Synovectomy and Repair of Incomplete Posterior Tibial Tendon Tears

Key Takeaway
Posterior tibial tendon dysfunction (PTTD) often begins with tenosynovitis and incomplete tears. Surgical intervention via synovectomy and tendon imbrication is indicated when conservative measures, such as custom orthoses, fail. This comprehensive guide details the biomechanical rationale, step-by-step surgical approaches for tendon debridement and repair, and tailored postoperative rehabilitation protocols to restore the medial longitudinal arch and prevent disease progression.
Introduction to Posterior Tibial Tendon Dysfunction
Posterior tibial tendon dysfunction (PTTD) is the most common cause of adult-acquired flatfoot deformity. The posterior tibial tendon (PTT) serves as the primary dynamic stabilizer of the medial longitudinal arch. When this tendon undergoes myxoid degeneration, tenosynovitis, or partial tearing, the delicate biomechanical balance of the hindfoot and midfoot is disrupted. This leads to a progressive collapse of the arch, hindfoot valgus, and compensatory forefoot abduction.
Understanding the precise stage of the disease is paramount for determining the appropriate intervention. Early-stage disease (Stage I) is characterized by tenosynovitis without deformity, while Stage II introduces a flexible, passively correctable deformity. Surgical management via synovectomy and repair of incomplete tears is primarily indicated for patients with recalcitrant Stage I disease or early Stage II disease where the tendon retains structural continuity but exhibits significant intrasubstance degeneration or longitudinal splitting.
Clinical Evaluation and Differential Diagnosis
A meticulous clinical examination is required to differentiate isolated PTTD from other causes of medial arch collapse. Patients typically present with medial ankle pain, swelling along the course of the tendon, and progressive loss of the arch.
During the physical examination, the surgeon must assess the flexibility of the hindfoot. The single-leg heel rise test is a critical diagnostic maneuver; inability to perform this test or failure of the hindfoot to invert during heel rise indicates significant PTT insufficiency.
💡 Clinical Pearl: The "Too Many Toes" Sign
Observe the patient from behind while they are standing. In advanced PTTD with forefoot abduction, more toes will be visible on the lateral side of the affected foot compared to the contralateral side. This indicates peritalar subluxation.
It is crucial to rule out other etiologies of flatfoot deformity, such as idiopathic flexible flatfoot, diabetic neuroarthropathy (Charcot foot), or inflammatory arthropathies.
Idiopathic flexible flatfoot in an adolescent patient. This must be differentiated from adult-acquired flatfoot secondary to PTTD.

FIGURE 82-16 Collapse of the medial longitudinal arch (left foot) resulting from diabetic neuropathy. Note the distinct clinical presentation compared to isolated PTT tenosynovitis.
Presentation of Tenosynovitis
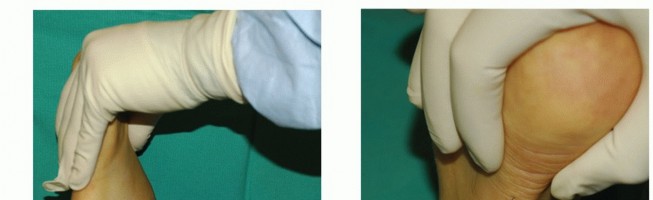
In cases of persistent tenosynovitis, patients will exhibit marked fullness behind the medial malleolus. This swelling is often unresponsive to prolonged immobilization.

FIGURE 82-19 A, Persistent posterior tibial tenosynovitis on the left was unresponsive to many weeks of casting and several months of double upright brace wear with a medial T-strap. Note the fullness behind the medial malleolus on the left, not seen on the right.

