Trapeziometacarpal Ligament Reconstruction and Arthroplasty: A Comprehensive Guide
Key Takeaway
Trapeziometacarpal ligament reconstruction, pioneered by Eaton and Littler, is a cornerstone procedure for addressing basal joint instability and early-stage arthrosis. This technique utilizes a distally based strip of the flexor carpi radialis (FCR) tendon to reconstruct the volar beak ligament, restoring biomechanical stability. Advanced modifications, including the Calandruccio interposition arthroplasty, offer robust solutions for end-stage pantrapezial arthritis by combining ligamentous reconstruction with biological interposition.
Introduction and Biomechanics
The trapeziometacarpal (TMC) joint of the thumb is a highly specialized biconcave saddle joint that affords the thumb its unique wide range of motion, including flexion, extension, abduction, adduction, and opposition. However, this mobility comes at the cost of inherent osseous instability. The primary static stabilizer of the TMC joint is the anterior oblique ligament (AOL), also known as the volar beak ligament.
Attenuation or traumatic rupture of the AOL leads to dorsal and radial subluxation of the first metacarpal base under the deforming forces of the abductor pollicis longus (APL) and adductor pollicis. Over time, this altered kinematics results in eccentric cartilage wear, volar beak osteophyte formation, and progressive osteoarthritis.
Trapeziometacarpal ligament reconstruction, originally popularized by Eaton and Littler, aims to restore the stabilizing function of the AOL using a distally based strip of the flexor carpi radialis (FCR) tendon. For more advanced disease, modifications such as the Calandruccio ligament reconstruction and tendon interposition (LRTI) or distraction arthroplasty are indicated.
Classification of Thumb Carpometacarpal Arthrosis
Burton, Eaton, Littler, and Dell proposed classification systems to stage thumb trapeziometacarpal arthrosis. These stages guide surgical decision-making, from isolated ligament reconstruction in early stages to complete trapeziectomy and interposition in late stages.
Table: Classification Systems of Thumb Carpometacarpal Arthrosis
| Stage | Eaton / Burton | Dell |
|---|---|---|
| STAGE I | No joint destruction. Joint space widened if effusion is present. Less than one-third subluxation. | Ligamentous laxity, pain, positive grind test. Dorsoradial metacarpal subluxation. |
| STAGE II | Slight decrease in joint space. Marginal osteophytes < 2 mm. May be one-third subluxation. | Symptoms with heavy use, positive grind test. Narrowed joint space, subchondral sclerosis. |
| STAGE III | Significant joint destruction with cysts and sclerosis. Osteophytes > 2 mm. Greater than one-third subluxation. | Pain with normal use, crepitus. Ulnar osteophyte, less than one-third subluxation. |
| STAGE IV | Pantrapezial degenerative changes. Involvement of multiple joint surfaces. | CMC adduction deformity, MCP joint hyperextension. May have pantrapezial arthritis. |
Clinical Pearl: While radiographic staging is helpful, it does not always reliably correlate with a patient’s subjective symptoms. Surgical intervention should be tailored to the patient's pain level, functional demands, and degree of clinical instability, rather than radiographs alone.
Surgical Technique: Eaton and Littler Trapeziometacarpal Ligament Reconstruction
This technique is primarily indicated for Stage I and early Stage II disease where articular cartilage is largely preserved, but symptomatic instability or painful subluxation is present.
Approach and Exposure
- Incision: Expose the thumb carpometacarpal joint through a Wagner-type incision along the radial border of the first metacarpal. Curve the incision ulnarly within the distal wrist flexion crease, extending as far as the flexor carpi radialis (FCR) tendon.
- Neurovascular Protection: Meticulous superficial dissection is critical. Three specific structures must be identified and protected:
- The superficial branch of the radial nerve (SBRN).
- The superficial branch of the radial artery.
- Palmar cutaneous sensory branches, particularly from the median nerve.
Figure: Incision for exposure, highlighting the superficial branch of the radial nerve and palmar branch of the median nerve.
- Muscle Reflection: Reflect the thenar muscles extraperiosteally from the metacarpal shaft and the volar aspect of the trapezium to expose the joint capsule.
