Scapula Fractures: Your Guide to Recognizing and Treating Scapula Injuries
Key Takeaway
This topic focuses on Scapula Fractures: Your Guide to Recognizing and Treating Scapula Injuries, Scapula fractures involve the triangular scapula bone, a relatively uncommon injury representing 0.4-1% of all fractures. These fractures typically result from high-energy trauma, such as motor vehicle accidents or direct blows. Given the significant protective muscle mass surrounding the scapula, a scapula fracture often indicates severe associated injuries, necessitating a thorough trauma evaluation for comorbidities like rib or spine fractures.
Introduction and Epidemiology
Scapular fractures, while infrequent, represent a significant injury, typically indicative of high-energy trauma. This relatively uncommon injury accounts for approximately 3% to 5% of all shoulder girdle fractures and 0.4% to 1% of all fractures encountered in orthopedic practice. The mean age of patients sustaining a scapular fracture generally falls within the 35 to 45-year demographic, often aligning with populations engaged in activities associated with high-impact mechanisms. The unique anatomical position and robust muscular envelope of the scapula provide substantial protection, meaning that when a fracture does occur, substantial force has been exerted, necessitating a meticulous assessment for associated injuries.
The recognition and appropriate management of scapular fractures are critical, as delayed diagnosis or inadequate treatment can lead to chronic pain, shoulder dysfunction, and significant long-term morbidity. The historical perception of scapular fractures as benign, often managed non-operatively, has evolved with improved imaging modalities and a deeper understanding of glenohumeral biomechanics. Modern orthopedic practice now emphasizes accurate characterization of fracture patterns, particularly those involving the glenoid articular surface or significantly disrupting the mechanical axis of the shoulder. Given the typical mechanism of injury, a comprehensive trauma workup is paramount, extending beyond the shoulder to encompass the entire ipsilateral upper torso, spine, and thoracic cavity.
Surgical Anatomy and Biomechanics
The scapula is a flat, triangular bone crucial for linking the upper extremity to the axial skeleton. Its complex three-dimensional structure and extensive muscular attachments contribute to its unique biomechanical role, allowing for a wide range of shoulder motion while providing a stable base for the glenohumeral joint. The robust surrounding muscle mass, including the deltoid, rotator cuff, pectoralis major, latissimus dorsi, and serratus anterior, along with the inherent mobility of the scapulothoracic articulation, aids in dissipating forces and protecting the bone from direct impact.
Scapular Anatomical Regions
The scapula comprises several distinct anatomical regions, each with unique surgical implications when fractured:
* Body: The broad, flat portion of the scapula. Fractures here are often comminuted and can be associated with significant soft tissue injury.
* Spine: A prominent ridge that divides the posterior surface into the supraspinous and infraspinous fossae. It terminates laterally as the acromion.
* Acromion: The lateral extension of the scapular spine, forming the roof of the glenohumeral joint and articulating with the clavicle. Acromial fractures can lead to subacromial impingement or deltoid dysfunction.
* Coracoid Process: A hook-like anterior projection serving as an attachment site for several muscles and ligaments (e.g., pectoralis minor, coracobrachialis, short head of biceps, coracoacromial ligament, coracoclavicular ligaments). Fractures here can compromise superior shoulder stability.
* Glenoid: The shallow articular fossa that articulates with the humeral head, forming the glenohumeral joint. Glenoid fractures are intra-articular and can significantly impact joint congruence and stability.
* Neck: The constricture between the body and the glenoid. Fractures here can lead to significant displacement of the glenoid fragment relative to the scapular body, affecting glenohumeral alignment.
Muscular and Ligamentous Attachments
The scapula serves as the origin or insertion point for 17 muscles, providing dynamic stability and facilitating complex shoulder movements. Key muscles include the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis), deltoid, biceps, triceps, trapezius, rhomboids, levator scapulae, and serratus anterior. The integrity of these muscular attachments is vital for shoulder function. Ligamentous structures such as the coracoclavicular ligaments (conoid and trapezoid), coracoacromial ligament, and glenohumeral ligaments play critical roles in shoulder stability and are often involved in scapular fracture-dislocations or avulsion injuries.
Neurovascular Structures
Understanding the proximity of neurovascular structures is paramount in the surgical management of scapular fractures. The suprascapular nerve (C5-C6) is particularly vulnerable as it courses through the suprascapular notch (under the superior transverse scapular ligament) and then the spinoglenoid notch (under the spinoglenoid ligament) to innervate the supraspinatus and infraspinatus muscles. Injury to this nerve can result in significant shoulder dysfunction and pain. The axillary nerve and posterior circumflex humeral artery are intimately associated with the surgical neck of the humerus but are also at risk with significant displacement of glenoid or neck fractures, particularly during approaches that risk posterior inferior dissection. The brachial plexus is located superior to the scapula, and severe trauma causing scapular fractures can involve traction or direct injury to these critical nerves.
Mechanism of Injury
Scapular fractures are typically the result of high-energy trauma, underscoring the necessity of a thorough systemic evaluation.
* Direct Trauma: A direct blow or fall onto the posterior aspect of the shoulder often results in body or spine fractures. Direct trauma to the point of the shoulder can lead to acromial or coracoid fractures.
* Motor vehicle accidents (MVAs) account for approximately 50% of cases, while motorcycle accidents contribute 11% to 25%.
* Indirect Injury: Axial loading on an outstretched arm can transmit forces through the humerus to the glenoid, leading to scapular neck, glenoid, or intra-articular fractures.
* Avulsion Fractures: Strong muscular contractions or ligamentous avulsions can cause small avulsion fractures, such as at the coracoid (due to pectoralis minor, coracobrachialis, or biceps short head) or glenoid rim (due to glenohumeral ligament traction in dislocations).
* Shoulder Dislocation: May directly cause glenoid rim fractures (Bony Bankart lesions) due to impaction of the humeral head against the glenoid anteriorly or posteriorly.
Associated Injuries
The presence of a scapular fracture should raise a high index of suspicion for concomitant injuries, given the significant force required to fracture the scapula. The reported incidence of associated injuries ranges widely from 35% to 98%. A systematic approach to trauma evaluation is essential.
* Ipsilateral upper torso injuries:
* Fractured ribs (common)
* Clavicle fractures (often part of a "floating shoulder" injury, where both the clavicle and scapular neck are fractured)
* Sternum fractures
* Pneumothorax (11% to 55% of scapular fractures)
* Pulmonary contusion (11% to 54% of scapular fractures)
* Hemothorax
* Injuries to neurovascular structures:
* Brachial plexus injuries (ranging from neuropraxia to complete avulsion)
* Subclavian or axillary artery/vein injuries (vascular avulsions, pseudoaneurysms)
* Suprascapular nerve injury
* Spine injuries:
* Cervical spine (approximately 20% of scapular fractures)
* Thoracic spine (approximately 76% of scapular fractures)
* Lumbar spine (approximately 4% of scapular fractures)
* Head trauma, abdominal trauma, and long bone fractures are also frequently observed.

