Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
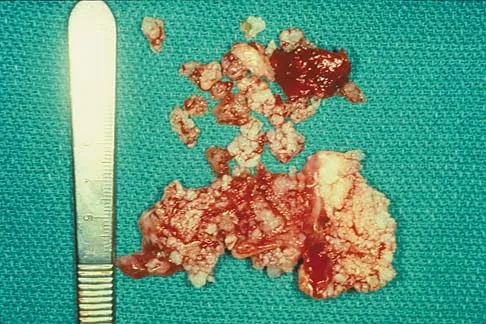
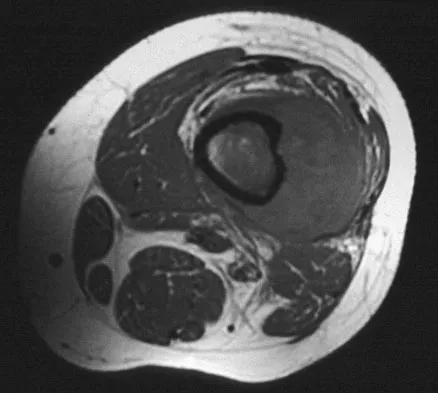
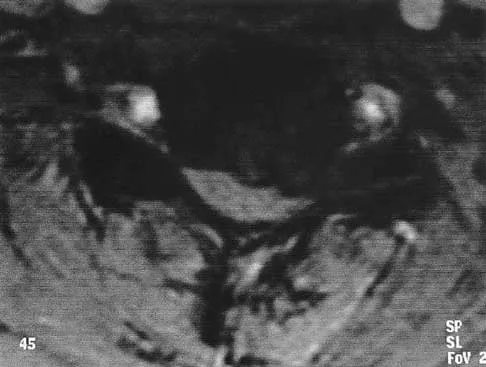
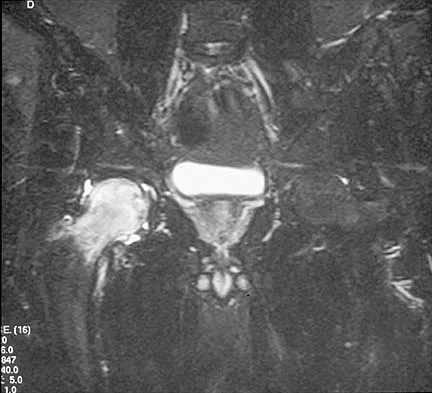
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of



Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 2
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?

Explanation
The clinical result in this patient has been good, with no dislocations, suggesting that the components are in reasonably good position. The radiograph and examination at the time of surgery suggest that the acetabular component is well fixed. The surrounding bone of the acetabulum is osteopenic and there would most likely be considerable bone loss if the acetabular component is removed. Access to the osteolytic lesions is possible. Cementing an acetabular component into the retained socket will cause the least amount of bone loss, shorten the procedure, and most likely result in a functional hip. Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Question 3
High Yield
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
In children, the main route of infection in skeletal TB is through hematogenous spread from a primary source. The mycobacterium is deposited in the end arterials in the vertebral body adjacent to the anterior aspect of the vertebral end plate. Thus, the anterior portion of the vertebral body is most commonly involved. The lower thoracic region is the most common segment; next in decreasing order of frequency are the lumbar, upper thoracic, cervical, and sacral regions. Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Question 4
High Yield
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 5
The parents of a 13-year-old boy with Down syndrome report that he has an increasing limp and decreased endurance with activities. Lateral flexion-extension radiographs of the cervical spine show no evidence of instability. Examination reveals a right Trendelenburg limp and an obvious limb-length discrepancy. Hip motion is symmetric except for some decreased abduction on the right side. A standing AP radiograph is shown in Figure 20. Management should consist of

Explanation
Ligamentous laxity and muscle hypotonia seen in Down syndrome contribute to the incidence of hip subluxation and dislocation. These factors can be progressive and lead to degenerative arthritis in adults with Down syndrome. Because this patient has a progressive limp and decreased endurance, observation and a shoe lift are not options. Bracing may be an option in the younger child before significant bony changes occur. Surgical intervention is the treatment of choice in this patient; however, all components of the deformity need to be addressed. Because of the increased capsular laxity, there is a high likelihood of recurrence if capsulorrhaphy is not included with the pelvic and femoral osteotomies. Surgery in these patients is associated with a high rate of complications. Shaw ED, Beals RK: The hip joint in Down's syndrome: A study of its structure and associated disease. Clin Orthop 1992;278:101-107. Aprin H, Zinc WP, Hall JE: Management of dislocation of the hip in Down's syndrome. J Pediatr Orthop 1985;5:428-431.
Question 6
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 7
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 8
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?