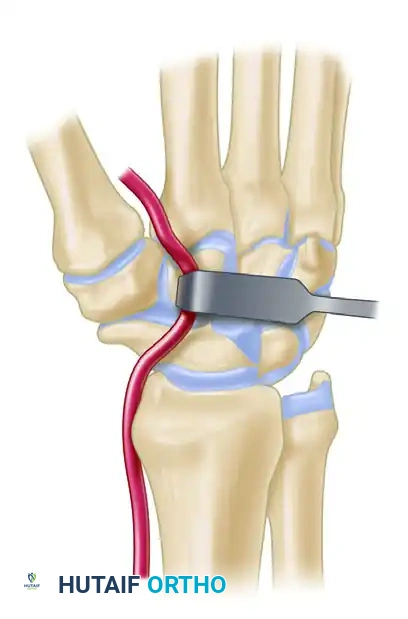
- FCR Tunnel Identification: Deep dissection at the proximal border of the trapezium reveals a sheet of transverse fascial fibers. These fibers form the roof over the separate fibro-osseous tunnel of the FCR. This tunnel is separated from the main carpal tunnel by a vertical septum located between the FCR and the flexor pollicis longus (FPL).
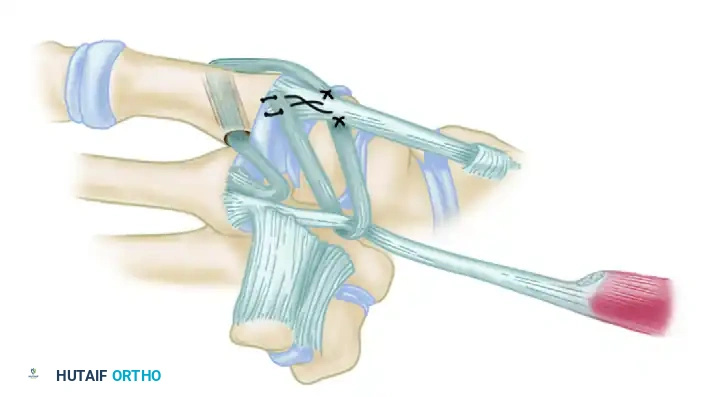
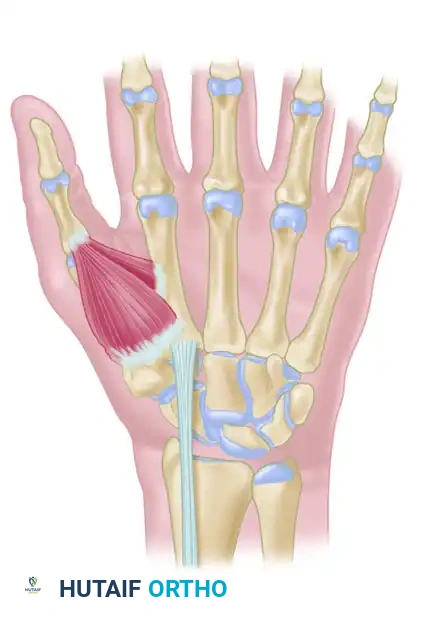
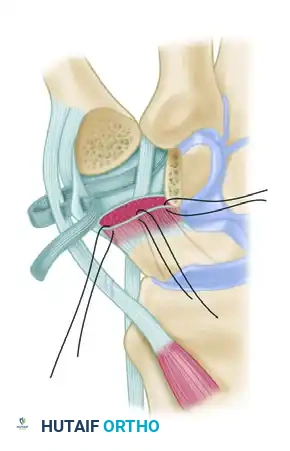
Figure: Schema of ligament support. The key volar ligament is a reflection of the transverse carpal ligament after insertion into the crest of the trapezium. Note the FCR passing directly beneath this ligament.
Joint Preparation and Tunnel Creation
- FCR Release: Incise the reflection of the transverse carpal ligament longitudinally to expose the FCR tendon. The tendon disappears distally beneath a horizontal trapezial ridge projection. Free the tendon approximately 0.5 cm distal to this point by sharp release of the overlying muscle origins.
