Single-Stage Great Toe-to-Thumb Transfer: Comprehensive Surgical Guide
Key Takeaway
The single-stage great toe-to-thumb transfer is a highly complex microsurgical procedure designed to restore opposition, pinch, and grasp following traumatic thumb amputation. This comprehensive guide details the dual-team surgical approach, encompassing precise donor site dissection, recipient bed preparation, peg-in-hole osteosynthesis, and intricate microvascular anastomoses. Strict adherence to biomechanical tendon balancing, utilizing May’s reconstruction scheme, ensures optimal functional recovery and aesthetic restoration of the thumb ray.
INTRODUCTION TO THUMB RECONSTRUCTION
The thumb contributes approximately 40% to 50% of overall hand function, serving as the critical post for opposition, key pinch, and power grasp. Traumatic amputation of the thumb results in profound functional impairment. While various reconstructive options exist—including pollicization, osteoplastic reconstruction, and distraction lengthening—the single-stage great toe-to-thumb transfer remains the gold standard for restoring length, sensation, aesthetic appearance, and dynamic function in cases of amputation at or proximal to the metacarpophalangeal (MCP) joint.
This highly demanding microsurgical procedure requires meticulous preoperative planning, a thorough understanding of both pedal and manual neurovascular anatomy, and precise execution of osteosynthesis, tenorrhaphy, and microvascular anastomosis.
Clinical Pearl: The success of a great toe transfer relies heavily on a dual-team approach. Simultaneous dissection of the donor foot and recipient hand minimizes total ischemia time and significantly reduces operative fatigue.
INDICATIONS AND PATIENT SELECTION
Patient selection is paramount. The procedure is technically demanding and requires a compliant patient capable of adhering to strict postoperative rehabilitation protocols.
Primary Indications
- Traumatic thumb amputations at or proximal to the MCP joint.
- Congenital absence or severe hypoplasia of the thumb (e.g., severe radial longitudinal deficiency).
- Failed prior thumb reconstructions requiring salvage.
Contraindications
- Absolute: Severe peripheral vascular disease, active infection at either the donor or recipient site, lack of suitable recipient vessels, or profound medical comorbidities precluding prolonged anesthesia.
- Relative: Advanced age, heavy tobacco use (smoking must be strictly ceased at least 6 weeks preoperatively), and severe psychiatric conditions or non-compliance.
PREOPERATIVE PLANNING AND VASCULAR ANATOMY
Thorough preoperative vascular assessment is mandatory. The arterial supply to the great toe exhibits significant anatomical variance, primarily concerning the first dorsal metatarsal artery (FDMA).
- Doppler Ultrasound & Angiography: Essential to map the dorsalis pedis artery, the FDMA, and the plantar arterial arch. The surgeon must confirm that harvesting the great toe will not compromise the vascularity of the remaining foot.
- Gilbert Classification of the FDMA:
- Type I: The FDMA arises superficial to the dorsal interosseous fascia (most favorable for dissection).
- Type II: The FDMA runs intramuscularly within the first dorsal interosseous muscle.
- Type III: The FDMA is absent or hypoplastic, and the dominant supply is derived from the plantar metatarsal artery (requires a more complex plantar dissection).
SURGICAL TECHNIQUE: PHASE 1 - DONOR FOOT DISSECTION
The objective of the foot dissection is to harvest the great toe with adequate bony length, a robust vascular pedicle, sufficient tendon length, and intact digital nerves, while minimizing donor site morbidity.
Incision and Exposure
- Design a racquet-shaped incision around the base of the great toe. The dorsal extension should follow the course of the dorsalis pedis artery and the FDMA.
- Make a transverse incision in the middle or proximal portion of the plantar surface of the foot. This separate incision is critical to obtain adequate length of the flexor hallucis longus (FHL) tendon.
Tendon and Nerve Harvest
- Extensor Tendons: Identify and section the extensor hallucis longus (EHL) tendon near the extensor retinaculum or more proximally through the same dorsal incision used for vessel dissection.
- Flexor Tendons: Dissect bluntly through the plantar incision to locate the FHL tendon.
