Surgical Management of Thumb Hypoplasia, Adduction Contractures, and Disproportion
Key Takeaway
Thumb hypoplasia and disproportion present complex reconstructive challenges. Management ranges from web space deepening for relative lengthening to complex opponensplasties for adducted thumbs. Conversely, macrodactyly requires the Millesi shortening technique. This guide details adduction contracture release via Z-plasty, opposition restoration using Huber or flexor digitorum superficialis transfers, and precise osteotomies, providing evidence-based protocols for orthopedic surgeons.
INTRODUCTION TO THUMB DISPROPORTION AND HYPOPLASIA
The thumb is the cornerstone of prehension, contributing to approximately 40% to 50% of overall hand function. Its unique kinematics—relying on a highly mobile carpometacarpal (CMC) joint and a complex interplay of intrinsic and extrinsic musculature—enable opposition, pinch, and grasp. Congenital or acquired anomalies affecting thumb length, girth, or posture present profound functional and aesthetic challenges.
Surgical management of thumb disproportion encompasses a broad spectrum of interventions. On one end of the spectrum is the abnormally large or long thumb (macrodactyly), which requires precise osseous and soft-tissue reduction techniques, such as the Millesi thumb shortening procedure. On the other end lies thumb hypoplasia and the adducted thumb, which demand intricate reconstructive efforts including web space deepening, opponensplasties, and ligamentous stabilization. This masterclass provides an exhaustive, evidence-based review of the surgical techniques required to address these complex pathologies.
THE SHORT THUMB: ETIOLOGY AND SYNDROMIC ASSOCIATIONS
A normal thumb typically extends to the level of the proximal interphalangeal (PIP) joint of the adjacent index finger. A thumb is clinically classified as "short" if its distal tip fails to reach this anatomical landmark. Hypoplasia of any or all osseous components (metacarpal, proximal phalanx, or distal phalanx) produces significant shortening.
Clinical Pearl: If a hypoplastic thumb is only short but maintains normal kinematics and stability, surgical correction is rarely indicated. Functional impairment, rather than aesthetic deviation, must drive the surgical decision-making process.
When prehension is significantly limited by a short thumb, deepening of the first web space is often sufficient to create a relative lengthening of the thumb, improving the span for grasping large objects.
Syndromic Pathoanatomy of the Short Thumb
The morphological characteristics of a short thumb often serve as diagnostic clues for underlying systemic syndromes:
- Short and Slender Metacarpal: Frequently a manifestation of Fanconi anemia, Holt-Oram syndrome, or Juberg-Hayward syndrome. These patients require rigorous screening for associated spinal, cardiovascular, and gastrointestinal malformations.
- Short and Broad Metacarpus: Associated with Cornelia de Lange syndrome, hand-foot-uterus syndrome, diastrophic dwarfism, or myositis ossificans progressiva.
- Proximal Phalanx Shortening: Typically associated with isolated brachydactyly.
- Broad and Short Distal Phalanx: Seen in Rubinstein-Taybi syndrome, Apert syndrome, Carpenter syndrome, or hand-foot-uterus syndrome.
- Morphological Variants: The thumb may present as radially deviated (the "hitchhiker’s thumb") or extremely short and stubby (historically termed "potter’s thumb" or "murderer’s thumb"). A slender distal phalanx is highly suspicious for Fanconi or Holt-Oram syndrome.
SURGICAL TECHNIQUE: THUMB SHORTENING (MILLESI PROCEDURE)
While hypoplasia requires lengthening or reconstruction, true macrodactyly or relative overgrowth requires shortening. The Millesi technique is a highly specialized procedure designed to reduce both the osseous length and the soft-tissue envelope of the thumb while preserving the nail complex and tactile sensibility.
Indications and Preoperative Planning
- Indications: True macrodactyly of the thumb, severe post-traumatic disproportion, or specific congenital overgrowth syndromes where the thumb's size mechanically impedes hand function.
- Preoperative Planning: Precise radiographic measurements are required to determine the exact amount of bone to be resected from both the proximal and distal phalanges to achieve symmetry with the contralateral thumb (if normal) or proportional harmony with the ipsilateral fingers.
