Acad Orthop Surg Challenge: Diagnose Shoulder Pain Case 1
Key Takeaway
Looking for accurate information on Acad Orthop Surg Challenge: Diagnose Shoulder Pain Case 1? A partial-thickness rotator cuff tear is common in older patients, presenting with insidious, diffuse deltoid pain, night pain, and exacerbated by overhead activities. Patients typically maintain full or nearly full active range of motion, experiencing pain but not significant weakness with resisted shoulder flexion, a key differentiator discussed in **acad orthop surg**.
Detailed Patient Presentation and Mechanism of Injury
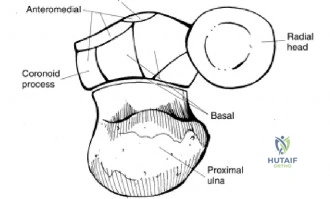
The presentation of insidious, progressive shoulder pain in the geriatric population is a ubiquitous challenge in orthopedic clinical practice, requiring a highly nuanced understanding of glenohumeral biomechanics and degenerative pathophysiology. In this classic grand rounds case, we evaluate a 76-year-old right-hand-dominant male who presents with chronic right shoulder pain that has progressively worsened over several months. The patient localizes the pain diffusely over the lateral aspect of the deltoid region, a pathognomonic sign of referred pain originating from the subacromial space and rotator cuff footprint. Unlike acute traumatic injuries, this patient’s history lacks a distinct inciting event, pointing toward an intrinsic degenerative etiology compounded by chronic microtrauma.
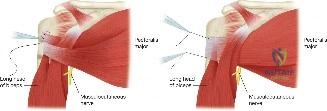
The hallmark symptom reported by this patient is night pain, particularly when rolling onto the affected shoulder. Night pain is a critical clinical indicator of rotator cuff pathology and subacromial bursitis. It is thought to occur due to the loss of gravity-assisted inferior traction on the humerus when supine, allowing the humeral head to migrate slightly superiorly and compress the inflamed bursa and rotator cuff against the rigid coracoacromial arch. Furthermore, the patient reports significant pain with overhead activities. Overhead kinematics require the coordinated force couple of the deltoid and the rotator cuff; as the arm elevates above 90 degrees, the supraspinatus must dynamically depress the humeral head. In the presence of a rotator cuff lesion, this mechanism becomes painful and inefficient, leading to secondary impingement and the classic "painful arc" of motion.

Understanding the mechanism of injury in this demographic requires a deep dive into the intrinsic and extrinsic theories of rotator cuff disease. Extrinsically, as described by Neer, the cuff is subjected to mechanical abrasion against the anterior undersurface of the acromion, the coracoacromial ligament, and the AC joint. Intrinsically, normal aging brings about diminished vascularity—particularly in the critical zone of the supraspinatus tendon, located approximately 1 cm proximal to its insertion on the greater tuberosity. This relative hypovascularity, combined with age-related changes in collagen composition (a shift from Type I to weaker Type III collagen) and tenocyte apoptosis, predisposes the tendon to failure under physiologic loads.

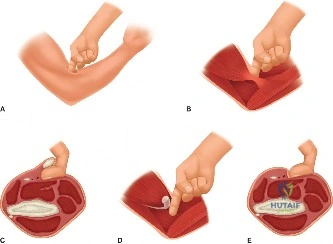
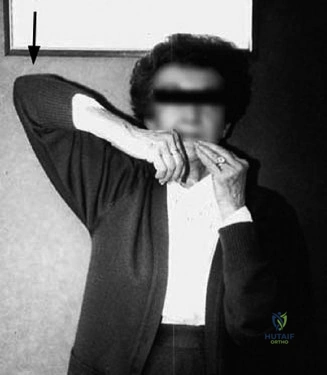
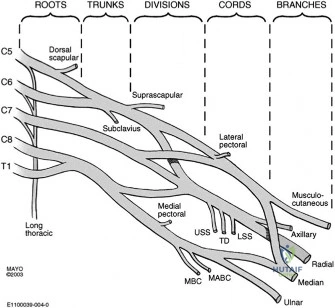
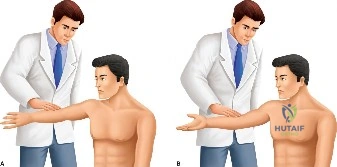
In this 76-year-old patient, the combination of these intrinsic and extrinsic factors has culminated in a symptomatic lesion. It is imperative to recognize that the diffuse nature of the pain—often radiating down the lateral arm but rarely past the elbow—is mediated by the C5 dermatome and the shared innervation of the shoulder joint by the suprascapular and axillary nerves. When a patient uses their entire hand to grasp the deltoid to indicate the location of their pain, rather than pointing with a single finger, the astute clinician should immediately place rotator cuff pathology at the top of the differential diagnosis.

