Tibial Nerve: Surgical Anatomy, Approaches, and Repair
Key Takeaway
The tibial nerve, the larger division of the sciatic nerve (L4-S3), dictates critical plantar flexion and foot intrinsic function. Surgical management of tibial nerve lesions requires meticulous anatomical knowledge, particularly within the popliteal fossa. This guide details the operative approaches, clinical examination protocols, and advanced techniques for closing nerve gaps, including intraneural dissection and autogenous interfascicular grafting, to optimize functional recovery and prevent disabling contractures.
INTRODUCTION TO THE TIBIAL NERVE
The tibial nerve represents the larger, medial, and biomechanically dominant division of the sciatic nerve. Composed of ventral rami fibers from L4, L5, S1, S2, and S3, it is responsible for the motor innervation of the posterior compartment of the leg and the intrinsic musculature of the plantar foot. Furthermore, it provides critical sensory feedback to the plantar aspect of the foot, a function paramount for normal gait, weight-bearing, and the prevention of neurotrophic ulceration.
Injuries to the tibial nerve, whether through high-energy trauma, penetrating injuries, or iatrogenic transection, result in profound functional deficits. The loss of plantar flexion severely impairs the push-off phase of the gait cycle, while the loss of plantar sensation frequently leads to unrecognized microtrauma and subsequent Charcot arthropathy or chronic ulceration. Consequently, the surgical management of tibial nerve lesions demands a rigorous understanding of its topographical anatomy, precise clinical evaluation, and mastery of advanced microsurgical repair techniques.
SURGICAL ANATOMY AND BIOMECHANICS
Proximal Course and the Popliteal Fossa
The tibial nerve formally begins in the distal third of the posterior thigh, just proximal to the apex of the popliteal fossa, at the anatomical bifurcation of the sciatic nerve where the common peroneal nerve diverges laterally.
As it courses distally, the tibial nerve bisects the popliteal fossa longitudinally. Within this space, it lies superficial (posterior) to the popliteal vein and artery, making it the most accessible of the major neurovascular structures in this region. Before passing deep to the tendinous arch of the soleus muscle, the tibial nerve yields several critical motor branches. These branches supply the:
* Plantaris
* Soleus
* Popliteus
* Medial and lateral heads of the gastrocnemius
Surgical Warning: The branching pattern in the popliteal fossa is highly variable. The branches to the gastrocnemius and soleus often arise as a common trunk or tether closely to the main tibial nerve. Aggressive retraction in this area without prior intraneural neurolysis can result in avulsion of these proximal motor branches.
Deep Compartment Transit
After exiting the popliteal fossa, the tibial nerve dives beneath the fibrous arch of the soleus, entering the deep posterior compartment of the leg. Here, it travels alongside the posterior tibial vessels, resting on the tibialis posterior muscle. In this segment, it provides motor branches to the deep flexors: the tibialis posterior, the flexor digitorum longus (FDL), and the flexor hallucis longus (FHL).
CLINICAL EXAMINATION AND DIAGNOSTICS
Accurate clinical evaluation of the tibial nerve requires isolating the specific muscles it innervates and mapping its autonomous sensory zones.
Motor Examination
The muscles supplied by the tibial nerve proximal to the soleus arch (gastrocnemius, soleus) are tested via active ankle plantar flexion against resistance. However, evaluating the deep flexors (innervated after the nerve passes beneath the soleus) requires more nuanced palpation:
* Flexor Hallucis Longus (FHL): The FHL can be difficult to isolate visually, but its tendon is readily palpable posterior to the medial malleolus as it courses toward the medial aspect of the plantar arch during active great toe flexion.
* Flexor Digitorum Longus (FDL): Testing the FDL is challenging due to the overlying musculature. However, in cases of chronic tibial nerve injury where atrophy of the intrinsic foot muscles has occurred, the FDL tendons may become palpable. Otherwise, this muscle is often not reliably palpable for isolated testing.
* Tibialis Posterior: Tested by assessing active foot inversion in a plantar-flexed position.