Step-by-Step Surgical Approach
- Preparation and Exposure:
- The procedure is performed under regional or general anesthesia with strict pneumatic tourniquet control to ensure a bloodless field.
- Begin by excising the distal half of the nail, the underlying nail matrix, and the distal phalangeal tuft. This reduces the overall width and length of the distal segment.
- Dorsal Approach and Distal Phalanx Resection:
- Create a dorsal longitudinal incision overlying the proximal and distal phalanges.
- Carefully elevate the skin flaps, protecting the dorsal sensory branches of the radial nerve and the extensor pollicis longus (EPL) insertion.
- Resect the middle third of the distal phalanx along with the middle third of the overlying nail and matrix.
- Proximal Phalanx Osteotomy:
- Address the proximal phalanx by performing parallel oblique osteotomies to remove its middle third. The oblique nature of these cuts increases the surface area for bony healing compared to transverse osteotomies.
- Reduction and Fixation:
- Reduce the two remaining longitudinal components of the distal phalanx. Compress them and achieve rigid fixation using a transverse Kirschner wire (K-wire).
- Reduce the distal and proximal fragments of the proximal phalanx in their new, shortened configuration. Secure this osteotomy with an oblique K-wire.
- Closure:
- Close the wound by meticulously approximating the skin edges and the remaining nail matrix. Precise matrix repair is critical to prevent postoperative nail dystrophy.
- Leave the K-wires protruding through the skin to facilitate easy removal in the clinic.
Surgical Warning: Over-resection of the nail matrix can lead to complete nail ablation or severe hook-nail deformity. Always ensure adequate proximal matrix remains viable.
Postoperative Care
- A rigid thumb spica splint is applied immediately postoperatively.
- The splint is worn continuously for 3 weeks.
- The K-wires are removed in the outpatient clinic once radiographic evidence of osteotomy healing is confirmed, typically between 4 to 6 weeks.
THE ADDUCTED THUMB: PATHOPHYSIOLOGY AND CLASSIFICATION
An adducted thumb is a complex deformity primarily caused by the absence or partial absence of the thenar musculature, resulting in profoundly deficient opposition.
Pathoanatomy
- Muscular Deficiency: These thumbs typically lack a functional flexor pollicis longus (FPL) muscle and exhibit severe hypoplasia of the abductor pollicis brevis (APB) and opponens pollicis.
- Ligamentous Laxity: The radial collateral ligament (RCL) and ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint are frequently deficient, leading to profound instability during pinch maneuvers.
- Clinical Appearance: The thumb is usually shortened and tapered, featuring a completely flattened thenar eminence and a severely deficient, contracted first web space.
- Genetics: The deformity is usually transmitted as an autosomal dominant trait and is most commonly unilateral.
Manske Classification of Thumb Hypoplasia
Surgical decision-making is heavily dictated by the Manske classification, which categorizes the severity of hypoplasia based on the integrity of the first web space, intrinsic/extrinsic muscles, and the CMC joint:
* Type 1: Minor hypoplasia; all structures present but slightly small.
* Type 2: Narrow first web space, hypoplastic thenar muscles, MCP joint instability.
* Type 3: Deficient extrinsic muscles (FPL, EPL) and skeletal hypoplasia.
* Type IIIA: Stable CMC joint. (Reconstructable)
* Type IIIB: Unstable CMC joint / partial metacarpal aplasia. (Requires amputation and pollicization)
* Type 4: Floating thumb (pouce flottant); deficient osseous structures, specifically the thumb metacarpal.
* Type 5: Complete absence of the thumb.
Clinical Pearl: The presence of a stable CMC joint (Type IIIA vs. Type IIIB) is the absolute critical determinant of whether the thumb should be reconstructed or amputated in favor of index finger pollicization.
