Comprehensive Introduction and Patho-Epidemiology
The terminal Syme procedure, historically codified in the orthopedic literature as the Thompson-Terwilliger procedure, represents a highly reliable, definitive surgical intervention for recalcitrant, end-stage pathology of the distal toe. The fundamental principle of the procedure involves the en bloc amputation of the distal half of the distal phalanx. Inherently, this aggressive resection mandates the complete excision of the nail plate, the germinal and sterile matrices, the lateral and proximal nail folds, and the underlying osseous bed upon which these structures rest. By removing the entire anatomic unit responsible for nail generation and the distal osseous support, the surgeon effectively eliminates the substrate for recurrent nail-based pathology.
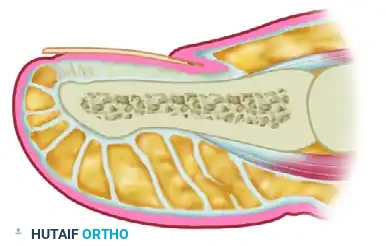
Conceptually, this technique is the digital analog to the classic Syme amputation of the ankle. In a traditional ankle Syme amputation, a robust, highly vascularized plantar soft-tissue flap is advanced dorsally to provide a durable, weight-bearing stump over the distal tibia. The terminal Syme procedure applies this exact biomechanical and reconstructive principle to the distal phalanx of the toe. By utilizing the thick, specialized glabrous skin of the plantar toe pad—which is physiologically engineered to withstand immense shearing and compressive forces—the surgeon covers the dorsal defect created by the matrixectomy. This reconstructive maneuver creates a resilient, pain-free terminal digit capable of withstanding the repetitive microtrauma of normal ambulation and footwear pressure.
The patho-epidemiology of conditions necessitating a terminal Syme procedure is diverse, yet most cases share a common trajectory of failed conservative and less invasive surgical management. Recalcitrant onychocryptosis (ingrown toenail) remains the most prevalent driving pathology. When chronic inflammation, recurrent paronychia, and hypertrophic granulation tissue persist despite multiple partial nail avulsions and chemical matrixectomies, the germinal matrix often becomes scarred, distorted, and hyperplastic. Furthermore, chronic subungual infections can lead to localized osteomyelitis of the distal phalangeal tuft, rendering soft-tissue procedures futile.
While frequently viewed by junior trainees as a procedure of last resort for benign nail pathology, the terminal Syme amputation remains an indispensable, definitive technique in the orthopedic surgeon’s armamentarium. It offers immediate and permanent resolution for patients who have exhausted less extensive options, particularly in the setting of chronic pain syndromes associated with severe nail deformities, subungual neoplasms, or structural hypertrophies of the distal digit. Understanding the epidemiological shift toward definitive single-stage procedures in high-risk populations, such as controlled diabetics with localized apical infections, further underscores the modern relevance of this classic operation.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the distal toe anatomy is an absolute prerequisite to executing the terminal Syme procedure without compromising the functional integrity of the digit. The nail unit is a complex appendage comprising the nail plate, the proximal and lateral nail folds, the hyponychium, the sterile matrix (nail bed), and the germinal matrix. The germinal matrix is the critical structure responsible for the generation of the nail plate. Crucially for the operating surgeon, the germinal matrix extends significantly proximal to the visible eponychium (cuticle), often curving proximally and plantarly to rest directly upon the periosteum of the dorsal base of the distal phalanx. Failure to recognize this proximal extension and resect it in its entirety is the primary anatomical cause of postoperative nail spicules, or "horns."
The osseous anatomy of the distal phalanx dictates the exact level of surgical transection. The phalanx consists of a broad base, a narrow diaphyseal waist, and a distal tuft. The tendinous insertions are paramount: the Extensor Hallucis Longus (EHL) inserts onto the dorsal aspect of the phalangeal base, while the Flexor Hallucis Longus (FHL) inserts onto the broad plantar base. The terminal Syme procedure mandates the transection of the distal phalanx strictly distal to these tendinous insertions. Typically, this safe zone is located 1 to 2 mm distal to the metaphyseal flare. Preserving these tendinous insertions is biomechanically critical; inadvertent proximal transection results in a flail distal interphalangeal (DIP) joint. A flail joint leads to profound instability, altered push-off biomechanics during the gait cycle, and the subsequent development of a rigid hammer toe deformity due to unopposed proximal forces.