Sensory Examination and Autonomous Zones
The autonomous sensory zone of the tibial nerve is highly specific. When evaluating a proximal lesion (within or above the popliteal fossa), the zone includes the medial sural cutaneous branch. The general autonomous zone encompasses:
1. The sole of the foot (excluding the medial border of the instep, which is supplied by the saphenous nerve).
2. The lateral surface of the heel.
3. The plantar surface of the toes.
If the injury occurs distal to the popliteal fossa (beneath the soleus), the autonomous zone is smaller because the sural nerve contribution is spared.
Electromyography (EMG) and Nerve Stimulation
Because the tibial nerve lies deep within the adipose tissue of the popliteal fossa, transcutaneous electrical stimulation in this area is notoriously unreliable.
* Proximal Lesions: EMG is strictly indicated to differentiate between complete axonotmesis/neurotmesis and neurapraxia, and to monitor for early signs of reinnervation in the proximal musculature.
* Distal Lesions: The nerve becomes superficial again at the posterior aspect of the medial malleolus (within the tarsal tunnel). Here, the nerve can be stimulated with relative ease to assess distal conduction.
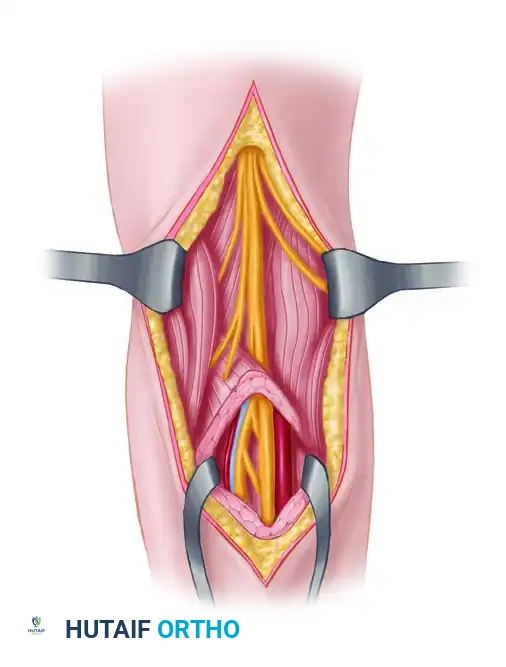
SURGICAL APPROACH TO THE TIBIAL NERVE IN THE POPLITEAL FOSSA
Exposure of the tibial nerve in the popliteal fossa is indicated for exploration of penetrating trauma, tumor resection, or repair of nerve lacerations. The approach must be meticulously planned to avoid debilitating postoperative contractures.
Patient Positioning
The patient is placed in the prone position. All bony prominences are heavily padded. A pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is critical for identifying delicate fascicular structures and avoiding injury to the popliteal vessels.
Incision Design (The Mayfield Approach)
The skin of the popliteal fossa is subject to constant dynamic tension during knee flexion and extension.
Pitfall: Never utilize a straight longitudinal incision across the popliteal crease. A perpendicular incision across these skin folds will inevitably lead to hypertrophic scarring, severe flexion contractures of the knee, and potential skin ulceration.


- Incision: Utilize the Mayfield incision or a curvilinear "S" shaped incision. Begin proximally on the posterior thigh, curving laterally or medially as it approaches the popliteal crease.
- Crease Transit: Traverse the popliteal crease obliquely or transversely.
- Distal Extension: If necessary, extend the skin incision distally along the medial side of the hamstring tendons and continue on the leg just posterior to the medial border of the tibia.
Deep Dissection
- Divide the superficial fascia in line with the skin incision.
- Identify the lesser saphenous vein and the medial sural cutaneous nerve; trace them proximally to locate the main trunk of the tibial nerve.
- Retract the hamstring muscles (semimembranosus and semitendinosus medially; biceps femoris laterally) to expose the proximal apex of the fossa.
- The tibial nerve is identified superficially. The popliteal artery and vein lie deep and slightly medial to the nerve.
- Trace the nerve distally, carefully preserving the motor branches to the gastrocnemius and soleus.
METHODS OF CLOSING GAPS IN THE TIBIAL NERVE
The primary challenge in peripheral nerve surgery is achieving a tension-free neurorrhaphy. When a segment of the tibial nerve is destroyed, closing the resulting gap requires a strategic combination of mobilization, joint positioning, and occasionally, nerve transposition or grafting.
