Surgical Anatomy and Operative Management of the Lumbar Plexus and Femoral Nerve
Key Takeaway
The lumbar plexus and its terminal branches, notably the femoral and obturator nerves, are critical for lower extremity motor function and stability. Iatrogenic or traumatic injuries to these structures demand precise clinical evaluation and meticulous surgical intervention. This guide details the complex surgical anatomy, diagnostic protocols, and step-by-step operative approaches for femoral nerve exploration and repair, providing orthopedic surgeons with evidence-based strategies for managing significant nerve gaps.
SURGICAL ANATOMY OF THE LUMBAR PLEXUS
The lumbar plexus is a complex neural network essential for the motor and sensory innervation of the lower extremity and pelvic girdle. It is formed by the junction of the anterior primary rami of L1, L2, L3, and L4. White rami communicantes leave the L1 and L2 roots, less frequently L3, and rarely L4. Crucially, all nerves within the plexus receive gray rami communicantes from the sympathetic chain, integrating autonomic function with somatic motor and sensory pathways.
The L4 nerve root holds unique anatomical and clinical significance. It makes a substantial contribution to the formation of the sacral plexus by joining with the L5 anterior primary ramus to form the lumbosacral trunk. Because of its bifurcating contribution to both the lumbar and sacral plexuses, the L4 nerve is frequently referred to as the nervus furcalis (the "forked nerve").
Clinical Pearl: Pathologic processes affecting the L4 nerve root (such as a far-lateral disc herniation at L4-L5) can present with a confusing constellation of symptoms that overlap both femoral (lumbar plexus) and sciatic (sacral plexus) distributions.
THE OBTURATOR NERVE
Anatomy and Course
The obturator nerve arises from the anterior divisions of the L2, L3, and L4 ventral rami. It descends through the psoas major muscle, emerges from its medial border, and runs along the lateral wall of the lesser pelvis. It exits the pelvis by passing through the obturator canal (within the obturator foramen) to enter the medial compartment of the thigh.
Upon exiting the obturator canal, the nerve divides into anterior and posterior divisions, separated by the adductor brevis muscle.
Motor and Sensory Innervation
- Anterior Division: Supplies motor innervation to the adductor longus, gracilis, adductor brevis, and occasionally the pectineus. It also provides articular branches to the anterior aspect of the hip joint.
- Posterior Division: Supplies motor innervation to the obturator externus, the adductor magnus (adductor minimus portion), occasionally the adductor brevis, and provides articular branches to the posterior aspect of the knee joint.
- Cutaneous Innervation: The cutaneous branches supply the medial thigh and, occasionally, the medial aspect of the knee.
Surgical Warning: The referred pain pattern from a diseased hip joint to the medial knee is mediated by the dual articular innervation of the obturator nerve. Always evaluate the hip in a patient presenting with isolated medial knee pain and a normal knee examination.
Pathoanatomy and Mechanisms of Injury
The obturator nerve is vulnerable to compression and traumatic injury at several distinct anatomical choke points:
* Pelvic Pathology: The nerve may be compressed against the rigid wall of the pelvis by space-occupying lesions, such as intrapelvic tumors, hematomas, or a gravid uterus.
* Trauma: Because of its intimate relationship with the superior pubic ramus, the nerve is frequently injured in pelvic ring fractures or acetabular fractures.
* Positional Injury: Acutely flexed positions of the hip during prolonged surgical procedures can compress the nerve against the pubis.
* Inflammatory/Infectious: Due to its proximity to the sacroiliac and hip joints, severe joint disease, infection, or trauma can secondarily involve the obturator nerve.
Clinical Evaluation and Management
In significant lesions of the obturator nerve, clinical findings include:
* Profound atrophy of the medial compartment of the thigh.
* Sensory disturbances (hypesthesia or paresthesia) over the distal medial surface of the thigh and medial knee.
* Weakness or complete paralysis of hip adduction.
Obturator Neurectomy:
While traumatic injuries may require neurolysis or repair, intentional transection of the obturator nerve (obturator neurectomy) is a recognized therapeutic intervention. It is highly beneficial in relieving severe adductor spasticity in conditions such as cerebral palsy or severe upper motor neuron lesions, which cause debilitating "scissoring" of the lower extremities, impeding perineal hygiene and ambulation.
THE FEMORAL NERVE
Anatomy and Course
The femoral nerve is the largest branch of the lumbar plexus, formed by the union of the posterior divisions of the L2, L3, and L4 roots. It descends through the substance of the psoas major muscle, emerging from its lower lateral border. It then passes distally through the retroperitoneal space, deep to the iliac fascia.
The nerve enters the anterior compartment of the thigh by passing deep to the inguinal ligament. Crucially, it remains lateral to the femoral artery, separated from the vascular bundle by a portion of the psoas fascia.
Clinical Pearl: Remember the anatomical mnemonic for the femoral triangle contents from lateral to medial: NAVEL (Nerve, Artery, Vein, Empty space, Lymphatics). The femoral nerve is not enclosed within the femoral sheath, which contains only the artery, vein, and lymphatics.