Explanation
Acetabular screws are inserted to supplement fixation. The acetabular component can be divided into four quadrants. Anatomic studies have shown that screws placed in the anterior superior and anterior inferior quadrants of the cup may injure the external iliac vein and obturator artery, respectively. Posterior superior and posterior inferior placement (in screws greater than 25 mm) may injure the sciatic nerve or the superior gluteal artery. The common iliac artery is proximal to the acetabulum and is at least risk for injury from acetabular screw placement.
Question 9
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
The radial nerve is only 4 mm from the anterolateral portal, while the median nerve is 11 mm away from the anteromedial portal. The ulnar nerve is only at risk on the medial side of the elbow. Anterior and posterior interosseous nerves are more distal within the forearm and are not in danger during portal placement. O'Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Question 10
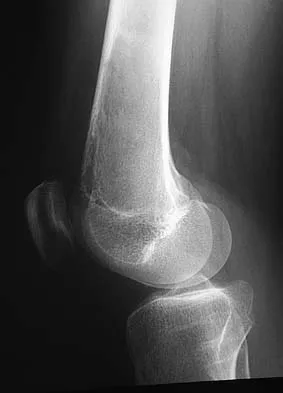
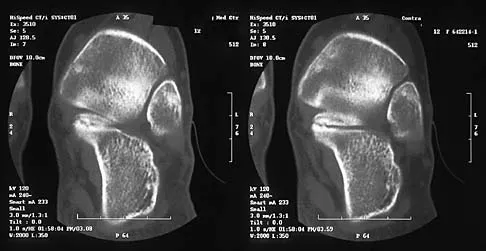
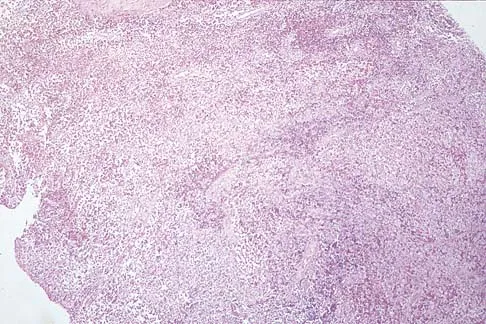
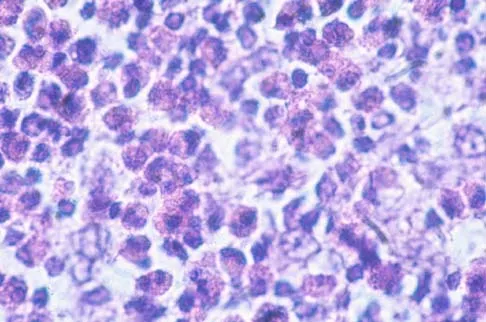
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?


Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 11
High Yield
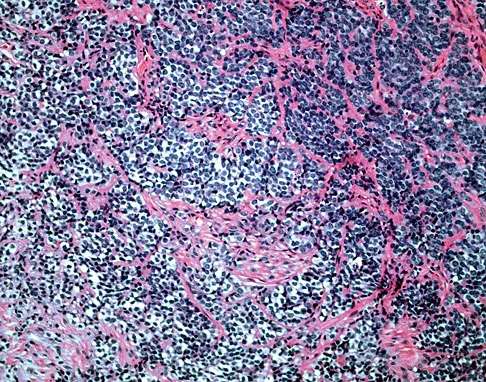
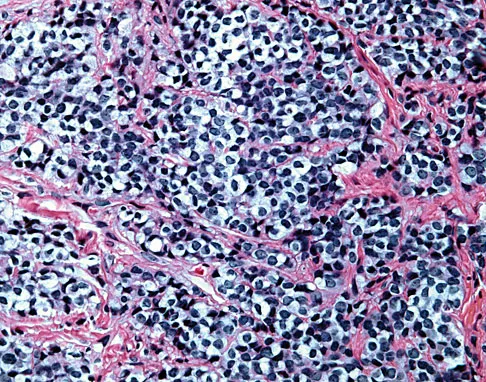
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?