Comprehensive Clinical Examination Findings
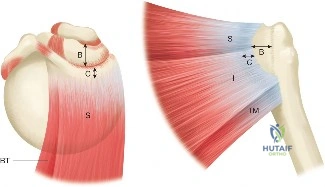
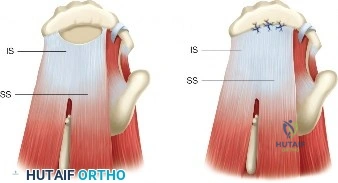
The physical examination of the shoulder is a masterclass in differentiating structural failure from inflammatory or degenerative pain. Upon visual inspection of this patient, there is a notable absence of muscle atrophy in the supraspinatus and infraspinatus fossae. This is a critical negative finding. In chronic, massive, full-thickness rotator cuff tears, the lack of mechanical tension on the muscle belly leads to rapid disuse atrophy and fatty infiltration (Goutallier changes), which manifest clinically as prominent scapular spines and hollowed fossae. The preserved muscle bulk in this patient strongly suggests that the biomechanical continuity of the rotator cuff is at least partially intact, maintaining resting muscle tension.
Range of motion (ROM) testing further delineates the extent of the pathology. The patient demonstrates full passive range of motion, which effectively eliminates adhesive capsulitis (frozen shoulder) from the differential. Adhesive capsulitis is characterized by a global, multi-planar restriction in both active and passive ROM due to profound capsular fibroplasia and contracture, particularly in external rotation with the arm at the side. Furthermore, the patient has near-full active range of motion. The ability to actively elevate the arm without significant kinematic substitution (e.g., shoulder shrugging) indicates that the rotator cable—the thick, fibrous bundle described by Burkhart that spans the rotator crescent—remains structurally competent to transmit forces and stabilize the glenohumeral joint.
Strength testing and provocative maneuvers isolate the specific tendinous deficits. The patient experiences pain and mild, pain-inhibited weakness with resisted forward flexion and abduction (Jobe's or Empty Can test). True mechanical weakness (pseudoparalysis) is typically indicative of a massive full-thickness tear where the force couples are completely uncoupled. In contrast, the weakness observed here is secondary to pain inhibition (algogenic paresis). When the supraspinatus is loaded, tension across the partially torn fibers stimulates mechanoreceptors and nociceptors, causing a reflex inhibition of motor output.

Additional provocative testing would likely reveal positive impingement signs. Neer's test (passive forward elevation in internal rotation) and the Hawkins-Kennedy test (internal rotation of the shoulder elevated to 90 degrees in the scapular plane) forcibly compress the greater tuberosity against the coracoacromial arch, eliciting sharp pain. However, tests for the subscapularis (Lift-off, Belly Press) and the infraspinatus/teres minor (External Rotation Lag Sign, Hornblower's sign) would likely remain negative or demonstrate normal strength, localizing the primary pathology to the superior cuff, specifically the supraspinatus tendon.