- Arthrotomy: Perform a longitudinal arthrotomy of the radial capsule. This allows for thorough débridement of hypertrophic synovium, excision of marginal osteophytes, and direct inspection of the articular cartilage. Remove as much diseased synovium as possible.
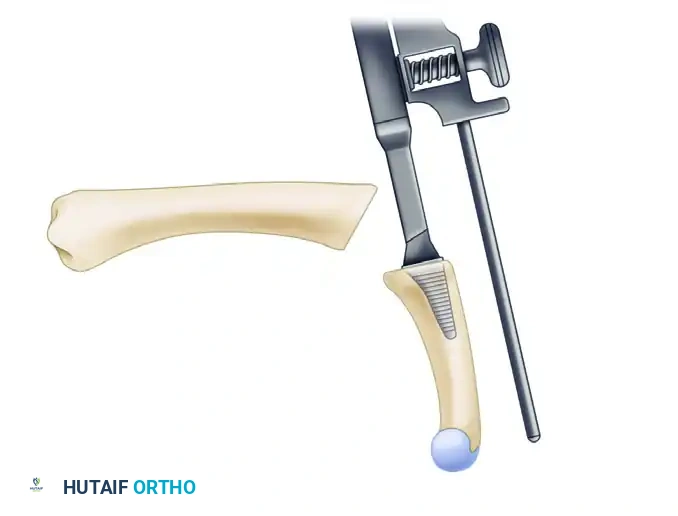
- Metacarpal Tunnel: Create an extraarticular bone tunnel from the dorsal base of the metacarpal to the volar beak apex.
- Vector: The tunnel must be in a plane strictly perpendicular to the thumb nail.
- Starting Point: Start just distal to the dorsal base of the metacarpal, between the extensor pollicis brevis (EPB) and extensor pollicis longus (EPL) tendons.
- Exit Point: The volar beak of the metacarpal. Do not breach the articular surface.
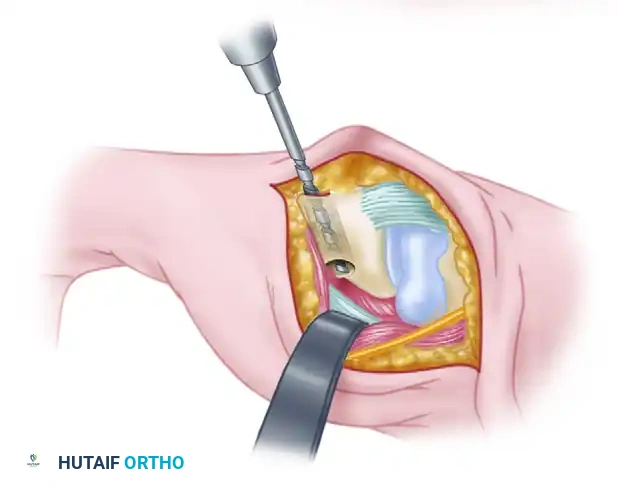
Figure: Gouge tract created in the sagittal diameter of the metacarpal, emerging at its volar beak. A small branch of the radial nerve is retracted volarly.
Intraoperative view demonstrating the creation of the metacarpal tunnel.