Surgical Warning: The FHL must be carefully separated from its connections to the flexor digitorum longus (FDL) tendons (the Master Knot of Henry). These tendinous interconnections make it extremely difficult and dangerous to attempt releasing the FHL blindly through an ankle incision.
- Nerves: Identify and mobilize the plantar digital nerves. Obtain as much length as possible, depending on the requirements of the recipient thumb area. Occasionally, interpositional nerve grafts (e.g., sural nerve) may be required if the recipient bed has extensive nerve loss.
Osteotomy and Joint Management
- Separate the toe at the metatarsophalangeal (MTP) joint.
- If the reconstructive plan requires a new MCP joint in the hand, the MTP joint capsule must be harvested en bloc with the toe.
- Bone Resection: The plantar aspect of the first metatarsal head should be preserved to maintain weight-bearing mechanics in the foot. However, the dorsal portion of the first metatarsal may be taken with the toe by performing an oblique osteotomy from the dorsal surface proximally to the plantar surface distally.
Pedicle Isolation
- Dissect the dorsalis pedis artery, FDMA, and the accompanying venae comitantes or superficial dorsal veins.
- CRITICAL STEP: Leave the vascular pedicle attached to the foot until the hand dissection has been completed and the recipient bed is fully prepared. This ensures continuous perfusion and minimizes ischemia time.
Donor Site Closure
- Once the hand team is ready, ligate the pedicle, release the tourniquet, and achieve meticulous hemostasis in the foot.
- Fashion the skin flaps to allow side-to-side closure of the foot incision. Leave only small areas, if any, for split-thickness skin grafting.
- Close the foot incisions over small, thin closed-suction drains if needed.
- Apply a bulky, nonconstricting compression bandage to the foot.
SURGICAL TECHNIQUE: PHASE 2 - RECIPIENT HAND DISSECTION
Simultaneous preparation of the hand is performed by the second microsurgical team. The goal is to isolate healthy recipient vessels, nerves, and tendons outside the zone of injury.
Incisions and Exposure
- Two primary incisions are usually required.
- Dorsal Incision: Outline a curved dorsal incision near the anatomical snuffbox, extending to the tip of the bony remnant of the amputated thumb.
- Palmar Incision: Make a palmar incision parallel to the thenar crease, extending proximally over the carpal tunnel and obliquely across the wrist flexion crease into the distal forearm.
- Exsanguinate the limb by elevation or with an elastic wrap, and inflate the pneumatic tourniquet.
Dorsal Dissection
- Elevate full-thickness skin flaps to expose the thumb metacarpal or phalangeal remnant.
- Identify and mobilize the tendons of the extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and abductor pollicis longus (APL).
- Carefully isolate the cephalic vein and its tributaries to serve as venous recipients.
- Identify the radial artery and its distal first metacarpal (princeps pollicis) extension.
- Isolate the superficial radial nerve and its terminal branches for sensory coaptation.
Palmar Dissection
- Through the thenar/carpal tunnel incision, identify and expose the stumps of the palmar digital nerves to the thumb.
- Isolate the flexor pollicis longus (FPL) tendon.
- Identify the adductor pollicis (ADD) and abductor pollicis brevis (AbPB) tendons if they are available and viable.
- Isolate the palmar digital arteries if they are suitable for microvascular anastomosis (though the dorsal radial system is more commonly used).
- Deflate the tourniquet and achieve satisfactory hemostasis. The remainder of the procedure may be done without the tourniquet, or it can be used intermittently to minimize blood loss during osteosynthesis.