Advanced Imaging and Diagnostics
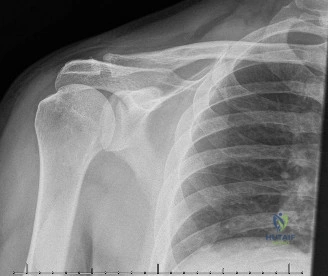
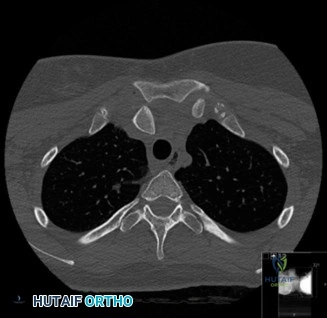
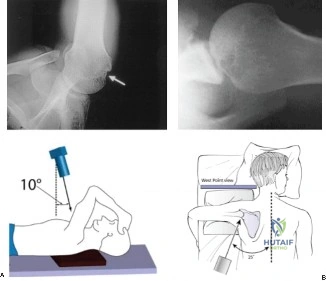
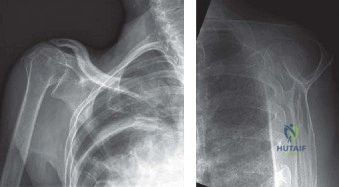
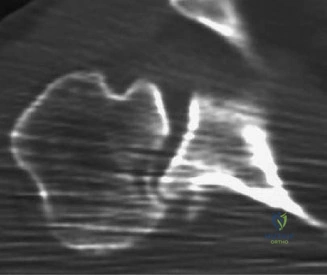
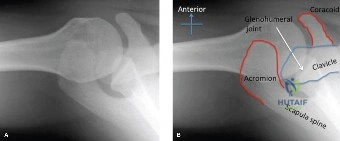
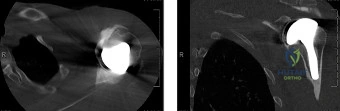
While the clinical examination provides a robust working diagnosis, advanced imaging is paramount for surgical templating, prognosticating, and definitively ruling out concomitant intra-articular or osseous pathology. The initial imaging modality must always be a high-quality, orthogonal radiographic series of the shoulder, including a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. In a 76-year-old with a partial-thickness rotator cuff tear, radiographs may appear surprisingly benign.
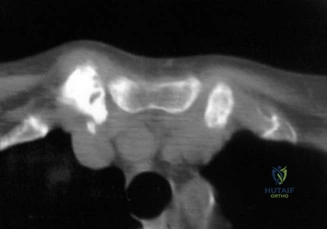
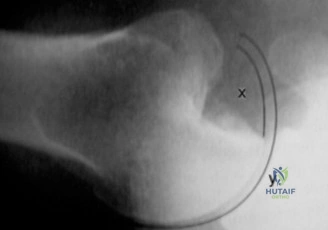
However, subtle radiographic clues often hint at the underlying pathology. The Grashey view is scrutinized for the acromiohumeral interval (AHI). A normal AHI is between 7 and 14 mm. An AHI of less than 7 mm is highly indicative of a massive, chronic full-thickness rotator cuff tear allowing superior migration of the humeral head due to the unopposed upward pull of the deltoid. In our patient with a partial tear, the AHI will likely be preserved, as the intact portion of the cuff continues to depress the humeral head. We also evaluate the greater tuberosity for sclerosis, cortical irregularity, or cystic changes—the so-called "footprint cysts" that develop secondary to chronic micro-avulsions and hypervascularity at the tendon insertion.