Tendon Harvest and Routing
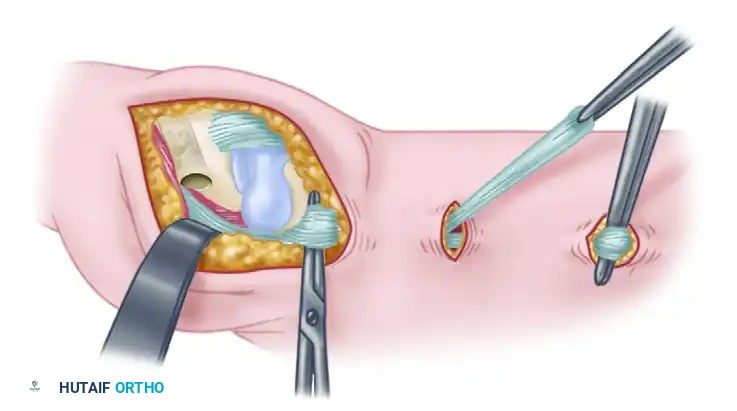
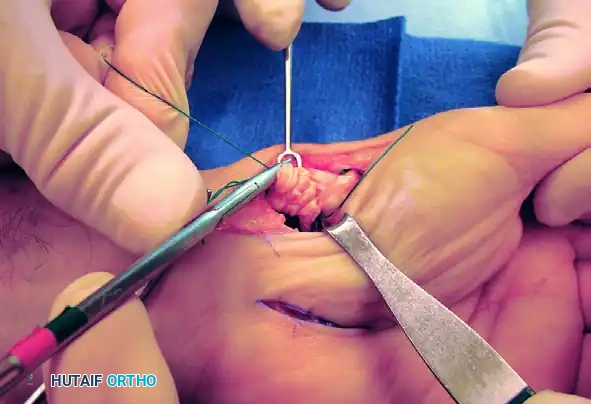
- FCR Strip Harvest: To obtain the "new ligament," make two transverse incisions over the FCR tendon—one at 3 cm and another at 6 cm proximal to the wrist crease.
- Splitting the Tendon: Split a strip comprising exactly half the width of the FCR tendon, taking the radial half. Tunnel this strip beneath the skin bridges to emerge beyond the wrist crease, ensuring it remains in continuity at its distal insertion at the base of the second metacarpal.
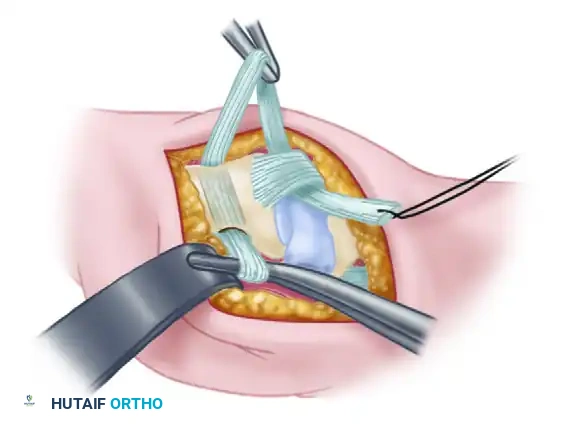
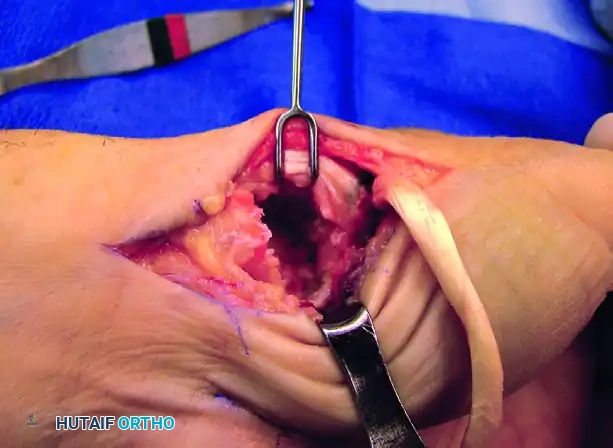
Figure: A 6- to 8-cm strip, representing half the width of the FCR tendon, is split away while remaining in continuity distally.
Intraoperative view of the FCR tendon strip harvested and prepared for routing.
- Rerouting: Continue the split 5 mm distal to the crest of the trapezium. Redirect the free end of the tendon strip across the crest to enter the volar portion of the previously created intramedullary channel at the thumb metacarpal beak.
- Passage: Draw the tendon dorsally through the metacarpal tunnel using a previously placed wire loop or suture passer.