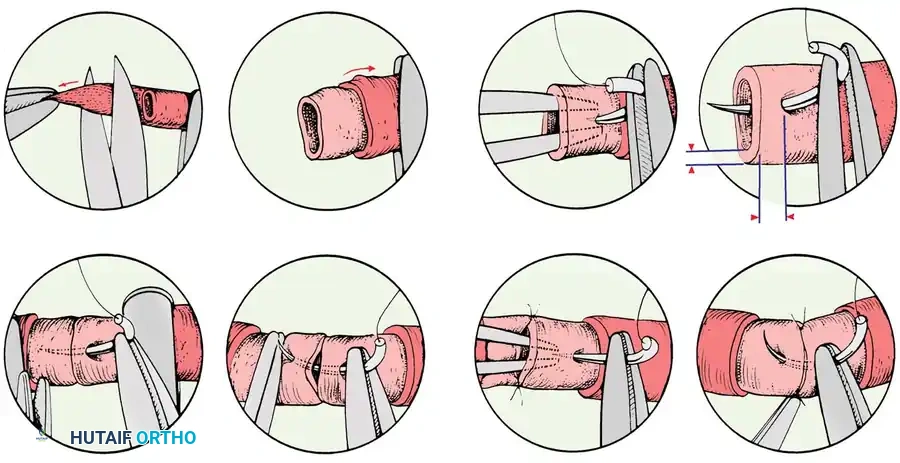
SURGICAL TECHNIQUE: PHASE 3 - TRANSFER AND OSTEOSYNTHESIS
Once the toe is amputated and transferred to the hand, rigid skeletal fixation is the immediate priority to provide a stable foundation for subsequent microsurgery.
- Bony Apposition: Achieve stable bony apposition using a "peg-in-hole" (cup-and-cone) technique. Make a hollow recess in the base of the proximal phalanx of the transferred toe.
- Remodel the recipient thumb metacarpal or phalangeal remnant to form a peg, and insert it into the recess in the toe phalanx.
- Fixation: Supplement this construct with internal fixation. Crossed Kirschner wires (K-wires) or intraosseous wiring are standard, though miniature plates and screws can be utilized depending on bone quality and surgeon preference. Ensure proper pronation and palmar abduction of the new thumb to optimize opposition.
SURGICAL TECHNIQUE: PHASE 4 - TENDON RECONSTRUCTION AND BALANCING
Restoring dynamic balance is one of the most challenging aspects of the procedure. The intrinsic and extrinsic forces must be meticulously balanced to prevent clawing or deviation of the transferred digit.
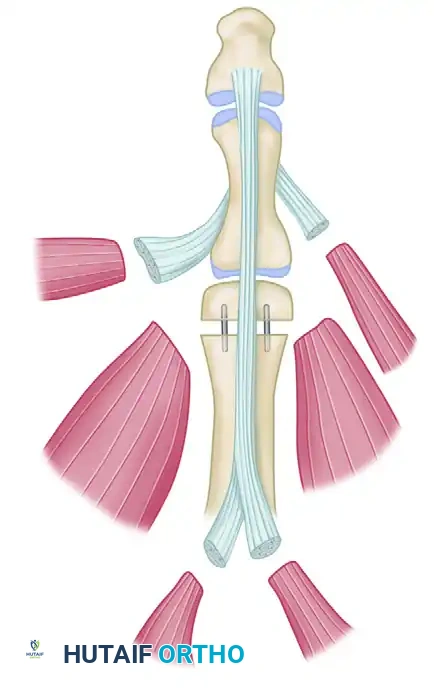
May et al. suggested a highly effective scheme for the reconstruction of available tendon attachments to replicate native thumb biomechanics.
FIGURE 63-62: Transfer of great toe to thumb. Scheme suggested by May for reconstruction of available tendon attachments. AbH, abductor hallucis; AbPB, abductor pollicis brevis; ADD, adductor hallucis; EHB, extensor hallucis brevis; EHL, extensor hallucis longus; EPB, extensor pollicis brevis; EPL, extensor pollicis longus; FHL, flexor hallucis longus; FPL, flexor pollicis longus.
Extensor and Abductor Mechanism Repair
- EPL to EHL: The recipient Extensor Pollicis Longus is woven into the donor Extensor Hallucis Longus to restore primary IP joint extension.
- EPB to EHB: The recipient Extensor Pollicis Brevis is sutured to the donor Extensor Hallucis Brevis to restore MCP joint extension.
- AbPB to AbH: The recipient Abductor Pollicis Brevis is attached to the donor Abductor Hallucis to restore palmar abduction and assist in opposition.