FIGURE 82-19 B, Closer view of the medial aspect of the left ankle showing the distinct area of tenosynovitis.
Radiographic Evaluation
Weight-bearing radiographs of the foot and ankle (anteroposterior, lateral, and mortise views) are mandatory. The surgeon should evaluate the talonavicular coverage angle, the talocalcaneal angle (Kite's angle), and the lateral talometatarsal angle (Meary's angle).
Advanced imaging, such as MRI, is highly sensitive for detecting tenosynovitis, longitudinal tears, and intrasubstance degeneration of the PTT, though the diagnosis remains primarily clinical. Radiographs are also essential to rule out structural anomalies such as tarsal coalitions or occult fractures that could mimic or exacerbate PTTD symptoms.

FIGURE 82-15 Middle facet tarsal coalition; note the characteristic beaking of the neck of the talus, which can present with rigid flatfoot and medial pain.

FIGURE 82-17 Standing lateral radiograph showing fracture and fragmentation of the navicular with collapse of the talus into the resulting defect. The arrow points to attempted healing of fractures.
Stage II Disease and Conservative Management
Stage II disease encompasses a wide spectrum of symptoms and varying physical and radiographic findings, characterized primarily by a hindfoot that remains flexible and passively correctable.
Bluman et al. refined the classification system to reflect this spectrum, dividing it into subtypes IIa and IIb:
* Stage IIa: Flexible hindfoot valgus with minimal forefoot abduction.
* Stage IIb: Flexible hindfoot valgus with significant forefoot abduction (typically >30% uncoverage of the talonavicular joint).
Orthotic and Brace Management
Conservative management of Stage II disease is often highly successful and should be exhausted prior to surgical intervention. Most patients obtain significant pain relief with the application of an orthotic device featuring a medial post, or a double upright ankle-foot orthosis (AFO) with a medial T-strap.
The brace is typically configured to allow 20 to 30 degrees of plantar flexion and 10 degrees of ankle extension. While highly effective, compliance can be an issue. Although many men will wear a double upright brace to avoid surgery, women often decline for cosmetic reasons. In these patients, especially if the deformity is not severe, a hinged polypropylene short-leg AFO is a viable alternative. It is lighter, fits into a variety of shoes, and is more cosmetically acceptable, albeit sometimes less comfortable.
📊 Evidence-Based Outcome: Bracing Efficacy
Patients who obtain significant relief with brace wear often find that after 9 to 12 months of routine use, they can transition to regular shoes with custom insoles for extended periods without pain. At our institution, Lin et al. demonstrated that 70% of patients treated with double-upright AFOs (average duration of bracing: 15 months) were brace-free and had not required surgery at a 7-year follow-up. Furthermore, 61% were "satisfied" with their outcomes, and 33% were "satisfied with minor reservations."
Surgical Indications
Surgical intervention is indicated when a minimum of 3 to 6 months of aggressive conservative management (immobilization, custom bracing, NSAIDs, and physical therapy) fails to relieve symptoms, and the patient experiences unacceptable limitations in daily activities. Synovectomy and repair are specifically targeted at tendons that are inflamed and partially torn but have not undergone complete rupture or irreversible elongation.
Surgical Technique 82-1: Synovectomy and Imbrication
This technique is designed for localized tenosynovitis and incomplete longitudinal tears of the posterior tibial tendon.
Positioning and Exposure
- Positioning: Place the patient supine on the operating table. A bump may be placed under the contralateral hip to allow external rotation of the operative leg, providing optimal access to the medial ankle. Apply a proximal thigh tourniquet.
- Foot Position: Allow the foot to rest in gravity equinus. This relaxes the gastroc-soleus complex and decreases tension on the posterior tibial tendon during exposure.
- Incision: Starting at the inferior edge of the navicular tuberosity, carry a straight incision proximally. The incision should remain approximately 1 cm posterior to the prominence of the medial malleolus and continue 3 to 4 cm proximal to the flexor retinaculum.
- Dissection: Carefully dissect through the subcutaneous tissues, taking great care to identify and protect the greater saphenous vein and the saphenous nerve, which lie in close proximity to the surgical field.
Tendon Sheath Release and Synovectomy
- Identification: Identify the posterior tibial tendon at the inferior margin of the wound. Trace it proximally until the musculotendinous junction is visualized.
- Retinaculum Release: Release the pulley behind the medial malleolus (the flexor retinaculum or laciniate ligament) and the deep investing fascia of the distal leg.
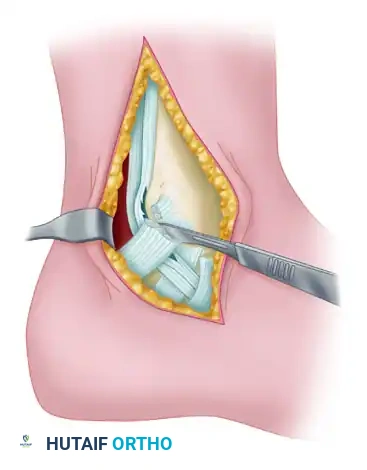
- Debridement: By sharp dissection, meticulously remove all abnormal-appearing, hypertrophic synovium.