Explanation
The imaging studies and histology are most consistent with Ewing's sarcoma. Tuberculosis can show small round blue cells on histology (lymphocytes associated with chronic infection) but would more typically involve the knee joint and periarticular bone. Osteosarcoma and MFH do not have small round blue cells histologically. Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Question 12
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of


Explanation
The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 13
The incidence of osteosarcoma is highest in what age group?

Explanation
The peak incidence of osteosarcoma occurs in the second decade, followed by the third decade. Up to 75% of all cases of osteosarcoma occur in patients between 10 and 25 years. It rarely occurs after age 30. Affected women tend to be younger than affect men. Osteosarcoma associated with Paget's disease or in radiation-induced osteosarcoma occurs in an older population. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Question 14
High Yield
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
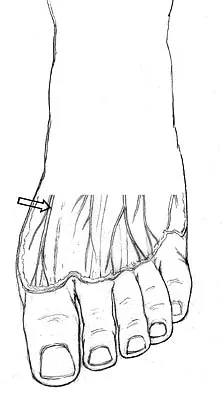
Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 15
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?

Explanation
Cadaver and clinical studies have shown that the sural nerve is at the highest risk for injury with a percutaneous repair of the Achilles tendon.
Question 16
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?

Explanation
The radiograph shows three zones: an outer regenerated cortical layer, an interface zone consisting of viable trabecular bone and occasional particles of bone cement, and an inner layer of necrotic bone embedded in cement. No fibrous membrane is noted, and there is no direct contact of cement with native bone. Based on these findings, it is believed that the middle layer is the result of incorporation of the allograft with further remodeling. Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Question 17
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?


Explanation
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 18
What is the preferred treatment of a patient with breast cancer and a pathologic fracture of the clavicle in her dominant arm?
Explanation
Closed management should be attempted for upper extremity pathologic fractures, particularly the clavicle. If nonunion or pain persists, surgery may be indicated. Radiofrequency ablation is not indicated for subcutaneous bones. Early motion is likely to cause increased pain and disability. Weber KC, Lewis VO, Randall RL, Lee AK, Springfield D: An approach to the management of the patient with metastatic bone disease. Instr Course Lect 2004;53:663-676.
Question 19
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?

Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 20
High Yield
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in

Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 21
High Yield
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?

Detailed Explanation
The incidence of injury associated with horseback rising is estimated to be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately 15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled at 6 months after injury as recreational riders. Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Question 22
High Yield
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
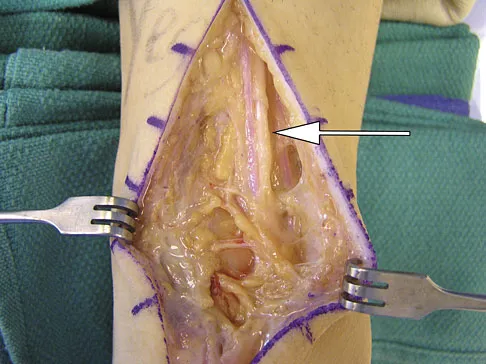
Explanation
The sural nerve runs with the small saphenous vein on the posterior leg just lateral to the Achilles tendon. It is formed by contributions from both the tibial and common peroneal nerves and provides sensation on the dorso-lateral aspect of the foot. Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Question 23
High Yield
With a full-thickness articular cartilage injury, the body's healing response produces cartilage mainly composed of what type of collagen?
Detailed Explanation
With a full-thickness articular cartilage injury, a healing response is initiated with hematoma, stem cell migration, and vascular ingrowth. This response produces type I collagen and resultant fibrous cartilage rather than desired hyaline cartilage as produced by chondrocytes. This repair cartilage has diminished resiliency, stiffness, poor wear characteristics, and the predilection for arthritis. Type I collagen is also found in the annulus of intervertebral disks, tendon, bone, meniscus, and skin. Type II is found in articular cartilage and nucleus pulposus of intervertebral disks. Type III is found in skin and blood vessels, type IV is found in basement membranes, and type X is found in the calcified layer of cartilage. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Question 24
High Yield
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Detailed Explanation
Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 25
Which of the following nerves travels with the deep palmar arch?