Flexor and Adductor Mechanism Repair
- FPL to FHL: The recipient Flexor Pollicis Longus is repaired to the donor Flexor Hallucis Longus. This is typically performed in the distal forearm using a Pulvertaft weave to ensure a strong repair capable of early active mobilization. Tensioning is critical; the thumb should rest in slight flexion when the wrist is in neutral.
- ADD to ADD: The recipient Adductor Pollicis is sutured to the donor Adductor Hallucis to restore powerful key pinch.
Pitfall: Over-tensioning the extensor mechanism relative to the flexor mechanism will result in a hyperextended, non-functional interphalangeal joint. Tendon tension must be assessed by passively ranging the wrist (tenodesis effect) prior to final suturing.
SURGICAL TECHNIQUE: PHASE 5 - MICROVASCULAR ANASTOMOSIS AND NEURORRHAPHY
With the skeleton stabilized and tendons repaired, the microscope is brought into the field for neurovascular reconstruction.
Arterial Anastomosis
- Ensure satisfactory pulsatile flow through the recipient radial arterial branches.
- Perform an end-to-end or end-to-side anastomosis between the donor dorsalis pedis artery (or FDMA) and the recipient first metacarpal artery or the main radial artery in the anatomical snuffbox. Use 9-0 or 10-0 nylon sutures.
- Release the micro-clamps and confirm immediate perfusion of the transferred toe (brisk capillary refill, pink color).
Venous Anastomosis
- Perform at least two, preferably three, venous anastomoses to ensure adequate outflow and prevent venous congestion.
- Anastomose the dorsal superficial veins of the toe to the cephalic vein and its tributaries using 10-0 nylon.
Neurorrhaphy
- Perform epineurial repairs of the nerves using 9-0 or 10-0 nylon under high magnification.
- Coapt the plantar digital nerves of the toe to the palmar digital nerves of the thumb.
- Coapt the dorsal sensory branches of the superficial peroneal nerve (from the toe) to the terminal branches of the superficial radial nerve.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative phase is as critical as the surgical execution. The patient is transferred to a specialized microsurgical intensive care or step-down unit.
Medical Management
- Anticoagulation: Begin continuous intravenous infusion of low-molecular-weight dextran or heparin immediately after the arterial anastomosis has been completed, depending on institutional preference and surgeon protocol. This is typically maintained for 3 to 5 days.
- Environment: Keep the patient's room warm to prevent vasospasm. Hydration must be strictly maintained.
- Monitoring: Flap checks (color, capillary refill, temperature, and tissue turgor) are performed every hour for the first 48 hours, then every 2 hours. Implantable venous Doppler probes may be utilized for continuous monitoring.
Rehabilitation Timeline
- Weeks 0-3: The hand is immobilized in a bulky, non-compressive splint. No active motion is permitted.
- Weeks 3-4: K-wires are typically removed if clinical and radiographic signs of early union are present. Gentle active range of motion (AROM) of the IP and MCP joints is initiated under the strict guidance of a certified hand therapist.
- Weeks 6-8: Passive range of motion (PROM) and gentle strengthening exercises begin.
- Months 3-6: Progressive pinch and grip strengthening. Sensory re-education begins as Tinel's sign advances distally.
COMPLICATIONS AND MANAGEMENT
- Vascular Thrombosis: The most devastating complication. Arterial insufficiency presents as a pale, cool digit with absent capillary refill. Venous congestion presents as a swollen, purple digit with rapid, dark capillary refill. Both require immediate return to the operating room for exploration and thrombectomy.
- Donor Site Morbidity: Delayed wound healing, hyperkeratosis under the first metatarsal head, and altered gait mechanics. Preserving the plantar aspect of the first metatarsal head significantly mitigates gait disturbances.
- Nonunion: Rare, but may occur at the osteosynthesis site, requiring secondary bone grafting and revision fixation.
- Tendon Adhesions: Common, particularly with the flexor mechanism. Tenolysis may be required 6 to 12 months postoperatively if rehabilitation plateaus.
The single-stage great toe-to-thumb transfer represents the pinnacle of reconstructive hand surgery. Through meticulous adherence to anatomical principles, precise microsurgical technique, and rigorous postoperative care, surgeons can restore profound function and quality of life to patients suffering from devastating thumb amputations.
You Might Also Like