Just distal to the inguinal ligament, the femoral nerve arborizes rapidly into a "cauda equina-like" spray of anterior and posterior branches.
Motor and Sensory Innervation
- Anterior Branch: Divides into the intermediate cutaneous and medial cutaneous nerves, supplying the anteromedial aspect of the thigh. Its motor branches supply the pectineus and the sartorius muscles.
- Posterior Branch: Provides the muscular innervation to the quadriceps femoris (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius).
- The Saphenous Nerve: The largest cutaneous branch of the posterior division. It continues distally with the femoral vessels into the subsartorial (Hunter's) canal, pierces the deep fascia along the medial side of the knee to become subcutaneous, and supplies the skin on the anteromedial aspect of the leg, extending distally to the medial malleolus and the medial arch of the foot.
Mechanisms of Injury
Femoral nerve injuries are often overlooked in the acute trauma setting due to concurrent life-threatening injuries. Common etiologies include:
* Penetrating Trauma: Deep lacerations or gunshot wounds to the lower abdomen or groin. These are frequently associated with catastrophic vascular injuries (iliac or femoral artery) and hollow viscus injuries (small intestine).
* Iatrogenic Injury: The nerve is at risk during pelvic, retroperitoneal, or anterior hip surgeries. Retractor placement during anterior approaches to the hip or spine can cause severe neuropraxia.
* Hematoma Compression: Femoral neuropathies frequently result from retroperitoneal or iliopsoas hematomas. This is a classic complication in patients with hemophilia, those on aggressive anticoagulant therapy, or following blunt trauma.
* Pelvic Fractures: Branches of the femoral nerve may be contused, stretched, or lacerated by displaced bony fragments.
* Positional Ischemia: During prolonged operations in the prone position, inadequate padding can lead to excessive compression of the nerve against the inguinal ligament.
Clinical Examination
Diagnosis of a femoral nerve lesion requires a high index of suspicion.
* Motor Deficits: Atrophy of the anterior thigh muscles (quadriceps) becomes obvious in subacute or chronic settings. Surprisingly, active extension of the knee is rarely lost completely despite complete division of the femoral nerve. The patient can often stand and walk on level surfaces because the tensor fasciae latae, gracilis, and gluteus maximus provide compensatory stabilization of the limb. However, the patient will demonstrate profound weakness and buckling when attempting to go uphill, climb stairs, or rise from a seated position.
* Sensory Deficits: The autonomous zone of sensory supply is remarkably small, usually consisting of a localized area just superior and medial to the patella. The broader anterior aspect of the thigh and the saphenous nerve distribution typically show only varying degrees of hypesthesia due to overlapping dermatomal innervation.
* Diagnostics: High-resolution Magnetic Resonance Neurography (MRN) is excellent for identifying neuromas, transections, or compressing hematomas. Electromyography (EMG) and Nerve Conduction Studies (NCS) with needle electrodes inserted near the femoral nerve are invaluable for assessing the severity of the lesion, distinguishing between neuropraxia and neurotmesis, and tracking reinnervation.
OPERATIVE MANAGEMENT: APPROACH TO THE FEMORAL NERVE
Surgical exploration and repair of the femoral nerve are indicated for sharp transections, penetrating trauma with confirmed loss of continuity, or failure of clinical/EMG recovery after 3 to 6 months in closed injuries.
Preoperative Planning and Positioning
- Anesthesia: General anesthesia with complete muscle relaxation is required. Avoid long-acting paralytics if intraoperative nerve stimulation is planned.
- Positioning: The patient is placed supine on a radiolucent operating table. A small bump may be placed under the ipsilateral hemipelvis. The entire lower extremity, hemipelvis, and lower abdomen must be prepped and draped free to allow for acute hip flexion during nerve repair.
Surgical Technique (Extensile Retroperitoneal Approach)
This approach allows for proximal control of the nerve within the retroperitoneum and distal exposure into the femoral triangle.
- Incision: Begin the incision 5 cm proximal to the anterior superior iliac spine (ASIS). Direct it diagonally and distally toward the point where the femoral nerve passes beneath the inguinal ligament. This landmark is reliably 2.5 to 3 cm lateral to the palpable femoral artery pulse.
- Distal Extension: As the incision reaches the inguinal crease, direct it medially for about 2.5 cm to avoid crossing the skin flexion creases at a right angle (preventing future scar contracture). Continue the incision distally onto the anterior aspect of the thigh over the femoral triangle.
- Superficial Dissection: Proximal to the inguinal ligament, deepen the incision through the subcutaneous fat, Scarpa's fascia, and the aponeurosis of the external oblique muscle.
- Retroperitoneal Exposure: Carefully incise the internal oblique and transversus abdominis muscles. Open the transversalis fascia.