FIGURE 82-20 Abundant synovium surrounding the posterior tibial tendon. This extended from the inferior edge of the flexor retinaculum to the tuberosity of the navicular. Evaluation for rheumatoid arthritis and seronegative spondyloarthropathy was negative. The patient was a large-framed man with mild unilateral pes planus and posterior tibial insufficiency secondary to tenosynovitis and loss of tendon excursion through the pulley of the flexor retinaculum.
Tendon Inspection and Repair
- Inspection: Thoroughly inspect the tendon for longitudinal tears, myxoid degeneration, and intratendinous fibrosis.
- Distal Evaluation: Trace the plantar slip of the tendon 1 cm distal to the navicular tuberosity to be absolutely certain it is intact and functional.
- Imbrication: If the tendon insertion into the navicular and the slip plantar to it appear intact, but the tendon is attenuated or exhibits longitudinal splitting, imbricate the tendon across the abnormal-appearing area.
- Excision of the degenerative intrasubstance tissue is performed first.
- The imbrication (often a side-to-side tubularization or a pants-over-vest repair using non-absorbable suture) is performed over a length of 1.0 to 1.5 cm to restore appropriate tension and structural integrity.
- Closure: Leave the flexor retinaculum open to prevent postoperative stenosis and ischemia of the tendon. Close the subcutaneous tissue and skin in a standard layered fashion.
⚠️ Surgical Warning: Flexor Retinaculum Management
While leaving the flexor retinaculum open prevents restrictive adhesions and decompression of the tendon sheath, the surgeon must ensure that the tendon does not bowstring anteriorly during active inversion and plantar flexion. If bowstringing is a risk, a partial or Z-lengthened closure of the retinaculum may be considered, though open management is standard for severe tenosynovitis.
Surgical Technique 82-2: Extended Exposure
When preoperative imaging or clinical examination suggests more extensive proximal involvement, or if a complete disruption is suspected, a more extensile approach is required.