Explanation
The ulnar nerve divides alongside the pisiform, and the deep branch supplies the three hypothenar muscles and crosses the palm with the deep palmar arch to supply the two ulnar lumbricals, all interossei, and finally the adductor pollicis. The superficial branch supplies the ulnar digital branches to the small and ring fingers. The median nerve branches are more superficial in the palm near the superficial palmar arch. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 26
High Yield
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
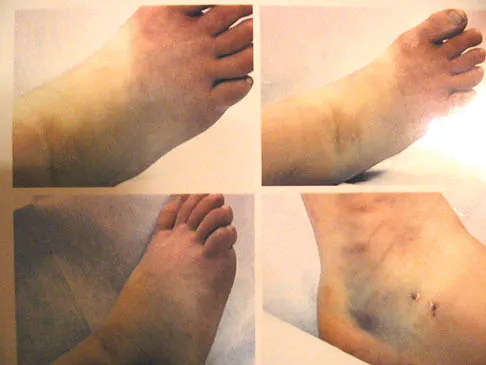
Explanation
The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast. Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Question 27
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
Question 28
High Yield
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?


Explanation
Osteolysis in the trochanteric bed can result in weakening of the bone and fracture. Nonsurgical management will provide reasonable clinical and radiographic results in patients with limited fracture displacement. Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Question 29
High Yield
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
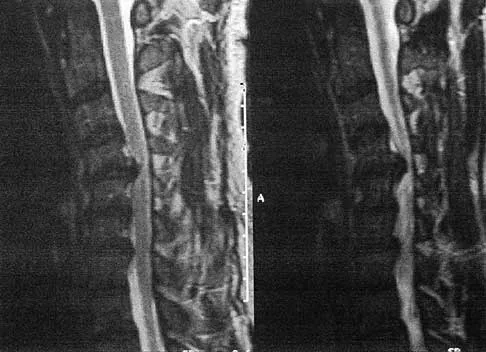
Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 30
High Yield
A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact. What is the most likely diagnosis?
Explanation
Traumatic mydriasis occurs from a contusion to the iris sphincter. This is a transient phenomenon during which the iris fails to constrict properly, resulting in a dilated pupil. More severe trauma can result in a tear of the sphincter and permanent pupillary deformity. In association with head injury, traumatic anisocoria would be a concerning indicator of the severity of injury. Retinal detachment, lens dislocation, corneal abrasion, and traumatic hyphema are all potential results of eye injury but are not reflected by this clinical description. Brucker AJ, Kozart DM, Nichols CW, Irving MR: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby Year Book, 1991, pp 650-670.
Question 31
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?



Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 32
High Yield
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Detailed Explanation
The superior gluteal artery is most at risk with a posterior iliac crest bone graft harvest. The artery leaves the pelvis through the sciatic notch and can be injured by retractors or other sharp instruments entering the sciatic notch area. The deep circumflex iliac, iliolumbar, and fourth lumbar arteries supply the iliacus and iliopsoas muscles and can be damaged during anterior bone graft harvest. The ascending branch of the lateral femoral circumflex artery is at risk during the anterior approach to the hip. Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Question 33
A 46-year-old patient with cervical myelopathy undergoes a multilevel posterior cervical laminectomy from C3 to C7. The risk of postlaminectomy kyphosis is greatest with removal of which of the following structures?
Explanation
Removal of more than 50% of a facet joint can lead to segmental instability and compromises the overall strength of the joint. Removal of the lamina, interspinous ligament, and ligamentum flavum are standard features of a cervical laminectomy. Most surgeons favor fusion with instrumentation of a laminectomized cervical spine. If the anterior part of the spine is already ankylosed from previous surgery or from degenerative conditions, or a posterior fusion with instrumentation is included, then the risk of kyphosis or instability is reduced.
Question 34
High Yield
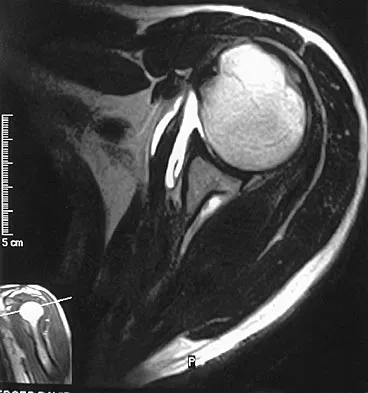
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of