The neurovascular arborization within the distal toe is robust, yet highly susceptible to iatrogenic injury. The proper plantar digital arteries and nerves travel along the plantar-medial and plantar-lateral aspects of the digit, arborizing extensively within the plantar pad to form a rich anastomotic network. The specialized glabrous skin of the plantar flap is tethered to the underlying distal phalanx by dense fibrous septa known as the retinacula cutis, which compartmentalize the subcutaneous fat to provide weight-bearing shock absorption.
During the elevation of the plantar flap, the surgical dissection must proceed directly along the periosteum of the distal phalanx. This subperiosteal or strictly extra-periosteal plane ensures that the neurovascular supply to the plantar flap remains entirely uncompromised. The flap must remain robustly vascularized to survive the dorsal transposition and subsequent suturing under mild tension. Compromise of the proper digital arteries at the proximal extent of the dissection will inevitably lead to ischemic necrosis of the terminal flap, transforming a definitive reconstructive procedure into a catastrophic surgical failure requiring further proximal amputation.
Exhaustive Indications and Contraindications
The decision to proceed with a terminal Syme amputation must be carefully weighed against the functional shortening and cosmetic alterations it inherently produces. Patient selection, comprehensive preoperative counseling, and strict adherence to surgical indications are paramount to achieving high clinical satisfaction rates and minimizing postoperative regret.
Primary Indications
The most common indication for a terminal Syme procedure is recalcitrant onychocryptosis that has failed multiple less invasive interventions, such as partial nail avulsion with phenol matrixectomy or Winograd wedge resections. In these patients, the nail matrix is often severely deformed, and the lateral folds are chronically hypertrophic. Subungual and distal phalangeal neoplasms represent another major indication. The procedure serves as an excellent oncologic or excisional approach for tumors localized to the nail unit and distal phalanx, including glomus tumors, subungual exostoses, enchondromas, and early-stage localized malignancies like subungual melanoma in situ or squamous cell carcinoma, provided adequate oncologic margins can be obtained.
Additionally, localized chronic osteomyelitis of the distal phalanx tip—often a sequela of neglected paronychia, puncture wounds, or diabetic foot ulcerations—is a strong indication, provided the proximal bone stock at the base of the distal phalanx remains viable and uninfected. The procedure is also occasionally utilized in pediatric and adult reconstructive surgery to debulk and shorten a severely hypertrophic distal digit in cases of macrodactyly or complex congenital deformities.
Severe Nail Incurvatum
In cases of severe nail incurvatum (pincer nail deformity), the nail plate becomes highly convex, pinching the underlying sterile matrix and distal phalanx, leading to excruciating pain with footwear.

While a terminal Syme procedure is definitive for severe incurvatum, alternative soft-tissue procedures such as isolated nail fold excision without concomitant nail plate removal have been described. However, for severe incurvatum where the nail plate is already pathologically narrow, further reduction in size via standard longitudinal matrixectomies yields a cosmetically displeasing, hyper-narrow nail. In these advanced cases, the terminal Syme is a highly viable, albeit aggressive, alternative that provides definitive pain relief.
Contraindications
Absolute contraindications include active, untreated acute infection (e.g., fluctuant abscess, acute ascending cellulitis) and severe peripheral arterial disease (PAD) with inadequate distal perfusion. Operating through an actively infected field significantly increases the risk of seeding the remaining proximal bone, leading to catastrophic postoperative osteomyelitis. Severe PAD precludes the survival of the transposed plantar flap. Relative contraindications include patient non-compliance, unrealistic cosmetic expectations, and the presence of systemic conditions that severely compromise wound healing without optimization.
| Category | Specific Condition | Rationale / Clinical Consequence |
|---|---|---|
| Primary Indication | Recalcitrant Onychocryptosis | Eradicates deformed matrix; prevents recurrent ingrown nails. |
| Primary Indication | Subungual Neoplasms (Benign/Malignant) | Allows en bloc excision of tumor with adequate deep margins. |
| Primary Indication | Apical Osteomyelitis | Removes infected bone while preserving DIP joint function. |
| Absolute Contraindication | Active Fluctuant Abscess | High risk of seeding proximal bone; requires prior I&D. |
| Absolute Contraindication | Severe Peripheral Arterial Disease | Plantar flap will necrose due to insufficient arterial inflow. |
| Relative Contraindication | Unrealistic Cosmetic Expectations | Patient dissatisfaction due to bulbous, shortened toe appearance. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential for a successful terminal Syme procedure. Clinical evaluation must begin with a rigorous vascular assessment. In patients with a history of diabetes mellitus, smoking, or known peripheral vascular disease, palpable pedal pulses are insufficient. Non-invasive vascular studies, including Ankle-Brachial Indices (ABI), Toe-Brachial Indices (TBI), and arterial Doppler waveforms, should be obtained. A TBI of less than 0.5 or an absolute toe pressure of less than 40 mmHg strongly predicts flap failure and represents a contraindication to the procedure until vascular optimization is achieved.
