Thumb Metacarpophalangeal Fractures and Dislocations: A Comprehensive Surgical Guide
Key Takeaway
Thumb metacarpophalangeal (MCP) joint fractures and dislocations require precise biomechanical understanding for optimal management. While simple dorsal dislocations often respond to closed reduction utilizing hyperextension and adduction, complex irreducible dislocations necessitate open surgical intervention. This comprehensive guide details the indications, reduction techniques, and surgical approaches—including the preferred dorsal approach for volar plate entrapment—essential for restoring joint stability and function in thumb MCP injuries.
INTRODUCTION TO THUMB METACARPOPHALANGEAL INJURIES
The thumb metacarpophalangeal (MCP) joint is a highly specialized diarthrodial joint that provides a critical balance between mobility and stability, enabling the complex functions of pinch and grasp. Injuries to this articulation, encompassing both fractures and dislocations, are frequently encountered in orthopedic practice, often resulting from high-energy trauma, sports injuries, or hyperextension forces.
Because the thumb MCP joint relies heavily on its robust ligamentous and capsular structures—namely the proper and accessory collateral ligaments, the volar plate, and the dynamic stabilization of the intrinsic musculature—disruptions here can lead to profound functional impairment if mismanaged. This comprehensive guide delineates the pathoanatomy, clinical evaluation, and evidence-based surgical management of thumb MCP fractures and dislocations, providing the orthopedic surgeon with a definitive framework for achieving optimal patient outcomes.
ANATOMIC AND BIOMECHANICAL CONSIDERATIONS
To master the operative management of the thumb MCP joint, a rigorous understanding of its anatomy is paramount. The joint is a condyloid articulation, though its cam-shaped metacarpal head and asymmetric condyles impart unique kinematic properties.
- The Volar Plate: A thick, fibrocartilaginous structure that prevents hyperextension. It is firmly attached to the base of the proximal phalanx and loosely attached proximally to the metacarpal neck via membranous checkrein ligaments.
- Collateral Ligaments: The proper collateral ligaments are taut in flexion, providing lateral stability, while the accessory collateral ligaments are taut in extension, stabilizing the volar plate.
- Sesamoid Bones: Two sesamoids (radial and ulnar) are embedded within the volar plate and serve as insertion sites for the flexor pollicis brevis (FPB) and adductor pollicis, respectively.
- Dynamic Stabilizers: The flexor pollicis longus (FPL) runs centrally, while the intrinsic muscles form a dynamic muscular sleeve that can complicate reduction efforts during dislocation.
CLINICAL PEARL:
The volar plate is structurally analogous to articular cartilage. In complex dislocations, this fibrocartilaginous structure ruptures proximally and becomes interposed between the metacarpal head and the proximal phalanx, acting as an impenetrable mechanical block to closed reduction.
THUMB METACARPOPHALANGEAL FRACTURES
Fractures around the thumb MCP joint most frequently involve the articular margins of the proximal phalanx base or the metacarpal head. The mechanism of injury dictates the fracture pattern, with avulsion fractures and impaction injuries being the most prevalent.
Ulnar Margin Avulsion Fractures
The most common fracture pattern involves the ulnar margin of the proximal phalanx base, typically resulting from an avulsion of the ulnar collateral ligament (UCL). This is the osseous equivalent of a "Skier's Thumb" or "Gamekeeper's Thumb."
Indications for Management
- Nonoperative Management: When the avulsed fragment is small and displaced less than 2 to 3 mm, surgical intervention is generally unnecessary. These injuries are treated similarly to purely ligamentous UCL sprains, utilizing a thumb spica cast or orthosis for 4 to 6 weeks.
- Operative Management: If the fragment is displaced greater than 3 mm, involves more than 20% of the articular surface, or if there is clinical instability, operative fixation is mandated to restore joint congruity and ligamentous tension.
Impaction and Intra-articular Fractures
Axial loading combined with angular forces can result in impaction fractures of the proximal phalanx base or metacarpal head.
- Nonoperative Criteria: Impaction fractures demonstrating less than 20 degrees of dorsal angulation and joint step-off or separation of less than 2 mm can often be managed conservatively with strict immobilization.
- Operative Criteria: Angulated and displaced fractures exceeding these parameters are best treated operatively to prevent post-traumatic osteoarthritis and chronic deformity.
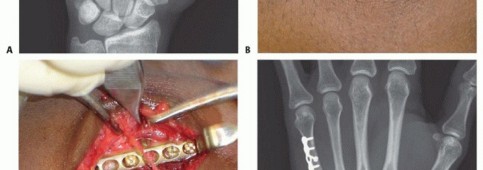
Surgical Techniques for MCP Fractures
When operative intervention is indicated, the goal is anatomic reduction and stable internal fixation.
- Approach: A dorsal or mid-axial incision is utilized depending on the fracture location. For ulnar base fractures, a dorsal-ulnar approach provides excellent exposure.