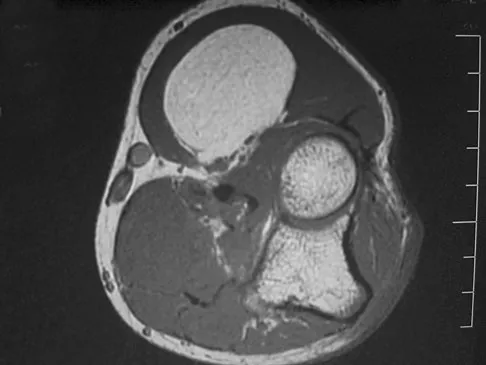
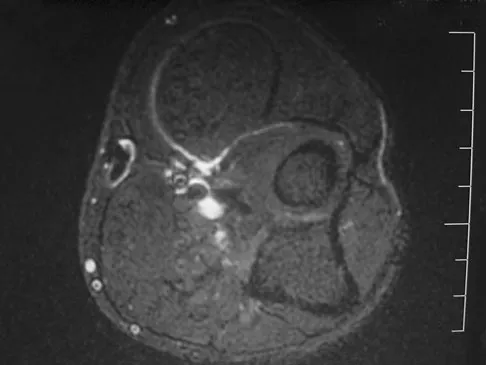
Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 35
Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?

Explanation
Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy. Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.
Question 36
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of


Explanation
The radiographs show a complex dislocation of the little finger metacarpophalangeal joint. This is characterized by obvious dislocation on the AP and lateral views and a type of bayonet apposition best visualized on the lateral view. Irreducibility of this injury is caused by displacement of the volar plate that has been traumatically avulsed from its origin on the metacarpal, with subsequent displacement into the metacarpophalangeal joint. This abnormal position of the volar plate causes irreducibility that can be corrected only by open reduction. This can be effected either by dorsal or palmar approaches. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Question 37
High Yield
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?

Detailed Explanation
A recent review of 200 consecutive distal radius fractures noted that the overall incidence of extensor pollicis longus rupture was 3%. The causes are believed to be mechanical irritation, attrition, and vascular impairment. The fracture is usually nondisplaced and the patient notes weeks to months after injury the sudden, painless inability to extend the thumb. Treatment involves extensor indicis proprius tendon transfer or free palmaris longus tendon grafting. Skoff HD: Postfracture extensor pollicis longus tenosynovitis and tendon rupture: A scientific study and personal series. Am J Orthop 2003;32:245-247. Bonatz E, Kramer TD, Masear VR: Rupture of the extensor pollicis longus tendon. Am J Orthop 1996;25:118-122.
Question 38
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of


Explanation
The patient has symptoms of synovitis that are most likely the result of the release of particles from the tibial polyethylene. While observation may be warranted in a completely asymtomatic knee, some intervention is indicated for this patient as there is clear radiographic evidence of lysis in both the tibia and femur. The decision about the extent of the revision should be made at the time of surgery. A limited incision technique is not indicated. Grafting (or using graft substitute) the defect is the most appropriate approach for treating the osteolytic lesions. While a posterior stabilized prosthesis might be the solution, surgical findings might dictate otherwise.
Question 39
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63. Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Question 40
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 41
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 42
High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 43
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a "pencil in cup" distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?

Explanation
The patient's clinical picture is considered the classic presentation for psoriatic arthritis. The other answers are not applicable for the constellation of findings. Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1691-1693.
Question 44
High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 45
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?




Explanation
Chondrosarcomas associated with diffuse bone lesions (enchondromas) are characteristic of Ollier's disease. When accompanied by subcutaneous masses (hemangiomas), the condition is called Maffucci's syndrome. Multiple hereditary exostosis is characterized by diffuse osteochondromas. McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia with cafe-au-lait spots and precocious puberty. Neurofibromatosis can have associated bone lesions but is not associated with chondrosarcomas. Sun TC, Swee TC: Chondrosarcoma in Maffucci's syndrome. J Bone Joint Surg Am 1985;67:1214-1219. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Question 46
High Yield
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of


Detailed Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 47
High Yield
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?


Explanation
The radiographs show a child with Legg-Calve-Perthes disease (LCPD) that has healed. Deformity (asphericity) of the femoral head is evident, but the femoral head and acetabulum are congruous. Stulberg and associates found that hips with aspherical congruity at skeletal maturity functioned well until the fifth or sixth decade of life. Similarly, another study found that degenerative arthritis caused deteriorating hip function after age 40 years in patients with this degree of residual deformity. Repeated episodes of ischemic necrosis are unlikely. Although some studies suggested coagulation abnormalities such as protein C and S deficiencies in children with LCPD, other studies failed to show any evidence of inherited thrombophila in most children with this disorder. There are no studies to suggest growth acceleration occurs following LCPD. Stulberg SD, Cooperman DR, Wallenstein R: The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:479-489.
Question 48
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of


Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 49
High Yield
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?