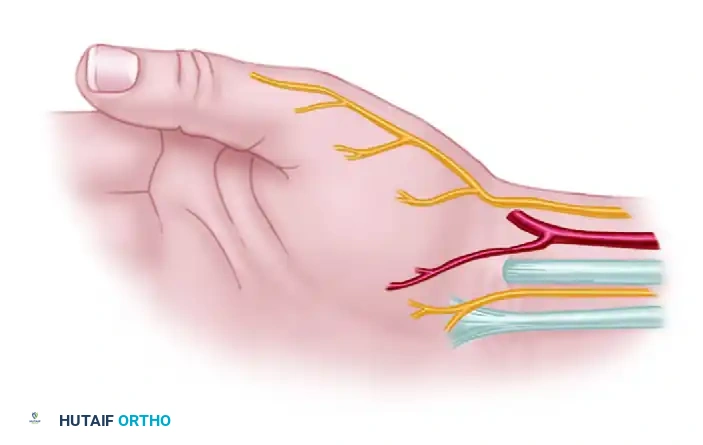
Figure: Path of the FCR strip rerouted to enter the volar channel at the beak of the metacarpal.
Intraoperative view showing the tendon strip being pulled dorsally through the metacarpal tunnel.
Joint Reduction and Fixation
- Reduction: Accurately reduce the TMC joint under direct vision. Hold the thumb in extension and abduction, firmly seating the metacarpal base against the deep facet of the trapezium.
- Pinning: Insert a 0.045-inch or 0.062-inch Kirschner wire (K-wire) from the dorsum of the metacarpal into the trapezium to rigidly maintain the reduction.
Surgical Warning: Ensure the K-wire does not impale the intramedullary portion of the tendon strip, which would compromise tensioning and tendon viability.
- Tensioning: With the joint stabilized, draw the tendon strip taut. Verify that it courses directly from its emergence at the FCR tunnel to the volar beak of the metacarpal, effectively recreating the anterior oblique ligament.

Intraoperative confirmation of joint reduction and K-wire placement.
Final Ligament Weaving
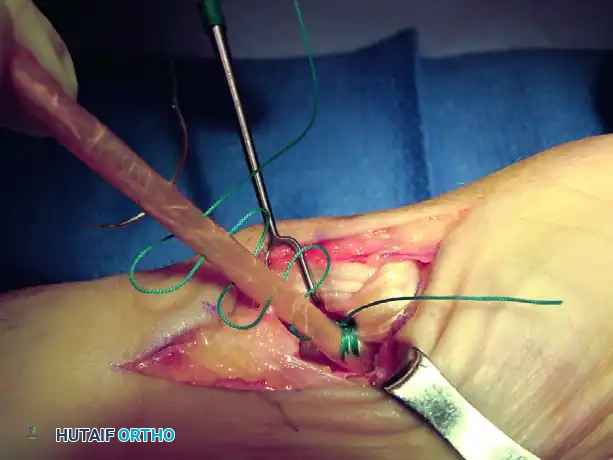
- Dorsal Anchoring: Suture the taut tendon to the dorsal periosteum of the metacarpal.
- Capsular Reinforcement: Route the remainder of the tendon proximally across the dorsal basal joint capsule, passing it beneath the EPB and APL insertions. Suture the strip under tension to the APL bony insertion.
- Final Weave: Pass the remaining tail beneath or through a short split in the intact FCR tendon just proximal to the trapezium. Route it back across the radial margin of the joint to insert into the metacarpal periosteum. Suture the tendon securely at every point where its direction changes.