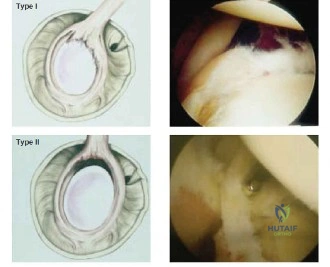
The scapular Y view and supraspinatus outlet view are essential for evaluating acromial morphology. Bigliani classified acromial shapes into three types: Type I (flat), Type II (curved), and Type III (hooked). A Type III hooked acromion significantly decreases the subacromial volume and is highly correlated with an increased incidence of rotator cuff tears, acting as a relentless mechanical abrading force against the bursal surface of the supraspinatus tendon. Additionally, the axillary view helps assess for glenohumeral osteoarthritis and ensures the humeral head is concentrically reduced, ruling out chronic subtle dislocations.
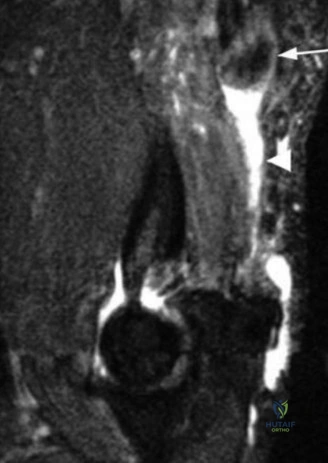
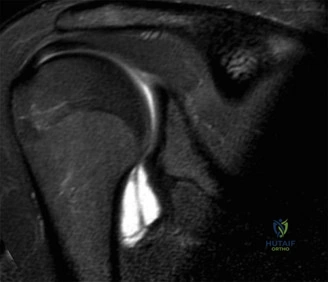
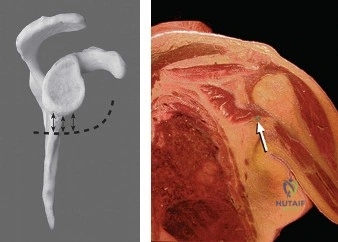
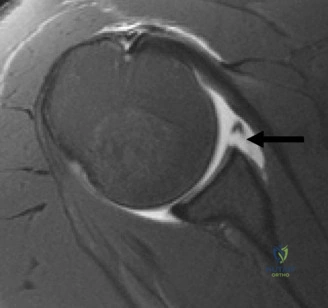
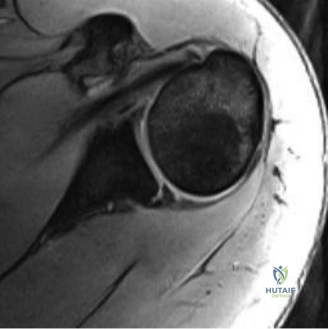
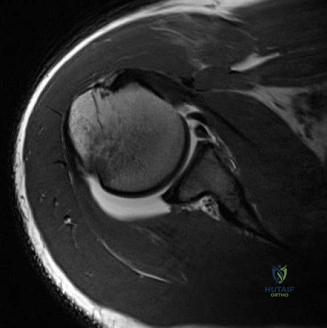
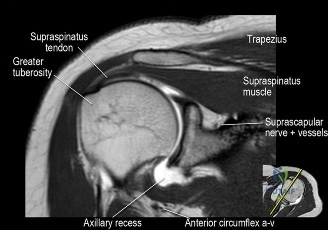
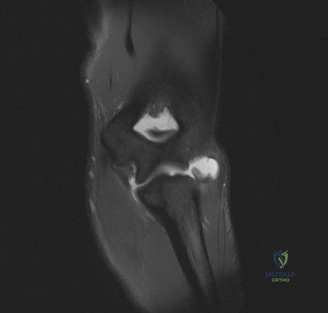
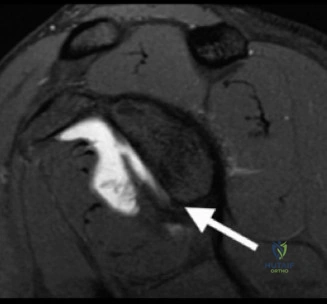
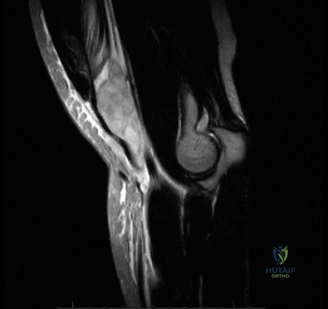
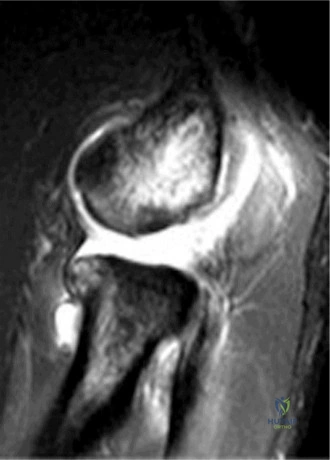
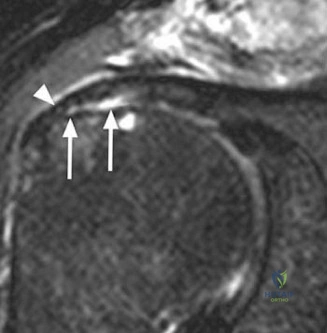
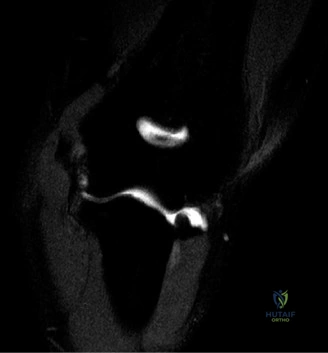
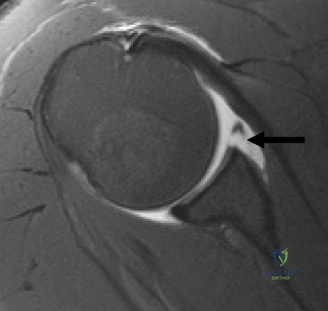
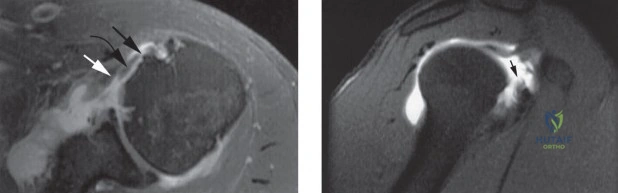
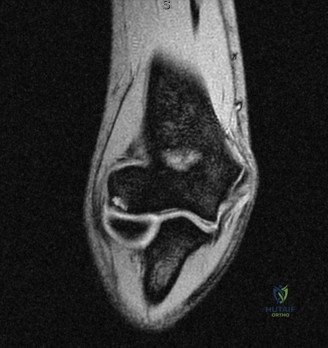
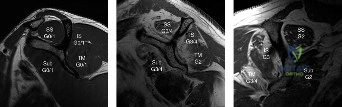
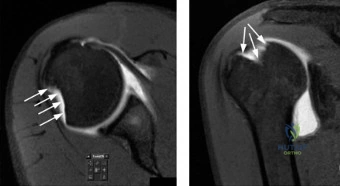
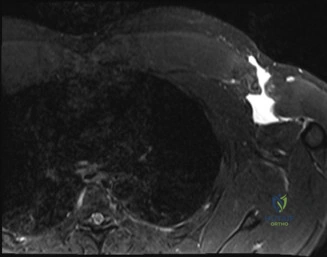
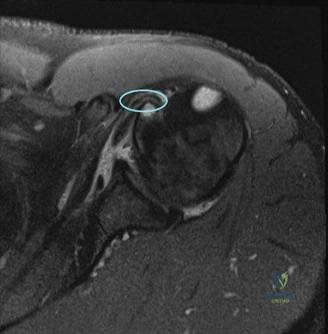
Magnetic Resonance Imaging (MRI), particularly without contrast or as an MR Arthrogram (MRA), remains the gold standard for evaluating the soft tissue envelope of the shoulder. For partial-thickness tears, MRI provides exquisite detail regarding the location (articular-sided, bursal-sided, or interstitial) and the depth of the tear. A T2-weighted coronal oblique sequence will typically demonstrate a focal region of hyperintensity extending partially through the tendon substance. Articular-sided partial tears (PASTA lesions - Partial Articular Sided Tendon Avulsions) are the most common and are best visualized on MRA, where the gadolinium contrast will imbibe into the articular defect, sharply outlining the extent of the avulsion from the footprint.