Explanation
The radiograph shows significant prevertebral soft-tissue swelling following a two-level anterior cervical diskectomy and fusion. The incidence of dysphagia 2 years after anterior cervical spine surgery is 13.6%. Risk factors for long-term dysphagia after anterior cervical spine surgery include gender, revision surgeries, and multilevel surgeries. The use of instrumentation, higher levels, or corpectomy versus diskectomy did not significantly increase the prevalence of dysphagia. Lee and associates demonstrated that while dysphagia after anterior cervical spine surgery is a common early finding, it generally decreases significantly by 6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia. Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Question 50
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?

Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 51
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 52
High Yield
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Detailed Explanation
Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended. Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394. Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Question 53
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be


Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 54
The cavovarus deformity associated with Charcot-Marie-Tooth (CMT) disease is caused by which of the following?
Explanation
The most common inherited neuromuscular disease seen by orthopaedic surgeons is CMT, which is an inherited autosomal-dominant disease. It is more commonly seen in men due to the nature of the inheritance. Identification of cavus deformity in the foot of a child should arouse suspicion. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-143. Charcot-Marie-Tooth Disease (CMT) Penn State Hershey Medical Center. www.hmc.psu.edu/healthinfo/c/cmt.htm
Question 55
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?

Explanation
The presence of synchronous bone disease in young patients carries a dismal prognosis, one that is even worse than the presence of resectable pulmonary metastasis. Many osteosarcomas cross the physis; therefore, this has not been shown to be of prognostic importance. Similarly, the presence of the soft-tissue mass has less prognostic significance.
Question 56
High Yield
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?

Explanation
Although cervical instability is a contraindication to posterior decompression alone, segmental instability in the myelopathic cervical spine can be addressed with concomitant posterior fusion with instrumentation. Cervical lordosis represents the ideal scenario for posterior decompressive procedures for myelopathy (laminectomy and laminoplasty) because compression from anterior osteophytes, if present, is relieved as the spinal cord migrates posteriorly. The anteroposterior diameter of the spinal canal does not have an impact on the selection of surgical approach. Posterior unroofing-type procedures in kyphotic cervical spines, however, are ineffective because anterior impingement on the spinal cord will remain; therefore, kyphosis of more than 10 degrees is considered a contraindication for posterior decompression. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 57
A 22-year-old man has mild hip pain bilaterally and multiple skeletal lesions. Based on the pelvic radiograph shown in Figure 30, what is the inheritance pattern for his disorder?

Explanation
Multiple hereditary exostoses (MHE) is an autosomal dominant disorder manifested by multiple osteochondromas and characteristic skeletal involvement. EXT1 on 8q24.1 and EXT2 on 11p13 are the two genes most strongly associated with MHE. Mutations in these genes affect proper development of endochondral bone, such that in all affected individuals exostoses develop adjacent to the growth plates of long bones, and some exhibit additional bone deformities. Defects in the EXT genes result in increased chondrocyte proliferation and delayed hypertrophic differentiation. Stieber JR, Dormans JP: Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 2005;13:110-120.
Question 58
High Yield
Ganglion cysts about the wrist most commonly arise from what structure?
Detailed Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 59
High Yield
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of

Explanation
Fractures in this area of the fifth metatarsal have a high incidence of delayed union, nonunion, and recurrence with nonsurgical management. In an acute fracture, prolonged casting in a non-weight-bearing cast may allow for healing; however, in the presence of prolonged symptoms, recurrent fracture, and intermedullary sclerosis, surgical treatment is preferred. Surgery most commonly consists of intermedullary fixation or medullary curettage and bone grafting, followed by application of a non-weight-bearing cast. Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Question 60
High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 61
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Sudden cardiac arrest following a blow to the chest in young athletes has been termed "commotio cordis." It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate. Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Question 62
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 63
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?

Explanation
The distal oblique shortening (Weil) metatarsal osteotomy has not been associated with transfer lesions to the extent of other shortening osteotomies, and malunions and nonunions are unusual complications. Recurrent dorsal contracture of the toe has been reported. Recommendations to reduce this problem include release of the dorsal capsule and tendons, as well as a flexor tendon transfer. A potential cause suspected for this phenomenon is the relatively dorsal positioning of the intrinsic tendons after plantar displacement of the metatarsal head. Trnka HJ, Nyska M, Parks BG, Myerson MS: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50. Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 64
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 65
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?