SURGICAL RECONSTRUCTION OF THE ADDUCTED THUMB
The primary goals of surgical reconstruction for the adducted thumb are twofold:
1. Complete correction of the adduction contracture (web space deepening).
2. Restoration of dynamic opposition (opponensplasty).
For Type IIIA thumbs, McDonald et al. recommend a staged reconstructive approach initiated at approximately 2 years of age. The first stage includes web space deepening, MCP joint stabilization, and transfer of the flexor digitorum superficialis (FDS) to the FPL. A later stage involves an extensor indicis proprius (EIP) to EPL transfer and a Huber opponensplasty.
1. Web Space Deepening and Contracture Release
The adduction contracture must be released before any tendon transfer can be effective. This is achieved through local tissue rearrangement or regional flaps.
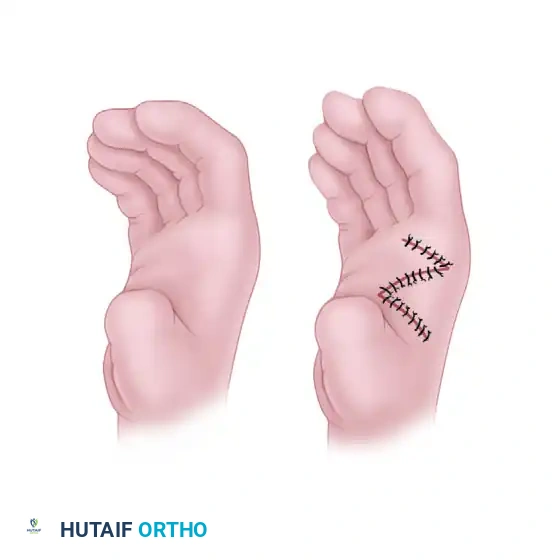
- Z-Plasty Techniques: A two-limb or four-limb Z-plasty can be utilized. However, a standard two-limb Z-plasty rarely attains adequate correction for severe contractures. Less than a 50% increase in web space spread is generally considered an inadequate result.
FIGURE 79-65: Simple Z-plasty of the thumb web. A, Incisions designed along the contracted web. B, Closure after reversal and transposition of the flaps to deepen the web space.
- Flap Reconstruction: For severe contractures, a sliding dorsal flap raised from the radial side of the index finger is preferred. Upton et al. have reported excellent results utilizing pedicled, distally based radial and dorsal interosseous forearm fasciocutaneous flaps to provide robust, pliable tissue to the deficient web space.
2. Restoration of Opposition (Opponensplasty)
Restoring opposition requires transferring a functioning muscle-tendon unit to replicate the vector of the abductor pollicis brevis (APB). The two most popular techniques are the FDS opponensplasty and the Abductor Digiti Quinti (ADQ/ADM) opponensplasty (Huber procedure).
The Huber Procedure (Abductor Digiti Minimi Transfer)
Originally described by Huber and popularized by Littler and Cooley, this procedure transfers the ADM from the hypothenar eminence to the thenar eminence.
* Advantages: It creates a more normal-appearing thenar eminence bulk, which is aesthetically superior for patients with severe thenar flattening.
* Modifications: Chase, and later Upton and Taghinia, described incorporating an overlying hypothenar skin paddle with the ADM muscle belly. This modification eliminates the need to route the muscle through tight, contracted palmar tissues and significantly improves thenar bulk and cosmetic appearance.
Flexor Digitorum Superficialis (FDS) Transfer
The FDS of the ring finger is harvested and routed across the palm (often using the flexor carpi ulnaris or a pulley constructed from the palmar aponeurosis) to insert into the APB insertion or the base of the proximal phalanx.
