Introduction and Epidemiology
The landscape of total hip arthroplasty is undergoing a significant demographic shift, characterized by an increasing prevalence of younger, highly active patients presenting with end-stage hip pathology. Concurrently, increasing global life expectancy necessitates arthroplasty solutions capable of enduring several decades of cyclic loading. Given these demographic trends, the probability of revision arthroplasty later in life is substantially elevated. Consequently, primary surgical interventions must prioritize the absolute minimization of soft tissue and osseous trauma to preserve bone stock for future revision scenarios.
Over the past three decades, the orthopedic community has rigorously investigated minimally invasive surgical approaches designed to mitigate iatrogenic soft tissue damage. Parallel to these developments, the last decade has witnessed a paradigm shift in implant tribology and geometry, culminating in the advent of bone and soft tissue-preserving femoral stems. Among these, femoral neck-preserving implants offer distinct biomechanical and anatomical advantages. Preservation of the femoral neck enhances primary stability, optimizes the distribution of stress loads across the proximal femur, and maintains the physiological insertions of critical musculotendinous units responsible for pelvic posture and dynamic hip kinematics.
Historically, Pipino pioneered the concept of neck-preserving, anatomically contoured prostheses utilizing a collared design. Subsequent iterations, such as the Mayo stem, employed metaphyseal anchorage relying heavily on lateral cortical support. These early short-stem designs aimed to provide robust primary stability, resist micromotion, and facilitate the accurate restoration of patient-specific joint geometry. The fundamental philosophy dictates that the femoral neck should be retained as a primary zone for anchorage and load transfer.





Beginning in 2002, a consortium of orthopedic surgeons collaborated with Plus Orthopedics GmbH (subsequently acquired by Smith and Nephew) to engineer a neck-preserving prosthesis that meticulously accounted for proximal femoral anatomy while ensuring biomechanically stable metaphyseal anchorage. This collaboration yielded the Nanos neck-preserving short-stem implant. The design parameters were derived from an exhaustive morphological analysis of 565 computed tomography scans of patients under the age of 65, focusing on internal cortical geometry and the spatial positioning of the femoral head center. An additional 50 high-resolution scans measured the femoral neck from the subcapital region to the lesser trochanter, enabling optimal three-dimensional polynomial shaping. These morphometric analyses informed the development of a triple-taper cross-sectional geometry, which maximizes rotational stability by increasing the bone-implant contact area while accommodating varying centrum-collum-diaphyseal angles.
Surgical Anatomy and Biomechanics
A profound understanding of proximal femoral anatomy is paramount when utilizing neck-preserving short stems. Unlike conventional diaphyseal-engaging stems, the Nanos implant relies exclusively on metaphyseal fixation. The proximal femur is characterized by a complex trabecular network designed to transmit multi-directional physiological loads from the femoral head to the diaphyseal cortex. The primary compressive trabeculae extend from the medial calcar to the superior aspect of the femoral head, while the secondary tensile trabeculae arc from the lateral cortex to the inferior head.
By preserving the femoral neck, the Nanos stem capitalizes on the dense trabecular bone of the calcar femorale and the robust lateral cortical bone. The preservation of the femoral neck ring maintains the integrity of the proximal femoral hoop stresses, which are often disrupted by standard neck resections. This structural retention significantly mitigates the risk of periprosthetic fractures during broaching and stem insertion.








Biomechanically, conventional stems frequently induce proximal stress shielding due to distal load transfer, leading to calcar resorption in accordance with Wolff's Law. The Nanos stem is engineered to replicate physiological load transmission. Its proximal-medial and distal-lateral polynomial curvatures adapt precisely to the inner cortical contours of the preserved femoral neck. This geometry facilitates a proximal load transfer mechanism, stimulating the calcar and preserving proximal bone mineral density over time.
Furthermore, the triple-taper design of the Nanos stem is critical for primary stability. The taper in the coronal, sagittal, and transverse planes induces compressive forces at the bone-implant interface, resisting axial subsidence. The enlarged surface area provided by the trapezoidal cross-section provides exceptional resistance to torsional forces, a critical factor for short stems lacking diaphyseal splines or flutes. The proportional scaling of the implant sizes ensures that an increase in stem size correlates precisely with an increase in offset, allowing for accurate restoration of the abductor lever arm and physiological joint kinematics.
Indications and Contraindications
Patient selection is the most critical determinant of success in neck-preserving total hip arthroplasty. The Nanos stem is primarily indicated for younger, active patients with robust bone quality capable of supporting metaphyseal load transfer. The morphological characteristics of the proximal femur, specifically the Dorr classification, play a pivotal role in determining suitability. Dorr Type A and Type B femurs, characterized by thick cortices and a distinct metaphyseal-diaphyseal transition, are ideal for short-stem fixation.
Conversely, severe osteoporosis (Dorr Type C bone) represents a definitive contraindication, as the attenuated cortices and sparse trabecular network cannot provide adequate primary stability, leading to a high risk of early subsidence and aseptic loosening. Additional contraindications include severe developmental dysplasia of the hip (Crowe III and IV), which often presents with distorted proximal anatomy and insufficient bone stock for metaphyseal engagement. Massive cystic degeneration of the femoral neck or head-neck junction may also compromise the integrity of the preserved neck ring, rendering standard stems a safer alternative.