Explanation
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint. Renoult B, Lataste A, Jonon B, et al: Sternoclavicular joint infection in hemodialysis patients. Nephron 1990;56:212-213.
Question 66
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?


Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 67
High Yield
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
Nonsurgical management is considered for proximal tears as well as partial tears in some individuals. Surgical management is often not appropriate in older or sedentary patients. However, patients treated nonsurgically will have a significant cosmetic defect, as well as weakness in adduction and internal rotation. Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Question 68
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of


Explanation
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Question 69
High Yield
In displaced calcaneal fractures, what fragment is the only one that remains in its anatomic position?
Explanation
The sustentaculum tali remains in its anatomic position because of its supporting ligamentous structures. This provides the key to the reconstruction of the calcaneus. The posterior facet is reduced to the sustentaculum tali and then fixed to it for stability. All of the other components of the calcaneus are then reduced to this complex. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250. Eastwood DM, Gregg PJ, Atkins RM: Intra-articular fractures of the calcaneum: Part I. Pathological anatomy and classification. J Bone Joint Surg Br 1993;75:183-188.
Question 70
High Yield
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of

Detailed Explanation
Dislocation of the long head of the biceps tendon is the result of a defect in the region of the rotator cuff interval, coracohumeral ligament-superior glenohumeral ligament pulley, or an associated tear of the medial insertion of the subscapularis tendon. In the case of an intra-articular dislocation of the long head of the biceps tendon associated with a tear of the subscapularis tendon, stabilization of the biceps tendon is difficult in this situation; therefore, biceps release or tenodesis and repair of the subscapularis tendon is the treatment of choice. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Question 71
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 72
High Yield
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?


Explanation
The diagnosis is eosinophilic granuloma. The plain radiograph and MRI scan show a lesion in the midshaft of the femur. There is no soft-tissue mass. There is reactive bone about the lesion that suggests a less aggressive tumor. The histology reveals eosinophils in an otherwise bland cellular background with no evidence of mitotic figures or malignant cells to suggest sarcoma. The diagnostic elements are the amphophilic (ie, pale purple) histiocytes with cigar-shaped nuclei, some of which have linear longitudinal grooves. There is no histologic evidence of infection. Lymphoma of bone would be an unusual occurrence in this age group, and the histology is not consistent with that diagnosis.
Question 73
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 74
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?

Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 75
A Trendelenburg gait is most likely to be seen in association with

Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 76
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of

Explanation
The MRI scan shows a massive tear of the supraspinatus tendon with medial retraction to the level of the glenoid. This is most likely an attritional tear with a high risk of failure of the repair. The preferred treatment is nonsurgical management for pain and stiffness. Acromioplasty and coracoacromial ligament release in this setting are controversial, as they can result in the devastating complication of anterosuperior subluxation of the humerus. Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Question 77
High Yield
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of


Detailed Explanation
The patient has symptoms of synovitis that are most likely the result of the release of particles from the tibial polyethylene. While observation may be warranted in a completely asymtomatic knee, some intervention is indicated for this patient as there is clear radiographic evidence of lysis in both the tibia and femur. The decision about the extent of the revision should be made at the time of surgery. A limited incision technique is not indicated. Grafting (or using graft substitute) the defect is the most appropriate approach for treating the osteolytic lesions. While a posterior stabilized prosthesis might be the solution, surgical findings might dictate otherwise.
Question 78
High Yield
What are the five most common tumors that metastasize to bone?
Detailed Explanation
The five most common primary carcinomas that metastasize to bone are breast, prostate, lung, renal, and thyroid in decreasing order of incidence. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 79
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
The mutation of the retinoblastoma gene has been associated with an increased prevalence of osteosarcoma. The mutation resulting in EWS-FLI1 is associated with Ewing's sarcoma. The other mutations are associated with tumor formation and proliferation but not necessarily with osteosarcoma formation. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4. Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Question 80
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component. Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348. Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491. Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Question 81
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?




Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 82
High Yield
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of


Detailed Explanation
The complications of femoral neck fractures in children include osteonecrosis, malunion, nonunion, and premature physeal closure. It is presumed that the risk of osteonecrosis is directly related to the amount of displacement at the time of injury and is not affected by the type of treatment. The risk of the other complications can be decreased depending on the type of treatment. Anatomic reduction by either closed or open methods can reduce the risk of malunion. The addition of internal fixation allows for maintenance of the reduction. In young children who cannot comply with a partial or non-weight-bearing status, the addition of a spica cast gives added protection. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 83
High Yield
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?