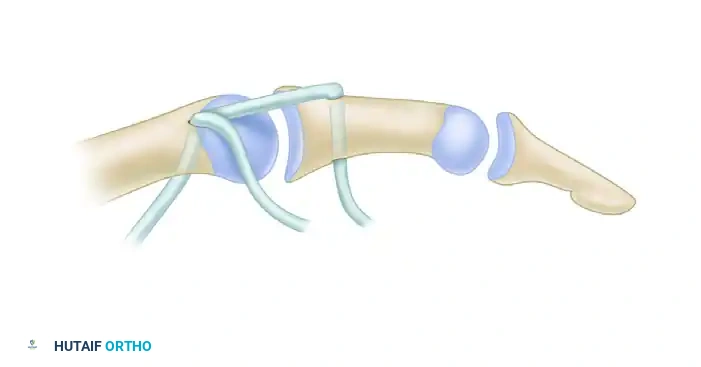
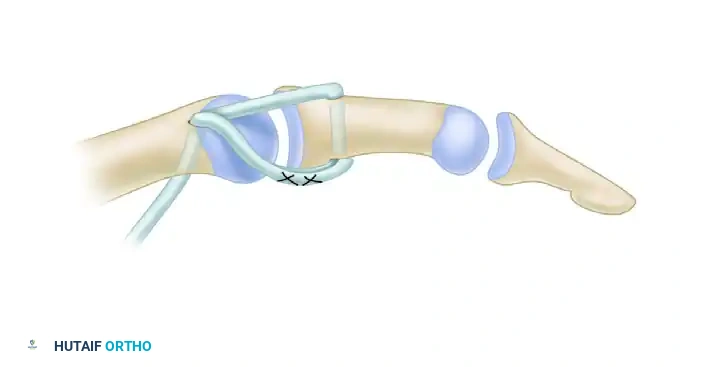
FIGURE 79-64: Flexor digitorum sublimis (superficialis) opposition transfer combined with collateral ligament repair. The tendon is routed to provide an optimal vector for palmar abduction and pronation.
The Littler Abdominal Flap Technique
For severe cases where local tissue is entirely inadequate, Littler and Cooley described the use of a pedicled abdominal flap to reconstruct the soft tissue envelope of the adducted thumb, providing a massive influx of healthy, vascularized tissue.
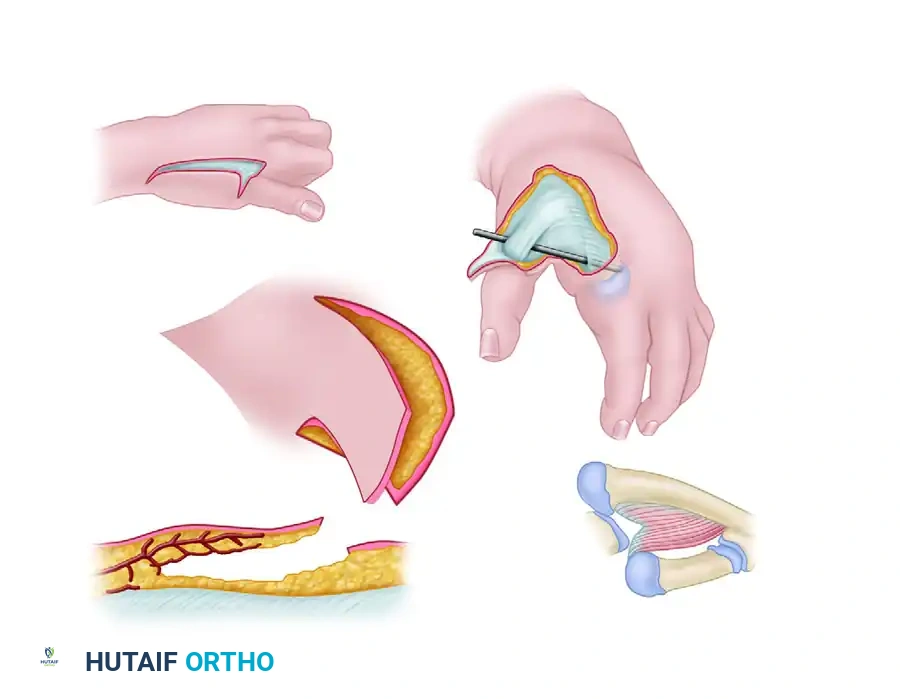
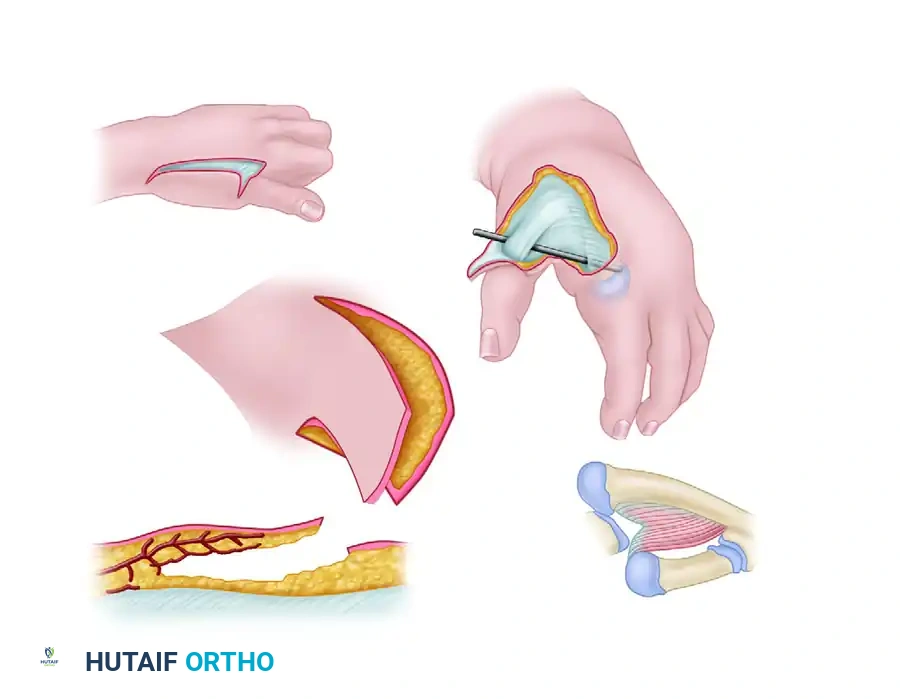
FIGURE 79-63: Littler correction of severe adduction contracture of the thumb utilizing an abdominal flap based on the thoracoepigastric vessels. Note the relationship to the extensor pollicis longus and the adduction-abduction axis.
3. Metacarpophalangeal Joint Stabilization
In the adducted or hypoplastic thumb, the MCP joint is frequently unstable due to profound laxity or absence of the ulnar collateral ligament (UCL). If left untreated, the force of a newly transferred opponensplasty will simply subluxate the MCP joint rather than oppose the thumb ray.
- Reconstruction Techniques: Stabilization can be accomplished by reefing the existing ulnar ligamentous tissues and advancing them distally.