Exhaustive Differential Diagnosis
The differential diagnosis for insidious onset shoulder pain in a septuagenarian is broad, but careful clinical correlation allows the orthopedic surgeon to systematically eliminate competing pathologies. The primary differentials include Partial-Thickness Rotator Cuff Tear (PTRCT), Full-Thickness Rotator Cuff Tear (FTRCT), Acromioclavicular (AC) Joint Arthritis, Adhesive Capsulitis, and Glenohumeral Labral Pathology. Cervical radiculopathy must also be considered, as C5 nerve root compression can masquerade as lateral shoulder pain.
AC joint arthritis is exceptionally common in this age group but presents distinctly differently from rotator cuff pathology. Patients with AC arthrosis will localize their pain precisely to the superior aspect of the shoulder, often pointing directly to the joint with a single finger (the "one-finger sign"). The pain is exacerbated by cross-body adduction (Scarf test) and direct palpation over the joint line. In contrast, our patient exhibits the "deltoid sign," utilizing the entire hand to cup the lateral shoulder, which is characteristic of subacromial pathology.

Adhesive capsulitis, or frozen shoulder, is characterized by a profound, multi-planar loss of both active and passive range of motion. The capsule undergoes intense fibroblastic proliferation and contracture, particularly in the rotator interval and the coracohumeral ligament. A patient with adhesive capsulitis will have a firm, mechanical block to passive external rotation. Our patient’s preservation of full passive range of motion definitively excludes this diagnosis. Similarly, while a glenohumeral labral tear (such as a SLAP lesion) can cause pain, it typically presents with a history of acute trauma (e.g., a traction injury or fall on an outstretched hand) and is accompanied by mechanical symptoms such as clicking, catching, or popping, which are absent in this case.

Differentiating a partial-thickness tear from a full-thickness tear relies heavily on the physical examination. A full-thickness tear often presents with profound weakness that is not merely pain-inhibited, visible atrophy of the spinatus fossae, and potentially a loss of active elevation despite preserved passive motion (pseudoparalysis). The structural continuity provided by the remaining intact fibers in a partial tear preserves the force couples necessary for active elevation, aligning perfectly with our patient's presentation.

Differential Diagnosis Matrix
| Pathology | Primary Pain Location | Active ROM | Passive ROM | Key Physical Exam Findings | Imaging Hallmarks |
|---|---|---|---|---|---|
| Partial-Thickness RCT | Diffuse lateral deltoid | Near full, painful arc | Full | Pain with resisted abduction; positive impingement signs | T2 hyperintensity not traversing full tendon thickness |
| Full-Thickness RCT | Diffuse lateral deltoid | Decreased (pseudoparalysis) | Full | True weakness; visible atrophy; positive drop arm test | Fluid signal traversing entire tendon; superior humeral migration |
| AC Joint Arthritis | Focal superior shoulder | Full | Full | Point tenderness at AC joint; positive cross-body adduction | AC joint space narrowing, osteophytes, subchondral sclerosis |
| Adhesive Capsulitis | Diffuse, deep joint pain | Severely restricted | Severely restricted | Firm block to passive external rotation | Thickened joint capsule, loss of axillary recess volume |
| Cervical Radiculopathy (C5) | Neck radiating to shoulder | Full | Full | Positive Spurling's test; altered dermatomal sensation | Foraminal stenosis at C4-C5 on cervical MRI |