Explanation
Transient osteoporosis is a self-limited painful but reversible disorder. Although first described in pregnant women, it is more common in young to middle-aged men. The radiograph shows loss of mineralization in the right hip relative to the left side. There is no osseous destruction or cortical expansion typical of metastasis or giant cell tumor. The process is confined to the femoral side of the joint unlike rheumatoid arthritis, which would be centered in the joint. Osteonecrosis is better defined with sharp but irregularly shaped margins, and there is no double-line sign. The MRI scans reveal diffuse edema in the femoral head and neck that is atypical for osteonecrosis. Transient osteoporosis may recur in the same or opposite hip.
Question 84
High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Detailed Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 85
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?


Explanation
This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear. Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573. Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 86
High Yield
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?



Detailed Explanation
A discoid meniscus is a large disk-like meniscus. It is seen in the lateral meniscus in 3% of the population; a discoid medial meniscus is much less common. It can be identified on the coronal view by noting meniscal tissue extending into the tibial spine at the intercondylar notch. The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 87
High Yield
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of


Detailed Explanation
Fractures of the long bones are common in patients with myelodysplasia, and the frequency of fracture increases with higher level defects. Fractures also occur following surgery and immobilization secondary to disuse osteoporosis. The response to the fracture (swelling, fever, warmth, erythema) is often confused with infection, osteomyelitis, or cellulitis. Management should consist of a short period of immobilization in a well-padded splint. Long-term casting results in further osteopenia and repeated fractures. Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Question 88
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80 degrees. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62 degrees. One year later, the mean gain was 33 degrees. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
Question 89
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?

Explanation
The patient has a failed Silastic implant. Nonsurgical management will not work at this point. A Keller resection will only exacerbate her metatarsalgia. Implant removal with structural bone grafting and MTP fusion is the most appropriate choice because restoration of length is needed to alleviate the forefoot pain and bone grafting is required to fuse the MTP joint because there is an abundance of osteolysis. Total toe implants do not offer good long-term outcomes and are very difficult to fit into the large exploded-out cavity of the proximal phalanx. Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Question 90
High Yield
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?


Explanation
The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically. Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Question 91
High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?

Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 92
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 93
High Yield
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?


Explanation
The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided. Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg 1997;6:544-548.
Question 94
High Yield
What is the single most important nutritional factor affecting athletic performance?
Explanation
Maintenance of adequate hydration is the single most important factor affecting athletic performance. While carbohydrate loading may be beneficial for some endurance athletes, the consumption of carbohydrates during exercise does not appear to be beneficial for athletes engaged in events that last less than 1 hour. In general, athletes consuming a balanced diet do not need electrolyte supplementation. Maughan RJ, Noakes TD: Fluid replacement and exercise stress: A brief review of studies on fluid replacement and some guidelines for the athlete. Sports Med 1991;12:16-31.
Question 95
High Yield
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength. Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172 Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Question 96
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?

Explanation
Most lesions of eosinophilic granuloma are simply observed, but larger aggressive lesions may require curettage and bone grafting. Frequently, biopsy is required to rule out a malignant diagnosis. The differential diagnosis of eosinophilic granuloma is osteomyelitis, Ewing's sarcoma of bone, or osteogenic sarcoma. The biopsy alone can be followed by spontaneous resolution. In some patients, low-dose radiation therapy is used. Chemotherapy or amputation is not indicated for these benign lesions.
Question 97
High Yield
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?

Detailed Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 98
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 99
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?

Explanation
Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player's first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season. Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Question 100
High Yield
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Explanation
Distant bone metastasis is associated with an extremely poor prognosis for patients with osteosarcoma (5-year survival rate of less than 10%). Most osteosarcomas are high grade and extracompartmental, and approximately half are greater than 8 cm at presentation. The 5-year survival rate for these patients is approximately 70%. Patients with a solitary pulmonary metastasis have a prognosis worse than patients without detectable metastases but not as bad as those with bone metastases. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790. Heck RK, Stacy GS, Flaherty MJ, et al: A comparison study of staging systems for bone sarcomas. Clin Orthop Relat Res 2003;415:64-71.