> Surgical Warning: Meticulously sweep the peritoneum medially using blunt dissection (sponge sticks or fingers) to expose the underlying iliac fascia. Violation of the peritoneum can lead to bowel injury or postoperative adhesions. - Nerve Identification: The femoral nerve can be palpated as a firm cord beneath the thick iliac fascia, lying in the groove between the psoas and iliacus muscles. Split the iliac fascia longitudinally along the course of the nerve.
- Proximal and Distal Mobilization: The nerve can now be exposed proximally to the point where it emerges from beneath the lateral edge of the psoas major muscle. Distally, trace it to the point where it passes beneath the inguinal ligament.
- Inguinal Ligament Release: If the lesion is at the level of the ligament, or if extensive mobilization is required, divide the inguinal ligament. This exposes the nerve as it enters the thigh and immediately arborizes into its motor and sensory branches.
NERVE REPAIR AND GAP MANAGEMENT
Methods of Closing Gaps
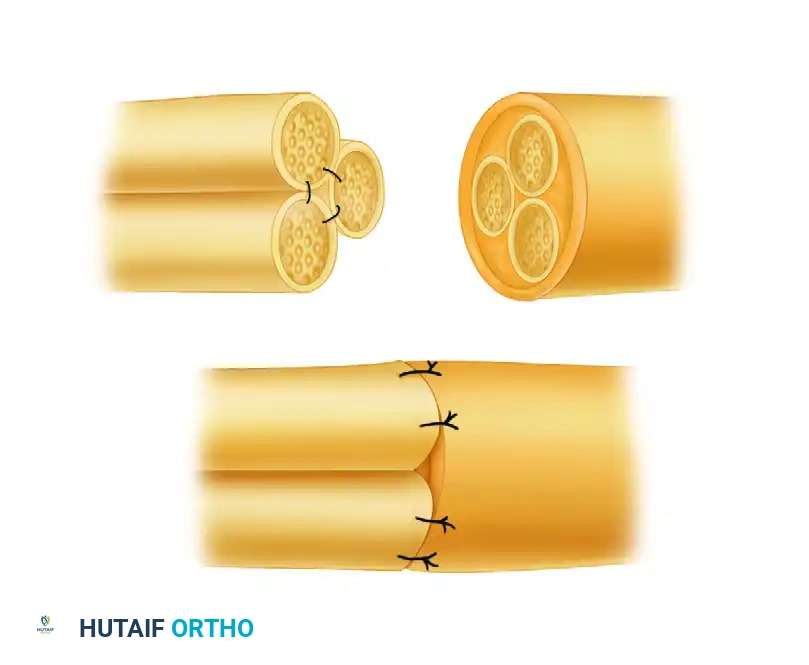
Primary end-to-end epineurial repair is the gold standard, provided it can be achieved without excessive tension. The femoral nerve possesses a unique capacity for mobilization, allowing for the closure of surprisingly large defects.
- Mobilization: Gaps of 8 to 10 cm can be closed without the need for nerve grafting. This is achieved by extensive proximal mobilization (freeing the nerve up to the lateral border of the psoas) and distal mobilization (carefully dissecting and freeing the individual branches of the nerve in the proximal thigh).
- Joint Positioning: The hip is flexed acutely (up to 90 degrees) to eliminate tension across the repair site.
- Neurorrhaphy: The nerve ends are prepared by resecting neuromas back to healthy fascicular tissue. An epineurial repair is performed using 8-0 or 9-0 non-absorbable monofilament sutures under operative magnification.
- Closure: The inguinal ligament must be meticulously reconstructed to prevent postoperative herniation. The abdominal wall is closed in layers (transversalis, internal oblique, external oblique aponeurosis) similar to any lower abdominal incision.
Grafting for Defects
If the gap exceeds 10 cm, or if primary repair requires excessive tension even with acute hip flexion, interfascicular nerve grafting is required. Sural nerve autografts are typically utilized. However, it must be noted that no significant, large-scale statistical information is currently available regarding the long-term functional outcomes of extensive grafting for massive defects in the femoral nerve.
Postoperative Protocol
- Immobilization: A custom hip spica cast or a rigid hinged hip orthosis locked in acute flexion is applied immediately in the operating room.
- Gradual Extension: The hip is maintained in acute flexion for 3 to 4 weeks to allow the epineurial repair to heal. Following this, the hip is gradually extended by 10 to 15 degrees per week.
- Rehabilitation: Once full extension is achieved (typically around 8 weeks postoperatively), aggressive physical therapy is initiated, focusing on quadriceps activation, gait training, and prevention of flexion contractures.
Results of Suture of the Femoral Nerve
Historically, there is a paucity of statistically significant, large-cohort data regarding the results of femoral nerve repair. However, clinical experience dictates that because the femoral nerve is a mixed nerve with a massive motor component supplying a single major muscle group (the quadriceps), targeted motor reinnervation is often more successful than in nerves with more complex, distal, and varied motor distributions (such as the sciatic or ulnar nerves). Early exploration, tension-free repair, and meticulous postoperative protection remain the cornerstones of optimizing functional recovery.
You Might Also Like