- Fixation Options:
- K-wires: Suitable for small, comminuted fragments where screw insertion might cause fragmentation.
- Mini-fragment Screws: 1.2 mm to 1.5 mm lag screws provide superior biomechanical compression for single, large avulsion fragments.
- Suture Anchors: If the osseous fragment is too small for fixation but the ligament is avulsed, the fragment may be excised, and the ligament repaired directly to the anatomic footprint using micro-suture anchors.
- Postoperative Protocol: The joint is immobilized in a thumb spica splint. Gentle active range of motion (ROM) is initiated at 2 to 3 weeks, protecting the joint from lateral stress for a full 6 weeks.
THUMB METACARPOPHALANGEAL DISLOCATIONS
Dislocations of the thumb MCP joint are predominantly caused by severe hyperextension injuries. While volar and lateral dislocations occur, dorsal dislocation is by far the most common and presents unique biomechanical challenges.
Classification of Dorsal Dislocations
Dorsal dislocations are strictly classified into two distinct categories based on their reducibility and pathoanatomy:
- Simple Dislocations: Reducible via closed techniques. The proximal phalanx rests in a hyperextended posture (often 60 to 90 degrees) relative to the metacarpal. The volar plate remains volar to the metacarpal head.
- Complex Dislocations: Irreducible via closed techniques. The proximal phalanx and the metacarpal shaft lie in a parallel configuration. The volar plate has ruptured proximally and is interposed within the joint space.
DIAGNOSTIC PITFALL:
A simple dislocation presents with obvious, dramatic hyperextension. A complex dislocation presents with a more subtle, parallel alignment of the thumb. Do not mistake the less deformed appearance of a complex dislocation for a less severe injury; the parallel alignment is the hallmark of volar plate entrapment.
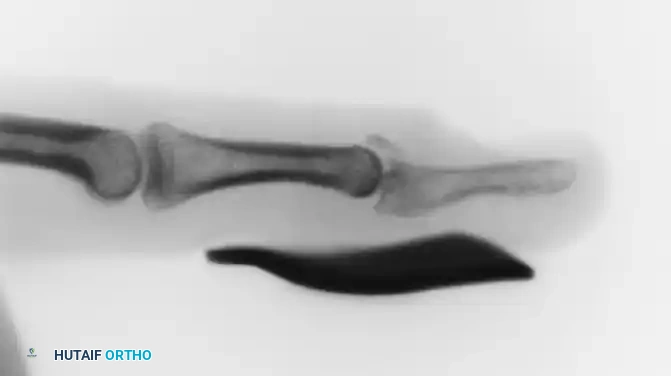
Radiographic Evaluation
Biplanar radiographs (true anteroposterior and lateral views) must always be obtained prior to any manipulation.
* In simple dislocations, the lateral view will demonstrate the proximal phalanx resting dorsally at a steep angle.
* In complex dislocations, the lateral view reveals parallel alignment. Additionally, the presence of a sesamoid bone widened within the joint space is a pathognomonic radiographic sign of volar plate interposition.
MANAGEMENT OF SIMPLE DISLOCATIONS
Early closed reduction of a simple dorsal dislocation is often straightforward, provided the surgeon adheres strictly to biomechanical principles. The primary obstacle to reduction is the tension of the intrinsic muscles and the "buttonhole" effect of the metacarpal head protruding through the volar capsule.
The Closed Reduction Technique
The fundamental rule of reducing a simple thumb MCP dislocation is to avoid longitudinal traction.
SURGICAL WARNING:
Applying longitudinal traction to a simple dislocation will pull the volar plate over the metacarpal head, converting a easily reducible simple dislocation into an irreducible complex dislocation.
Step-by-Step Reduction Maneuver:
1. Positioning and Relaxation: Maintain the thumb in adduction. This relaxes the intrinsic muscles (adductor pollicis and FPB) that are tethering the proximal phalanx.
2. Flexion of the IP Joint: Flex the interphalangeal (IP) joint of the thumb. This relaxes the flexor pollicis longus (FPL) tendon, reducing volar tension.
3. Hyperextension: Gently accentuate the hyperextension of the MCP joint. This unlocks the proximal phalanx from the dorsal metacarpal neck.
4. Distal Translation: Using the examiner's thumb, apply firm, distally directed pressure directly to the dorsal base of the proximal phalanx, pushing it forward over the metacarpal head.
5. Flexion: Once the base of the phalanx clears the metacarpal head, the joint is flexed into its anatomic position.
Post-Reduction Assessment and Care
Following successful reduction, the collateral ligaments must be meticulously assessed for stability. Pure dorsal dislocations rarely exhibit collateral instability.
* Immobilization: The thumb should be immobilized in a thumb spica cast or orthosis with the MCP joint in 20 degrees of flexion for 4 weeks to allow the volar capsule to heal.
* Contraindications: If the initial closed reduction attempt is unsuccessful, repeated forceful attempts are strictly contraindicated. The injury must be recognized as a complex dislocation requiring surgical intervention.