Illustration of scapular anatomy and surrounding structures.

Typical mechanism of high-energy trauma leading to scapular fractures.
Indications and Contraindications
The decision between operative and non-operative management of scapular fractures is complex, depending on fracture morphology, displacement, articular involvement, patient factors, and associated injuries. The primary goals of treatment are to restore glenohumeral stability, achieve adequate range of motion, and prevent long-term pain and dysfunction.
Clinical Evaluation
A full trauma evaluation is paramount in patients presenting with a suspected scapular fracture. Initial assessment should follow Advanced Trauma Life Support (ATLS) protocols, prioritizing airway, breathing, circulation, disability, and exposure.
Patients typically present with the affected upper extremity supported by the contralateral hand in an adducted and immobile position, experiencing severe pain with any shoulder movement, especially abduction. A careful examination will reveal tenderness, swelling, and possibly ecchymosis over the scapular region. Crepitus may be palpable. A thorough neurovascular examination of the entire upper extremity is mandatory to assess for brachial plexus, axillary nerve, or vascular injuries. Associated chest wall injuries must be actively sought.
Imaging Modalities
- Radiographs: Standard trauma series includes AP, scapular Y-view, and axillary lateral views. Specialized views like the Stryker notch view (for posterior glenoid rim) or West Point axillary view (for anterior glenoid rim) may be useful.
- Computed Tomography (CT): Essential for detailed characterization of fracture patterns, especially for intra-articular involvement (glenoid fractures), fracture displacement, and comminution. 3D reconstructions are invaluable for pre-operative planning.