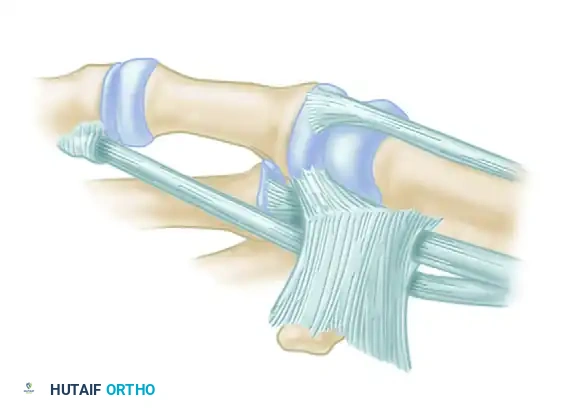
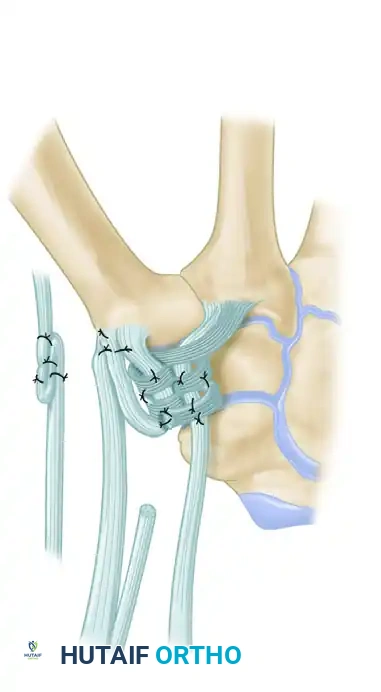
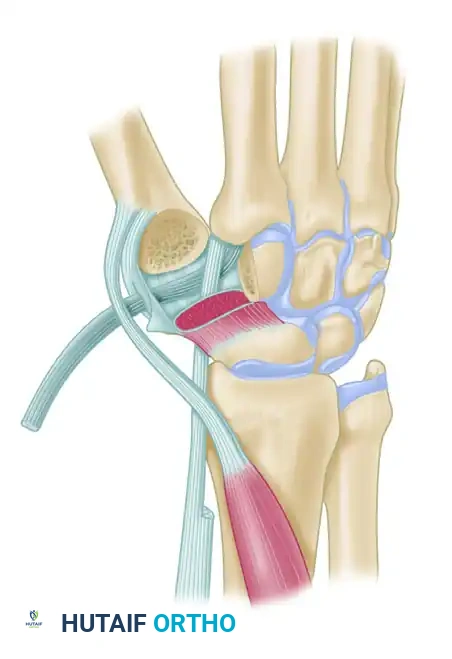
Figure: Schema of volar and radial ligament reconstruction. The complex course of the tendon strip creates robust reinforcement in the volar, dorsal, and radial aspects of the joint.
Intraoperative view of the final tendon weave and capsular reinforcement.
Technique Modification: Calandruccio Interposition Arthroplasty
For patients with Stage III or IV disease (significant joint destruction, pantrapezial arthritis), isolated ligament reconstruction is insufficient. The Calandruccio modification combines complete trapeziectomy with ligament reconstruction and tendon interposition (LRTI).
Trapezial Excision and Metacarpal Preparation
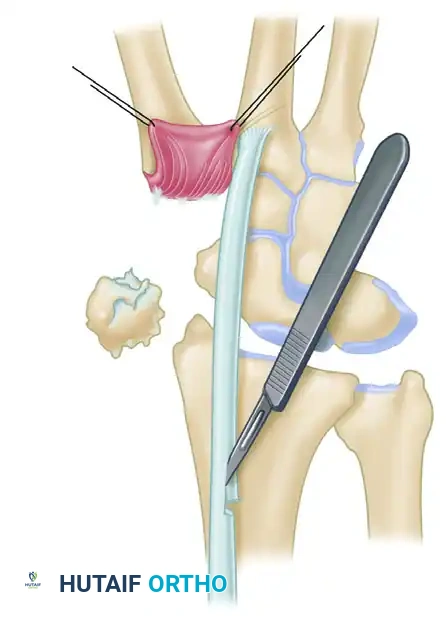
- Trapeziectomy: After exposing the joint through a volar incision along the FCR path and reflecting the thenar muscles, perform a complete excision of the trapezium. Care must be taken to protect the underlying FCR tendon during piecemeal or en bloc resection.
- Bone Tunnel Creation: Using a 4-mm rough burr, create holes through the base of the thumb metacarpal, directing them proximally and radially. Connect these holes using a series of curets (usually up to a No. 2) to form a smooth, continuous tunnel.