Radiographic templating is mandatory. Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the foot, or dedicated toe views, are required. The surgeon must scrutinize the distal phalanx to identify the exact location of the metaphyseal flare and the anticipated level of bone transection. In cases of subungual exostosis or suspected osteomyelitis, the extent of osseous involvement dictates whether a terminal Syme is sufficient or if a more proximal amputation at the DIP joint is warranted. The surgeon should mentally template the resection line 1 to 2 mm distal to the flare to ensure preservation of the EHL and FHL insertions.
Anesthesia for the terminal Syme procedure is typically achieved via a highly effective digital block. A combination of a long-acting local anesthetic (e.g., 0.5% bupivacaine) and a shorter-acting agent (e.g., 1% or 2% lidocaine) is utilized. While the historical dogma warned against the use of epinephrine in digital blocks, modern orthopedic literature supports the safety of lidocaine with 1:100,000 epinephrine in healthy patients without significant vasospastic or peripheral arterial disease, as it aids in hemostasis and prolongs the block. However, in vasculopathic patients, plain anesthetics are strictly preferred.
Patient positioning is straightforward but requires attention to ergonomics. The patient is placed in the supine position with the operative foot positioned at the extreme edge of the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the great toe into a neutral, easily accessible position. A sterile digital tourniquet—either a commercial digital ring tourniquet or a tightly wrapped Penrose drain secured with a hemostat—is applied to the base of the digit after exsanguination. The use of a tourniquet is strongly recommended to provide a bloodless surgical field, which is critical for identifying the proximal margins of the germinal matrix and protecting the proper digital nerves during flap elevation.
Step-by-Step Surgical Approach and Fixation Technique
Meticulous surgical technique, characterized by sharp dissection and obsessive attention to anatomical planes, is mandatory. The primary surgical objective is to remove the matrix, nail plate, and distal bone in a single, unfragmented en bloc specimen, thereby virtually eliminating the chance of troublesome nail recurrence or tumor seeding.
Incision Planning and Design
The design of the elliptical incision is the most critical technical step in preventing matrix recurrence and ensuring adequate, tension-free soft-tissue coverage.
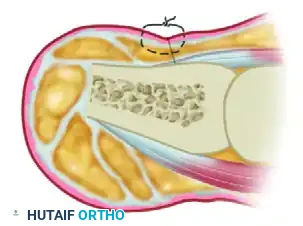

The dorsal proximal margin must be planned with precision. While historical texts occasionally recommended a 4 mm proximal margin, extensive clinical experience dictates that the germinal matrix frequently extends further. It is highly recommended that the proximal skin margin be drawn 6 to 7 mm proximal to the visible cuticle. This ensures complete matrix removal. Because the extrinsic tendon insertions (EHL/FHL) lie proximal to this 7 mm mark, this margin is anatomically safe. The distal margin is drawn 2 to 3 mm distal to the hyponychium to clear the distal sterile matrix. These two incisions are connected medially and laterally to form a complete ellipse around the entire nail unit.
Dissection and En Bloc Resection
The procedure relies on sharp dissection; blunt dissection causes unnecessary tissue trauma and increases the risk of flap necrosis.
1. Make the dorsal incision straight down to the bone proximally. On the lateral and medial aspects, the scalpel blade must remain perpendicular to the bone. Do not bevel the blade toward the center of the phalanx until you have passed completely plantar to the lateral flares of the bone. Beveling too early is a classic resident error that leaves lateral matrix horns behind in the soft tissue.
2. Elevate the plantar flap by using a robust clamp (e.g., a Kocher clamp or towel clip) to firmly grasp the distal aspect of the phalanx, including the nail plate.
3. Apply distal and dorsal traction on the clamp. Using skin hooks to gently retract the plantar flap (avoiding forceps which crush the skin edges), continue sharp dissection along the plantar surface of the phalanx in a distal-to-proximal direction. Stay directly on the periosteum to maximize the thickness and vascularity of the plantar flap.
Bone Transection and Contouring
Identify the metaphyseal flare of the distal phalanx through the bloodless field.