Operative Versus Non Operative Management
| Clinical Scenario | Operative Management Nanos THA | Non Operative Management Alternative THA |
|---|---|---|
| Primary Osteoarthritis in Young Active Patient | Indicated. Preserves bone stock for future revisions. Restores offset and biomechanics. | Non-operative: NSAIDs, physical therapy, intra-articular injections (corticosteroid/hyaluronic acid). |
| Avascular Necrosis Ficat Stage III to IV | Indicated if the necrotic lesion does not extend significantly into the basicervical region. | Core decompression (if early stage). Conventional THA if necrosis compromises the femoral neck base. |
| Developmental Dysplasia of the Hip Crowe I to II | Indicated. The short stem can navigate mild anatomical variations and restore the center of rotation. | Conventional THA or custom implants required for Crowe III-IV due to lack of metaphyseal bone stock. |
| Severe Osteoporosis Dorr Type C | Contraindicated. High risk of subsidence and periprosthetic fracture. | Conventional diaphyseal-engaging stem (often cemented) is indicated to ensure adequate fixation. |
| Post Traumatic Arthritis with Deformity | Indicated only if the proximal metaphyseal geometry remains relatively intact and supportive. | Conventional THA with diaphyseal bypass or modular stems to navigate complex proximal deformities. |
Pre Operative Planning and Patient Positioning
Thorough preoperative templating is mandatory to ensure accurate sizing, appropriate neck resection level, and restoration of limb length and global offset. Standardized anteroposterior pelvic radiographs with a magnification marker are utilized. Digital templating software allows the surgeon to superimpose the Nanos stem templates over the proximal femur.
The primary objective during templating is to determine the precise level and angle of the femoral neck osteotomy. Unlike conventional stems where the cut is typically made at a standard angle relative to the lesser trochanter, the Nanos stem requires a high, subcapital osteotomy to preserve the maximum amount of the femoral neck. The templating process should identify the optimal stem size that fills the metaphyseal region, achieving cortical contact laterally and calcar support medially. The surgeon must also evaluate the centrum-collum-diaphyseal angle to ensure the polynomial curvature of the implant aligns perfectly with the patient's native anatomy.








Patient positioning is dictated by the surgeon's preferred surgical approach. The Nanos stem is highly versatile and compatible with all standard and minimally invasive approaches. For the Direct Anterior Approach, the patient is positioned supine on a specialized traction table or a standard radiolucent operating table. This approach exploits the internervous plane between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve), aligning perfectly with the tissue-preserving philosophy of the implant. Alternatively, the anterolateral approach in the lateral decubitus position provides excellent exposure of the femoral neck while minimizing disruption to the posterior soft tissue envelope, thus reducing the risk of postoperative dislocation.
Detailed Surgical Approach and Technique
The surgical technique for the Nanos neck-preserving stem demands meticulous execution, particularly regarding the femoral neck osteotomy and subsequent metaphyseal preparation. The following details the procedure utilizing a minimally invasive anterolateral approach.
Exposure and Capsulotomy
Following standard skin incision and subcutaneous dissection, the fascia lata is incised. The interval between the tensor fasciae latae and the gluteus medius is identified and developed. The anterior third of the gluteus medius and minimus may be elevated from the greater trochanter if necessary, though true tissue-sparing techniques attempt to preserve these insertions entirely. An anterior capsulectomy or capsulotomy is performed to expose the femoral head and neck. Dislocation of the hip is executed with gentle external rotation and extension.
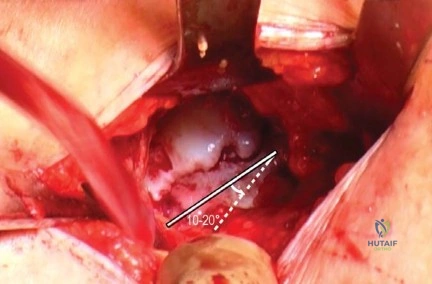
Femoral Neck Osteotomy
The femoral neck osteotomy is the most critical step in Nanos stem implantation. Unlike standard resections that remove the majority of the neck, the Nanos technique requires a high, subcapital cut. Using the preoperative template as a guide, the osteotomy is initiated just distal to the articular cartilage of the femoral head. The angle of the cut should be relatively horizontal to preserve the structural integrity of the inferior calcar and the lateral cortical bridge. Retaining this cylindrical bone stock is essential for the rotational stability of the triple-taper stem design.