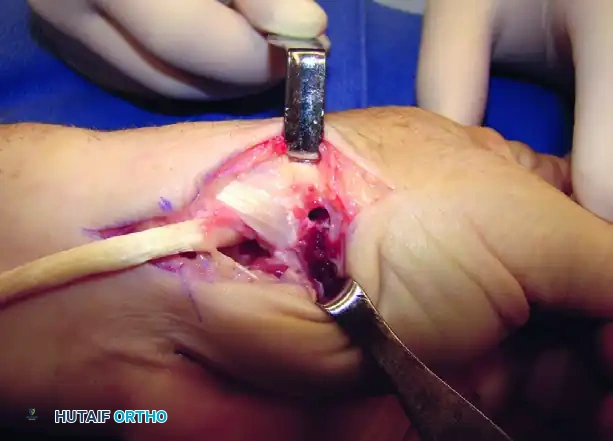
Figure A: Holes made in the thumb metacarpal base following trapeziectomy.
Intraoperative view of the trapezial void and preparation of the metacarpal base.
Tendon Routing and Suspensoplasty
- Tendon Passage: Pass the harvested FCR tendon strip through the newly created bone tunnel. Hold the tendon perpendicular to the index metacarpal shaft.
- Suspension: Approximate the index and thumb metacarpal bases by applying slight ulnarly directed pressure on the thumb metacarpal. Firmly secure the FCR tendon to the APL bony insertion using 2-0 braided nonabsorbable sutures. This step acts as a "suspensoplasty," preventing proximal migration of the thumb metacarpal.
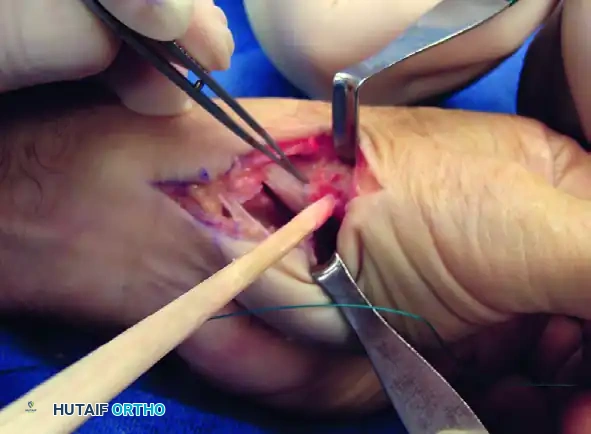
Figure B: FCR tendon passed through the bone tunnel while the index and thumb metacarpal bases are approximated.

Intraoperative view demonstrating the suspension of the first metacarpal.
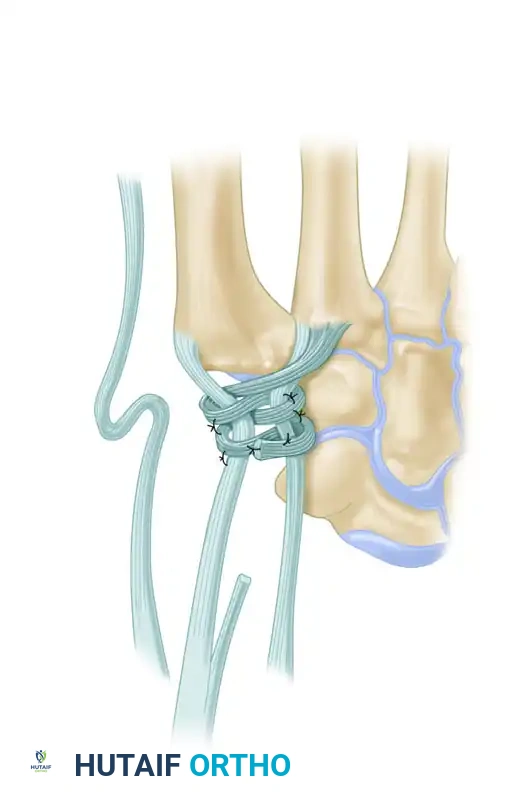
- Intermetacarpal Securing: Pass the FCR tendon between the thumb and index metacarpal bases and secure it to itself with the same nonabsorbable suture.
*Figure C: FCR tendon passed between
Associated Surgical & Radiographic Imaging



You Might Also Like