Surgical exposure demonstrating the posterior tibial tendon after release of the flexor retinaculum and excision of the tendon sheath.
Extended Incision and Deep Dissection
- Incision: Expose the posterior tibial tendon through an extended incision beginning 3 to 4 cm proximal to the tip of the medial malleolus. Curve it posterior to the malleolus and extend it to 3 to 4 cm distal to the navicular tuberosity.
- Rationale: This extensive incision is necessary to allow adequate evaluation of the condition of the posterior tibial muscle-tendon unit proximal to the flexor retinaculum.
- Distal Exposure: The incision should be distal enough to reach the Master Knot of Henry (the crossover point of the flexor digitorum longus and flexor hallucis longus). However, extreme caution must be exercised not to compromise dissection around the medial plantar neurovascular bundle.
- Pathologic Findings: Upon exposure, the posterior tibial tendon may be completely disrupted with rounding of the proximal stump. The proximal stump may appear to end in hypertrophic synovial tissue. Once the synovium is removed, the true extent of the tendon defect or degeneration can be accurately assessed, dictating whether a simple repair is sufficient or if a tendon transfer (e.g., FDL transfer) is required.
Postoperative Care and Rehabilitation
The postoperative protocol must be highly individualized. The length of cast immobilization and protected weight-bearing varies depending on the appearance of the tendon at surgery—specifically, the evaluation of its structural integrity and the extent of dissection necessary to rid the tendon of inflamed synovium.
Standard Protocol for Moderate to Severe Involvement
- Initial Immobilization: In most cases, weight-bearing is delayed for 4 to 6 weeks. The leg is immobilized in a well-padded posterior splint in slight equinovarus until the surgical wound is completely healed (typically 2 weeks).
- Early Mobilization: After wound healing, mobilization of the tendon within its sheath is encouraged. The patient is transitioned to a removable splint or controlled ankle motion (CAM) boot. Minimal resistance exercises (active range of motion) are initiated to prevent intrasheath adhesions.
- Obese Patients: In markedly overweight patients with an abnormal-appearing tendon, the mechanical stresses on the repair are significantly higher. After the extended period of NWB support, a double upright brace with a medial T-strap should be worn for an additional 3 months to protect the healing tendon.
Protocol for Mild Involvement
If the involvement is less severe (e.g., isolated tenosynovitis with minimal intrasubstance tearing), the protocol can be slightly accelerated, though caution is still required as wounds in this area may heal poorly due to watershed vascularity.
- Immobilization: The foot should be left in resting equinovarus in a non-weight-bearing cast for 2 to 3 weeks.
- Transition: After 2 to 3 weeks, sutures are removed, and a walking boot is worn for another 3 to 4 weeks, allowing progressive weight-bearing as tolerated.
Managing Postoperative Complications
- Edema: Edema about the ankle, especially medially, may continue for a prolonged period after surgery. The patient should be informed of this preoperatively and assured that it will eventually resolve. The use of a medical-grade support hose (compression stocking) for 2 to 3 months after cast removal is highly beneficial.
- Arch Restoration: If the flattening of the arch was mild preoperatively and the tendon appeared reasonably normal and robust at the conclusion of the surgery, the deformity should correct with time and appropriate rehabilitation.
- Recurrence: Recurrence of isolated tenosynovitis following a thorough surgical synovectomy and proper postoperative bracing is uncommon. However, failure to address underlying biomechanical faults (e.g., tight heel cord) can lead to continued arch collapse.
📚 Medical References
- posterior tibial tendon. Results in patients who have a varus deformity of the foot due to spastic cerebral palsy, J Bone Joint Surg 73A:734, 1991.
- Barrasso JA, Wile PB, Gage JR: Extraarticular subtalar arthro desis with internal fi xation, J Pediatr Orthop 4:555, 1984.
- Bassett FH III, Baker LD: Equinus deformity in cerebral palsy. In Adams JP, ed: Current practice in orthopaedic surgery, vol 3, St Louis, 1966, Mosby. Bell KJ, Ounpuu S, DeLuca PA, et al: Natural progression of gait in children with cerebral palsy, J Pediatr Orthop 22:677, 2002.
- Bennett GC, Rang M, Jones D: Varus and valgus deformities of the foot in cerebral palsy, Dev Med Child Neurol 24:499, 1982.
- Bisla RS, Louis HJ, Albano P: Transfer of tibialis posterior tendon in cerebral palsy, J Bone Joint Surg 58A:497, 1976.
- Bleck EE: Spastic abductor hallucis, Dev Med Child Neurol 9:602, 1967.
- Bleck EE: Forefoot problems in cerebral palsy: diagnosis and management, Foot Ankle 4:188, 1984.
- Bottos M, Gericke C: Ambulatory capacity in cerebral palsy: prognostic criteria and consequences for intervention, Dev Med Child Neurol 45:786, 2003.
- Bourelle S, Cottalorda J, Gautheron V, et al: Extra-articular
You Might Also Like