Complex Surgical Decision Making and Classifications
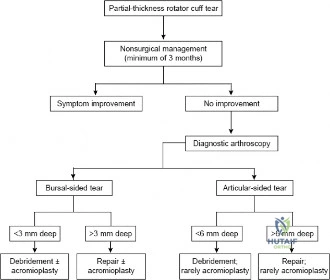
The management of a partial-thickness rotator cuff tear in a 76-year-old patient requires a delicate balance between symptom relief, functional demand, and the inherent risks of surgical intervention in the elderly. The initial approach is invariably non-operative, consisting of a structured physical therapy program focused on periscapular stabilization, rotator cuff strengthening, and postural correction. This is often augmented by subacromial corticosteroid injections to modulate the localized inflammatory response and provide a window of pain relief to facilitate rehabilitation. However, if the patient fails to progress after 3 to 6 months of dedicated conservative management, surgical intervention becomes a highly viable consideration.

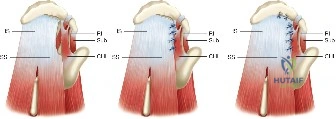
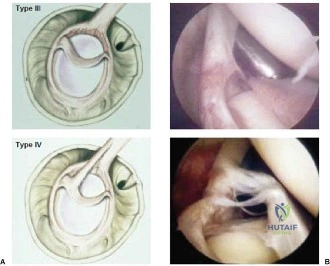
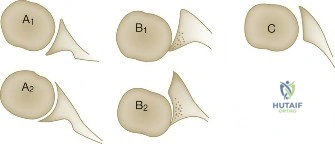
When templating for surgery, the orthopedic surgeon relies heavily on the Ellman Classification of partial-thickness rotator cuff tears. Ellman categorizes tears based on their location (A = Articular, B = Bursal, C = Interstitial) and their depth relative to the normal tendon thickness (which is approximately 10-12 mm at the footprint). Grade I tears involve less than 3 mm of depth (<25% of tendon thickness). Grade II tears involve 3 to 6 mm of depth (25-50% of tendon thickness). Grade III tears involve greater than 6 mm of depth (>50% of tendon thickness). This classification is not merely academic; it drives the intraoperative decision-making algorithm.

The general consensus in orthopedic sports medicine and shoulder surgery is the "50% Rule." For Ellman Grade I and Grade II tears (less than 50% thickness), surgical treatment typically consists of arthroscopic debridement of the frayed tendon edges to a stable margin, combined with a subacromial decompression and acromioplasty to eliminate the extrinsic mechanical impingement. The intact portion of the tendon is deemed biomechanically sufficient to maintain function.

Conversely, for Ellman Grade III tears (greater than 50% thickness), the remaining tendon is considered biomechanically compromised and at high risk for progression to a full-thickness tear. In these scenarios, the surgeon must decide between two primary repair techniques: an in situ transtendon repair or a formal takedown and repair. A takedown involves completing the tear to a full-thickness defect and repairing it using standard techniques. While this provides excellent visualization, it sacrifices the remaining intact, healthy tendon fibers. The in situ repair preserves the intact bursal or articular fibers, theoretically maintaining the native biomechanical length-tension relationship, but is technically more demanding.

Step-by-Step Surgical Technique and Intervention
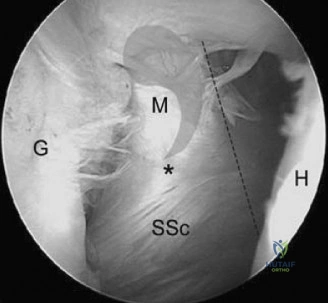
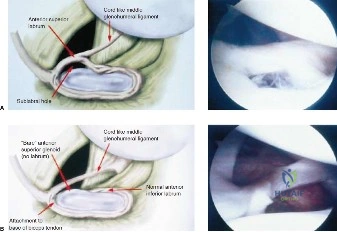
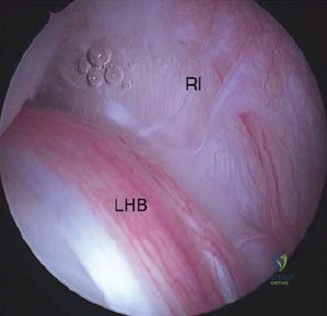
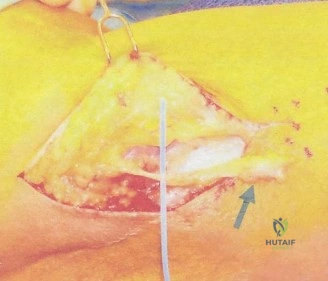
Should this patient proceed to operative intervention for a high-grade articular-sided partial tear (PASTA lesion), the procedure is performed entirely arthroscopically. The patient is positioned in either the beach chair or lateral decubitus position, depending on surgeon preference. A standard posterior viewing portal is established, and a thorough 15-point diagnostic arthroscopy of the glenohumeral joint is performed. The articular surface of the supraspinatus is meticulously inspected. The partial tear will appear as a region of avulsed, frayed tendon fibers lifted off the medial aspect of the greater tuberosity footprint.
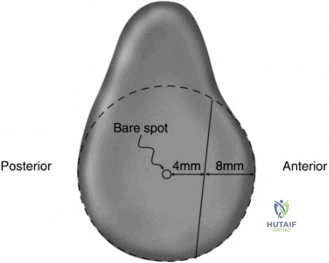
To accurately gauge the depth of the tear, a calibrated probe is used. If the tear is deemed to involve greater than 50% of the footprint (typically exposing more than 6-7 mm of bare bone medial to lateral), a repair is indicated. The footprint is first debrided using a motorized shaver and an arthroscopic radiofrequency wand to remove degenerative tissue and expose a bleeding cancellous bone bed, which is critical for optimal tendon-to-bone healing.