Transect the distal phalanx 1 to 2 mm distal to the EHL and FHL insertions. This is best accomplished using an oscillating microsaw for a perfectly clean cut, though a sharp double-action bone cutter or rongeur is acceptable. Once the bone is transected, release any remaining deep soft tissue attachments to complete the en bloc amputation. Inspect the remaining proximal stump. Use a fine rasp or rongeur to meticulously smooth the dorsal and plantar cortical edges. Any sharp bony prominences left behind will cause pressure necrosis against the plantar flap once weight-bearing resumes.
Hemostasis and Closure
Before closure, the digital tourniquet must be deflated to assess flap perfusion and achieve strict hemostasis.
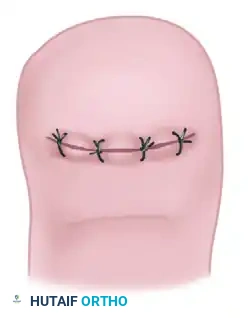
Use bipolar electrocautery sparingly to address specific bleeding vessels. Widespread, indiscriminate use of monopolar electrocautery will cause thermal damage to the subdermal plexus, leading to marginal flap necrosis. Advance the robust plantar flap dorsally over the contoured bone stump. Close the wound using interrupted, nonabsorbable sutures (e.g., 4-0 or 3-0 Nylon or Prolene), employing a vertical mattress technique to ensure slight eversion of the skin edges.
Crucial Surgical Pitfall: Trimming the "Dog Ears"
As the broad, convex plantar flap is sutured to the narrower, flatter dorsal skin margin, prominent medial and lateral "dog ears" will inevitably form. Under no circumstances should these dog ears be trimmed. Excision of these tissue redundancies severs the arborizing proper digital arteries and severely compromises the vascular supply to the distal flap, risking partial or total flap necrosis. These dog ears will remodel and flatten out naturally over several months as the scar matures.
Complications, Incidence Rates, and Salvage Management
While the terminal Syme procedure is highly dependable and boasts excellent long-term success rates, complications can and do arise. The vast majority of these complications stem directly from technical errors during the execution of the procedure rather than inherent flaws in the operation itself.
The most common and frustrating complication for both the patient and the surgeon is the development of troublesome nail spicules, or "horns." This occurs due to incomplete excision of the extreme proximal or lateral margins of the germinal matrix. When the scalpel is improperly beveled during the lateral incisions, microscopic remnants of the matrix are left in the paronychial folds. These remnants generate hard, aberrant spikes of nail plate that pierce the healing skin, causing chronic pain and recurrent infection. Management requires a revision surgery to formally explore the wound, identify the retained matrix tissue, and excise it completely. Prevention via the strict 6-7 mm proximal margin and perpendicular lateral incisions is the only definitive cure.
Flap necrosis is a devastating complication that can compromise the entire reconstructive effort. It is typically caused by excessive tourniquet time, aggressive and indiscriminate electrocautery, or, most commonly, the erroneous trimming of the medial and lateral dog ears during closure. Superficial epidermolysis (partial-thickness loss) can usually be managed with conservative local wound care, silver sulfadiazine, and time. However, full-thickness necrosis requires formal surgical debridement, potential further bone resection to allow tension-free closure, and healing by secondary intention or the application of a split-thickness skin graft.
Epidermal inclusion cysts represent a delayed complication. They form along the dorsal suture line if epidermal elements are inadvertently buried during the closure of the flap. They present as painful, slowly enlarging, firm nodules months or even years after the index surgery. Management requires simple, careful surgical excision of the cyst intact.
| Complication | Estimated Incidence | Etiology / Technical Error | Salvage Management |
|---|---|---|---|
| Nail Spicules (Horns) | 3% - 5% | Incomplete proximal/lateral matrix excision; beveling scalpel. | Revision surgery to excise retained germinal matrix remnants. |
| Flap Necrosis | 1% - 3% | Trimming dog ears; excessive cautery; severe unrecognized PAD. | Superficial: Wound care. Full-thickness: Debridement, possible skin graft. |
| Osteomyelitis | < 1% | Operating in the presence of an active, undrained abscess. | Aggressive bone debridement, culture-directed IV/PO antibiotics. |
| Epidermal Inclusion Cyst | < 1% | Burying epidermal edges during dermal closure. | Elective surgical excision of the cyst. |
| Flail DIP Joint | Rare | Transecting bone proximal to EHL/FHL insertions. | Arthrodesis of the DIP joint or custom orthotic management. |
Phased Post-Operative Rehabilitation Protocols
A strict, phased postoperative protocol is essential to ensure the survival of the transposed plantar flap, minimize edema, and facilitate a return to normal weight-bearing activities. The rehabilitation process requires patient compliance and clear preoperative expectation management regarding the timeline of recovery.