MANAGEMENT OF COMPLEX (IRREDUCIBLE) DISLOCATIONS
When closed reduction fails, the metacarpal head is typically trapped in a "buttonhole" slit comprised of the volar capsule, the volar plate, and the flexor pollicis brevis muscle. The volar plate, tethered tightly over the metacarpal head and neck, acts as an impenetrable barrier. Open reduction is mandatory.
Surgical Approaches: Dorsal vs. Volar-Radial
Historically, there has been debate regarding the optimal surgical approach for complex MCP dislocations.
- The Volar Approach: While it provides direct visualization of the volar structures, it carries a high risk of iatrogenic injury. The radial digital nerve is frequently displaced superficially and tented tightly over the prominent metacarpal head, making it highly vulnerable during the initial incision.
- The Dorsal Approach: First recommended by Farabeuf in 1876, the dorsal approach remains the gold standard for irreducible dislocations of the thumb MCP joint. It avoids the displaced neurovascular bundles and provides direct, unimpeded access to the dorsally displaced volar plate—the primary obstacle to reduction.
Open Reduction via the Dorsal Approach (Farabeuf's Technique)
1. Patient Positioning and Preparation:
The patient is positioned supine with the arm on a hand table. Regional anesthesia (axillary or supraclavicular block) or general anesthesia is utilized. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field.
2. Incision and Dissection:
* A longitudinal or slightly curved dorsal incision is made centered over the thumb MCP joint.
* Careful blunt dissection is performed to identify and protect the terminal branches of the superficial radial nerve.
* The extensor mechanism is exposed. The extensor pollicis longus (EPL) and extensor pollicis brevis (EPB) tendons are identified. The extensor hood is split longitudinally between the EPL and EPB, or the EPB is retracted radially and the EPL ulnarly.
3. Joint Exposure and Pathoanatomy Identification:
* Upon entering the joint dorsally, the articular surface of the proximal phalanx is immediately visible.
* The metacarpal head is obscured by a smooth, white, fibrocartilaginous structure. This is the proximally avulsed volar plate, which has flipped 180 degrees and is draped tightly over the dorsal aspect of the metacarpal head and neck.
4. Volar Plate Division and Reduction:
* Because the volar plate is tethered tightly by the accessory collateral ligaments, simply pulling it volarly is often impossible.
* A longitudinal incision is made directly through the center of the interposed volar plate.
* This division allows the two halves of the volar plate to separate and slip around the medial and lateral margins of the metacarpal head.
* With the mechanical block removed, gentle flexion of the proximal phalanx allows the metacarpal head to easily pop back into anatomic alignment.
5. Closure and Postoperative Protocol:
* The extensor mechanism is repaired with fine absorbable sutures. The skin is closed in a standard fashion.
* Unlike simple dislocations that require prolonged immobilization, the divided volar plate heals rapidly, and prolonged immobilization can lead to severe stiffness.
* Rehabilitation: A bulky dressing and volar splint are applied initially. Motion is started within a few days of surgery. A removable thermoplastic splint is used between therapy sessions to protect the joint while allowing early, controlled active range of motion to prevent extensor tendon adhesions and joint contracture.
COMPLICATIONS AND PITFALLS
Even with meticulous surgical technique, complications can arise following thumb MCP joint injuries. Anticipation and early intervention are key to mitigating these issues.
- Joint Stiffness: The most common complication following both simple and complex dislocations. The thumb MCP joint is highly prone to arthrofibrosis. This underscores the importance of early mobilization following open reduction. If stiffness persists beyond 6 months despite aggressive hand therapy, surgical capsulotomy may be considered, though results are variable.
- Chronic Instability: Failure to recognize and treat a concurrent collateral ligament injury (particularly the UCL) during the management of a dislocation can lead to chronic instability, weakness in pinch grip, and early-onset osteoarthritis. Always stress the joint post-reduction.
- Iatrogenic Nerve Injury: As previously noted, the radial digital nerve is at extreme risk during volar approaches to complex dislocations. Utilizing the dorsal approach significantly reduces this risk. If a volar approach is mandated for other reasons, meticulous superficial dissection is required.
- Avascular Necrosis (AVN): While rare, AVN of the metacarpal head can occur following severe, high-energy dislocations that disrupt the capsular blood supply. Patients presenting with late-onset pain and radiographic collapse should be evaluated for salvage procedures, such as MCP joint arthrodesis.
CONCLUSION
Thumb metacarpophalangeal fractures and dislocations represent a spectrum of injuries that demand a profound understanding of hand biomechanics. While non-displaced fractures and simple dislocations can be managed with conservative measures and precise closed reduction techniques, the surgeon must remain vigilant for the subtle signs of complex, irreducible injuries. By adhering to the principles of avoiding longitudinal traction during closed reduction, and utilizing the time-tested dorsal approach of Farabeuf for volar plate entrapment, the orthopedic surgeon can reliably restore anatomic alignment, joint stability, and essential hand function.
You Might Also Like