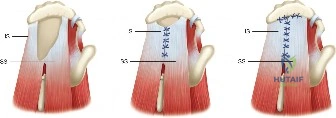
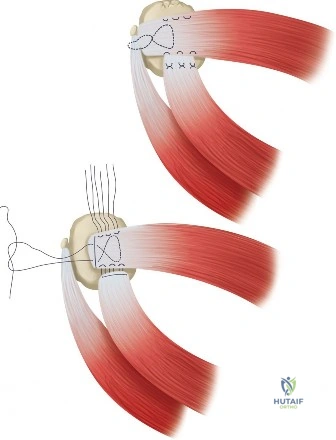
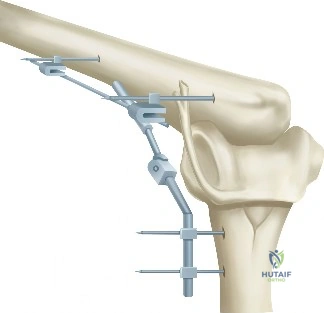
For an in situ transtendon repair, a spinal needle is introduced percutaneously from the lateral aspect of the shoulder, passing through the intact bursal layer of the supraspinatus tendon and exiting through the articular defect. This establishes the trajectory for anchor placement. A small stab incision is made in the intact tendon, and a bio-composite or PEEK suture anchor (typically 4.5 mm to 5.5 mm) is advanced through the tendon and impacted or screwed into the prepared bony footprint at the articular margin.

Once the anchor is seated, the sutures must be passed through the torn articular leaflet of the tendon. This is achieved using a specialized suture-passing device (e.g., a Scorpion or penetrating grasper). The sutures are passed in a mattress configuration to maximize tissue capture and compression. The scope is then transitioned to the subacromial space. A thorough bursectomy is performed to optimize visualization. If a Type III acromion is present, an acromioplasty is executed using a high-speed burr to create a flat, non-impinging coracoacromial arch. Finally, the sutures that were passed through the tendon are retrieved in the subacromial space and tied using arthroscopic sliding knots (e.g., SMC or Weston knot) followed by alternating half-hitches, effectively compressing the articular-sided tear down to the bony footprint while preserving the intact bursal fibers.

Strict Post-Operative Protocol and Rehabilitation Stages
The success of a rotator cuff repair, whether partial or full-thickness, is inextricably linked to strict adherence to a phased postoperative rehabilitation protocol. The biological timeline for tendon-to-bone healing dictates the pace of recovery; premature stress can lead to catastrophic failure of the repair, while excessive immobilization can result in profound postoperative stiffness.
Phase I: Maximal Protection (Weeks 0 to 6)
Immediately postoperatively, the patient is placed in an abduction sling to remove tension from the superior cuff repair. The primary goal during this phase is the protection of the surgical construct while preventing adhesive capsulitis. Therapy is strictly limited to passive range of motion (PROM). The therapist will perform passive forward elevation in the scapular plane and gentle external rotation with the arm resting safely at the side. Active motion of the elbow, wrist, and hand is encouraged to prevent distal edema and stiffness. No active motion of the shoulder is permitted, as the firing of the supraspinatus muscle belly would exert pull on the newly placed anchors.

