, and reassessment.
* Closure: Delayed primary closure may be attempted using vessel loops or dynamic wound closure devices. If the skin edges cannot be approximated without tension by day 5 to 7, split-thickness skin grafting (STSG) is mandatory.
Complications of Compartment Syndrome
The prognosis is excellent if fasciotomy is performed within 6 to 12 hours of symptom onset. However, delayed diagnosis leads to severe complications:
* Myonecrosis and Infection: Ischemic muscle serves as a nidus for severe bacterial infections, including clostridial myonecrosis (gas gangrene). If fasciotomy is delayed beyond 12 to 24 hours, the risk of infection in necrotic tissue skyrockets. In cases of profound, late-presenting ACS with established dead muscle, extensive debridement or primary amputation may be safer than fasciotomy.
* Volkmann's Ischemic Contracture: The end-stage result of untreated ACS, characterized by the replacement of necrotic muscle with dense, inelastic fibrous scar tissue, leading to severe limb deformity and loss of function.
* Systemic Complications: Rhabdomyolysis resulting from muscle necrosis can precipitate acute kidney injury (AKI) secondary to myoglobinuria. Aggressive intravenous fluid resuscitation and alkalinization of the urine are critical medical adjuncts in late-presenting cases.
===