Phase 1: Immediate Post-Operative Period (Days 0-4)
Immediately following the procedure, a bulky, non-adherent compressive dressing is applied. The primary goal during this phase is the mitigation of edema and the prevention of venous congestion within the flap. The patient's foot must be strictly elevated above the level of the heart for the first 48 to 72 hours. Strict elevation minimizes throbbing pain and reduces the hydrostatic pressure on the delicate venous outflow of the transposed flap. Ambulation is strictly limited to essential indoor activities (e.g., bathroom privileges).
Phase 2: Early Mobilization and Wound Care (Days 4-14)
The initial bulky dressing is typically removed and changed at 3 to 5 days postoperatively in the clinic. The flap is inspected for signs of venous congestion, arterial insufficiency, or marginal necrosis. The patient is allowed to ambulate for essential activities utilizing a rigid, wooden-soled, or firm-soled postoperative shoe with an open toe box. This specific footwear prevents any dorsal pressure on the healing flap and eliminates propulsive forces across the distal phalanx during the toe-off phase of gait. Daily dry dressing changes are instituted.
Phase 3: Suture Removal and Transition (Days 14-21)
Sutures in a terminal Syme procedure are left in place longer than standard skin closures. Because the thick plantar flap is sutured to the thin dorsal skin under mild tension, early suture removal risks catastrophic wound dehiscence. Sutures are routinely removed at 14 to 16 days postoperatively, provided the wound edges are fully epithelialized. Once sutures are removed, the patient can begin transitioning into a wide toe-box shoe, such as a deep athletic shoe or a diabetic extra-depth shoe, to accommodate the postoperative swelling and the prominent dog ears.
Phase 4: Long-Term Remodeling and Return to Activity (Months 1-12)
Preoperative patient counseling regarding the final cosmetic appearance is essential to prevent dissatisfaction during this phase.

Initially, the tip of the toe will appear bulbous, shortened, and aesthetically unattractive due to residual edema and the presence of the medial and lateral dog ears. However, over a period of 6 to 12 months, the soft tissues undergo significant physiological remodeling. The dog ears flatten spontaneously, and the plantar pad conforms smoothly to the underlying contoured bone. Patients are typically cleared for all high-impact activities and unrestricted footwear by 6 to 8 weeks, depending on their comfort level.
Summary of Landmark Literature and Clinical Guidelines
The terminal Syme procedure has a rich history in orthopedic literature, and its efficacy is supported by decades of retrospective cohort studies and clinical guidelines. Originally described in the mid-20th century by Thompson and Terwilliger, the procedure was designed to address the high failure rates of partial nail avulsions and simple wedge resections in the pre-antibiotic and early antibiotic eras. Their foundational texts emphasized the necessity of complete en bloc resection of the nail matrix and the biomechanical advantage of the plantar flap.
Modern clinical guidelines and landmark retrospective reviews consistently demonstrate that when the terminal Syme procedure is performed with strict adherence to the technical principles outlined above, the recurrence rate of nail pathology approaches zero percent. A landmark review by Dixon et al. evaluated long-term outcomes of the terminal Syme procedure for recalcitrant onychocryptosis and found a 98% patient satisfaction rate, with zero cases of recurrent nail growth when a 6 mm proximal margin was strictly utilized.
Comparative literature frequently evaluates the terminal Syme against other matrixectomy techniques, such as the Winograd procedure or the Zadik procedure. While the Winograd procedure remains the gold standard for first-time or mild recurrent ingrown toenails, the literature clearly delineates that for end-stage, severely deformed nails, or cases complicated by osteomyelitis, the terminal Syme procedure is vastly superior. The Zadik procedure, which removes the nail and matrix but preserves the distal phalanx, often suffers from higher rates of nail spicule recurrence and leaves a sensitive, vulnerable dorsal scar directly over the bone. The terminal Syme circumvents this by utilizing the robust plantar flap, providing a superior weight-bearing surface.
In conclusion, evidence-based orthopedic guidelines strongly support the terminal Syme procedure as the definitive surgical intervention for complex, recalcitrant distal toe pathology. Through meticulous surgical technique, respect for the neurovascular anatomy, and appropriate postoperative management, surgeons can reliably provide patients with a permanent, pain-free, and highly functional result.