Mobilization and Intraneural Dissection
Although the lesion itself can be fully exposed, a significant gap rarely can be closed by mobilizing the injured segment alone.
1. Extensive Exposure: Exposing and mobilizing the proximal part of the tibial nerve high in the popliteal fossa, or even farther proximally into the thigh, is almost always necessary. By connecting proximal and distal incisions, the nerve can be mobilized from the mid-thigh down to the ankle.
2. Intraneural Stripping: All muscular branches (particularly those to the gastrocnemius and soleus) must be stripped back intraneurally for several centimeters. This careful microdissection separates the fascicles supplying the muscles from the main trunk, allowing the main trunk to advance distally without tethering the proximal muscle bellies.
Joint Positioning for Length
Manipulating the joints of the lower extremity can provide significant nerve excursion, but it must be done with caution.
- Knee Flexion: Flexing the knee to 90 degrees is the most effective method for gaining length in the popliteal region. Because the tibial nerve crosses the flexor surface of the knee joint, 90 degrees of flexion allows for the closure of a gap of 10 to 12 cm.
- Ankle Plantar Flexion (NOT RECOMMENDED): While plantar flexing the foot technically provides additional distal length, it is highly discouraged. Prolonged postoperative immobilization in extreme plantar flexion frequently leads to a rigid, disabling equinus contracture of the ankle that is exceedingly difficult to correct and severely impairs gait.
Nerve Transposition
Occasionally, more length can be obtained by altering the anatomical course of the nerve. The tibial nerve can be transposed either between the soleus and the gastrocnemius, or superficial to both of these muscles.
* Indications: Transposition is especially applicable when the distal muscular branches to the flexor hallucis longus and flexor digitorum longus have been destroyed by the initial trauma.
* Technique with Intact Branches: Transposition can still be performed even if these distal branches are intact, provided they are meticulously dissected and stripped proximally all the way to the popliteal fossa to prevent tethering.
* Muscular Reattachment: If the nerve is transposed, the soleus muscle (which must be detached for the transposition) must be securely sutured back to its origin before the nerve neurorrhaphy is performed.
Clinical Pearl: After you are certain that the defect can be closed, but before the nerve is actually sutured, close the deep fascia of the popliteal fossa. Closing the fascia may slightly reduce the length you have regained. Checking this beforehand ensures that your final nerve suture line will not be placed under unexpected tension once the wound is closed.
Autogenous Interfascicular Grafting
When the gap is too large to be closed by mobilization, knee flexion, and transposition—or if closing the gap would require extreme, awkward, and disabling joint positioning—autogenous interfascicular grafting is the gold standard alternative.
Grafting prevents the joint contractures associated with extreme positioning and ensures a tension-free repair. The sural nerve is the most common donor graft utilized for bridging tibial nerve defects. The grafts are placed in a cable fashion, matching the cross-sectional fascicular topography of the proximal and distal stumps under microscopic magnification.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of a tibial nerve repair is dictated by the methods used to achieve closure.
- Immobilization: If knee flexion was utilized to close a gap, the limb is immobilized in a long-leg cast or rigid hinged brace with the knee locked in the required degree of flexion (up to 90 degrees). The ankle should be maintained in a neutral position (0 degrees) to prevent equinus contracture.
- Duration: Immobilization is typically maintained for 3 to 4 weeks to allow the neurorrhaphy site to heal sufficiently to withstand tensile forces.
- Gradual Extension: After the initial immobilization period, the knee is gradually extended. This is usually accomplished by adjusting a hinged knee brace by 10 to 15 degrees per week. Rapid extension can cause traction injury to the newly repaired nerve.
- Physical Therapy: Once full extension is achieved, aggressive physical therapy is initiated to restore joint mobility, prevent soft tissue adhesions, and maintain the suppleness of the denervated distal musculature until reinnervation occurs.
- Sensory Protection: Because plantar sensation will be absent for an extended period (nerve regeneration occurs at approximately 1 mm per day), patients must be educated on meticulous foot care, daily skin inspections, and the use of custom orthotic offloading footwear to prevent neurotrophic ulceration.
You Might Also Like