- Augmentation: The repair is often augmented with the distal portion of the FDS tendon when performing an opponensplasty. Alternatively, free tendon grafts (e.g., palmaris longus) or an MCP chondrodesis (in older patients with severe instability) may be required to provide a rigid post against which the index and middle fingers can pinch.
POSTOPERATIVE REHABILITATION AND OUTCOMES
Successful reconstruction of thumb hypoplasia and adduction contractures relies heavily on meticulous postoperative rehabilitation.
- Immobilization: Following opponensplasty and web space deepening, the thumb is immobilized in a bulky thumb spica cast in maximum palmar abduction and opposition. The wrist is typically positioned in slight flexion to remove tension from the FDS transfer.
- Therapy Progression: Immobilization is maintained for 4 weeks. Following cast removal, a custom thermoplastic splint is fabricated. Active range of motion (AROM) exercises are initiated, focusing on cortical re-education of the transferred muscle (e.g., teaching the patient to flex the ring finger to achieve thumb opposition in an FDS transfer).
- Passive Motion: Passive stretching of the first web space is critical to prevent recurrent contracture of the skin flaps or Z-plasties. Night splinting in wide abduction is continued for up to 6 months postoperatively.
By adhering to strict biomechanical principles—ensuring CMC stability, adequately releasing the adduction contracture, providing a robust soft-tissue envelope, and routing tendon transfers along precise anatomical vectors—the orthopedic surgeon can restore profound functional utility to the hypoplastic or adducted thumb.
You Might Also Like