Phase II: Active-Assisted to Active Motion (Weeks 6 to 12)
At the 6-week mark, biological healing has progressed sufficiently to withstand mild tensile loads. The sling is discontinued. The patient transitions from PROM to active-assisted range of motion (AAROM) using pulleys, wand exercises, and wall walks. By week 8, true active range of motion (AROM) is initiated. The focus is on re-establishing normal scapulothoracic kinematics and preventing compensatory shoulder shrugging. Isometrics for the deltoid and periscapular musculature are introduced, but resisted rotator cuff exercises remain contraindicated.
Phase III: Early Strengthening (Weeks 12 to 16)
By 12 weeks, the tendon-to-bone interface has matured into a more robust fibrocartilaginous integration. Progressive resistive exercises (PREs) are initiated. Strengthening begins with closed-chain exercises and low-resistance elastic bands, focusing on the internal and external rotators below shoulder level. Scapular stabilizers (rhomboids, serratus anterior, trapezius) are heavily targeted to ensure a stable base of support for the glenohumeral joint.

Phase IV: Advanced Strengthening and Return to Activity (Weeks 16+)
In the final phase, exercises transition to functional, open-chain movements, gradually incorporating overhead activities. Plyometrics and sport-specific or work-specific dynamic stabilization drills are introduced. For a 76-year-old patient, the goal is a return to pain-free activities of daily living, recreational golf or swimming, and comfortable sleep. Maximum medical improvement is typically reached between 6 and 12 months postoperatively.

High-Yield Clinical Pearls and Pitfalls
Mastering the diagnosis and management of shoulder pain in the elderly requires a synthesis of clinical acumen, radiographic interpretation, and surgical precision. There are several high-yield pearls and dangerous pitfalls that every orthopedic surgeon must internalize when approaching a case like this.
Pearl: The Value of the "Deltoid Sign"
Never underestimate the patient's own localization of pain. Referred pain to the lateral deltoid insertion is the hallmark of subacromial pathology. The suprascapular nerve, which innervates the supraspinatus and infraspinatus, shares nerve root origins (C5, C6) with the axillary nerve, which supplies the deltoid and the overlying skin. This neuroanatomical crossover is why rotator cuff tears rarely present with pain directly over the tendon itself, but rather further down the arm.

Pitfall: Misdiagnosing Cervical Radiculopathy
A classic pitfall is failing to evaluate the cervical spine in a patient presenting with shoulder pain. C5 radiculopathy can mimic rotator cuff pathology almost perfectly, presenting with lateral shoulder pain and weakness in abduction. Always perform a thorough neurologic exam, including a Spurling's maneuver and reflex testing. If the pain radiates past the elbow into the hand, or is accompanied by paresthesias, the cervical spine must be investigated with MRI.
Pearl: Differentiating Weakness from Pain Inhibition
When a patient exhibits weakness during a Jobe's test, the surgeon must differentiate between true structural failure (pseudoparalysis) and pain inhibition. A diagnostic subacromial injection of 1% lidocaine (the Neer Impingement Test) is an invaluable tool. If the patient's strength normalizes after the injection eliminates the pain, the weakness was secondary to pain inhibition, strongly suggesting a partial tear or tendinopathy rather than a massive full-thickness tear.

Pitfall: Over-treating Asymptomatic Tears
In the geriatric population, MRI findings must be correlated strictly with clinical symptoms. Literature has repeatedly demonstrated that up to 50% of patients over the age of 70 have asymptomatic rotator cuff tears. Operating on an MRI finding rather than the patient is a profound error. If a 76-year-old has a partial tear on MRI but minimal pain and good function, conservative management is not just an option; it is the standard of care.

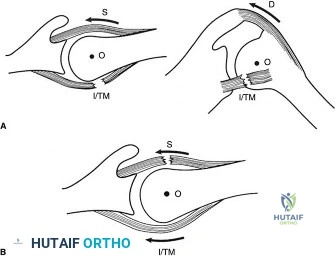
Pearl: The Biomechanics of the Rotator Cable
Understanding Burkhart's suspension bridge model of the rotator cuff is essential. The rotator cable is a thick bundle of fibers running perpendicular to the supraspinatus and infraspinatus tendons, shielding the thinner, avascular rotator crescent. Many partial tears, and even some full-thickness tears, involve only the crescent while the cable remains intact. This explains why patients like the one in this case can maintain near-full active kinematics despite a structural defect.





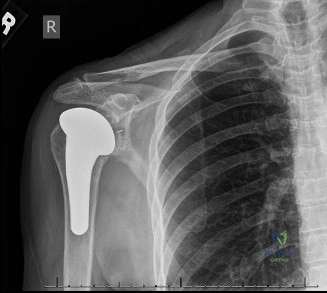
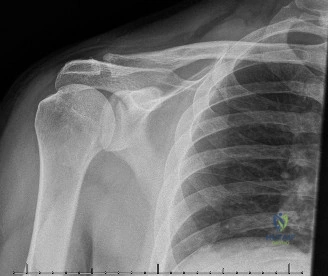
Clinical & Radiographic Imaging Archive