Femoral Preparation and Broaching
Following acetabular preparation and cup insertion, attention is directed to the femur. The femoral canal is accessed using a curved box osteotome or a starter awl, ensuring lateralization into the greater trochanter to avoid varus malalignment. Sequential broaching is then commenced.
The broaches for the Nanos stem are specifically designed to compact the cancellous bone rather than extract it, thereby enhancing the density of the metaphyseal bone bed. Broaching must follow the natural anteversion of the preserved femoral neck. The surgeon must pay careful attention to the medial-lateral and anterior-posterior stability of the broach. The final broach should seat firmly on the medial calcar while achieving intimate contact with the lateral cortex. The polynomial curvature of the broach will naturally guide it into the correct alignment.
Trialing and Final Implantation
Once axial and rotational stability of the final broach is confirmed, trial reduction is performed. Leg length, global offset, and soft tissue tension are meticulously evaluated. The hip is taken through a full range of motion to assess for impingement and dynamic stability.
Upon satisfactory trialing, the definitive Nanos stem is introduced. The implant is driven into the prepared metaphyseal envelope until the porous coating is fully engaged with the host bone. The triple-taper geometry will result in an interference fit, providing immediate rigid fixation. The selected modular femoral head is impacted onto the trunnion, and the hip is reduced. A final assessment of stability is conducted before layered closure of the soft tissues.









Complications and Management
While neck-preserving short stems offer significant biomechanical advantages, they are associated with specific intraoperative and postoperative complications that require astute surgical management. The reliance on metaphyseal fixation makes these implants particularly sensitive to errors in surgical technique and patient selection.
Intraoperative periprosthetic fractures are the most frequently encountered complication, primarily occurring during the broaching phase or final stem impaction. Calcar cracks can propagate if the broach is oversized or if the femoral neck osteotomy was performed too distally, compromising the structural ring. Varus malalignment is another significant risk, often resulting from inadequate lateralization of the starting point. When a short stem is placed in varus, it alters the load transfer mechanics, increasing the risk of lateral thigh pain and early aseptic loosening.
Subsidence is a critical postoperative concern. While minor subsidence (less than 2 mm) within the first six weeks may occur as the implant settles into its final interference fit, progressive subsidence indicates a failure of primary stability. This is typically observed in patients with unrecognized poor bone quality (Dorr C) or undersized implants.









Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology | Salvage Strategy and Management |
|---|---|---|---|
| Intraoperative Calcar Fracture | 1.5% to 3.0% | Oversized broach, aggressive impaction, unrecognized osteopenia. | If stable, cerclage wiring of the proximal femur. If unstable, bypass the fracture with a standard diaphyseal-engaging stem. |
| Progressive Subsidence | 2.0% to 4.0% | Undersized implant, Dorr C bone, lack of lateral cortical contact. | Close radiographic monitoring. If symptomatic or progressive beyond 5mm, revision to a standard length uncemented or cemented stem. |
| Varus Malalignment | 3.0% to 5.0% | Inadequate lateralization of the starting awl, failure to follow the native neck version. | Preventative: precise templating and lateralized entry. Postoperative: monitor for loosening; revision if symptomatic aseptic loosening occurs. |
| Aseptic Loosening | < 2.0% at 10 years | Failure of osseointegration, excessive micromotion, stress shielding. | Revision arthroplasty utilizing a standard or revision length diaphyseal stem. |
| Thigh Pain | 1.0% to 2.0% | Modulus mismatch, micromotion at the distal tip of the short stem. | Typically resolves conservatively within 6-12 months. Rule out infection and loosening. |









Post Operative Rehabilitation Protocols
The rehabilitation protocol following Nanos neck-preserving THA is designed to capitalize on the robust primary stability afforded by the metaphyseal interference fit, while respecting the biological timeline of osseointegration. Because the surgical technique inherently preserves bone and, depending on the approach, critical soft tissue structures, patients generally experience an accelerated functional recovery compared to traditional diaphyseal stems.
Immediate Postoperative Phase
Assuming optimal intraoperative fixation and the absence of periprosthetic fractures, patients are typically permitted immediate weight-bearing as tolerated with the assistance of an ambulatory device (walker or crutches). Early mobilization within the first 24 hours is highly encouraged to mitigate the risks of deep vein thrombosis and pulmonary embolism, and to stimulate early proprioceptive recovery. Physical therapy focuses on closed kinetic chain exercises, isometric gluteal sets, and ankle pumps.
Intermediate Phase
Between weeks two and six, the focus shifts to restoring normal gait mechanics and weaning off assistive devices. The preserved musculotendinous insertions, particularly the abductor complex, allow for rapid restoration of the Trendelenburg mechanism. Range of motion exercises are advanced, adhering to any specific precautions dictated by the surgical approach (e.g., avoiding combined extension and external rotation for anterior approaches, or flexion/adduction/internal rotation for posterior approaches).





