CT image demonstrating a complex scapular body fracture. - Magnetic Resonance Imaging (MRI): Less commonly used in acute trauma but can be helpful in assessing soft tissue injuries, rotator cuff tears, or brachial plexus involvement if clinical suspicion is high and CT is inconclusive.
Classification Systems
Several classification systems exist, primarily aiding in communication and guiding treatment decisions:
* AO/OTA Classification: A comprehensive system for all fractures, including scapula (15-E series).
* Ideberg Classification (for glenoid fractures): Categorizes glenoid fractures based on their anatomical location and involvement of the articular surface. Types I-VI, with increasing complexity and articular compromise.
* Orthopaedic Trauma Association (OTA) Classification: A hierarchical system that defines fracture patterns.
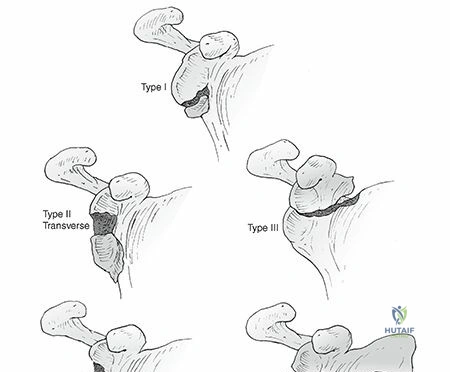
* Mayo Classification (for acromial fractures): Type I (nondisplaced), Type II (displaced but not involving the deltoid insertion), Type III (displaced and involving the deltoid origin, leading to deltoid detachment).
* Goss Classification (for floating shoulder): Defines stable vs. unstable floating shoulder injuries based on coracoclavicular ligament integrity.
Operative vs. Non-Operative Indications
The decision for surgical intervention is guided by the degree of displacement, articular involvement, stability of the glenohumeral articulation, and the presence of a "floating shoulder" injury.
| Criterion | Indications for Non-Operative Management | Indications for Operative Management |
|---|---|---|
| Fracture Type & Displacement | - Scapular body fractures with minimal displacement (<1 cm translation, <30° angulation). - Scapular spine fractures with minimal displacement. - Nondisplaced or minimally displaced (≤2 mm step-off) glenoid rim fractures. - Nondisplaced or stable coracoid/acromial fractures (e.g., Mayo Type I acromial, stable base coracoid fractures). - Scapular neck fractures with minimal angulation (<20-30°) and translation (<1 cm), particularly in older, low-demand patients. |
- Glenoid articular step-off or gap >2-3 mm. - Glenoid fractures involving >25% of the articular surface and associated with glenohumeral instability. - Scapular neck fractures with significant angulation (>20-30° medial or lateral) or translation (>1 cm), especially with glenoid fragment malorientation. - Displaced fractures disrupting the superior shoulder suspensory complex (e.g., "floating shoulder" with compromised CC ligaments or unstable clavicle fracture). - Displaced acromial fractures (Mayo Type II, III) causing impingement or deltoid dysfunction. - Displaced coracoid fractures associated with significant instability (e.g., coracoclavicular ligament disruption). |
| Associated Injuries | - No significant associated injuries that necessitate surgery. | - "Floating shoulder" (ipsilateral clavicle and scapular neck/body fracture) with significant displacement or disruption of the superior shoulder suspensory complex, particularly if medial clavicle displacement is >100% or angulation >45°. - Brachial plexus injury where reduction of fracture may relieve pressure. - Open fractures (rare). |
| Patient Factors & Co-morbidities | - Medically unstable patient. - Severe osteoporosis. - Significant soft tissue compromise limiting surgical access. - High surgical risk (ASA Class III/IV) where benefits of surgery do not outweigh risks. - Patient preference for non-operative care after informed consent. |
- Young, active, high-demand patient. - Polytrauma patient where definitive fixation is part of overall stabilization. - Patient compliance with rehabilitation. - Absence of absolute contraindications. |
| Glenohumeral Instability | - Stable glenohumeral joint. | - Persistent glenohumeral instability despite attempts at closed reduction. - Large articular fragment displacement leading to joint incongruity. |
Absolute Contraindications to Surgery:
* Hemodynamic instability: Patient instability precluding safe anesthesia and surgery.
* Severe comorbidities: Uncontrolled systemic diseases that make surgery excessively risky.
* Active infection: Local or systemic infection.
* Severe soft tissue compromise: Extensive devitalization, open wounds unsuitable for primary closure.
Relative Contraindications to Surgery:
* Severe osteoporosis with poor bone quality for fixation.
* Smoking or other factors impairing wound healing.
* Patient factors that may limit rehabilitation compliance.
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is essential for successful surgical management of scapular fractures, particularly given their complex anatomy and association with high-energy trauma.
Pre-operative Planning
- Comprehensive Trauma Workup: Re-evaluate the patient's overall condition. Ensure all life-threatening injuries are addressed. Optimize medical comorbidities.
- Detailed Imaging Review:
- Review all radiographs (AP, Y-view, axillary).
- Crucially, meticulously analyze the CT scan with 3D reconstructions. Identify all fracture lines, displacement, angulation, and articular involvement (especially for glenoid fractures). Determine the number and size of fragments, particularly for the glenoid.

3D CT reconstruction demonstrating complex scapular body and neck fracture.

Additional 3D CT view showing glenoid fracture extension. - Identify potential neurovascular structures at risk based on fracture pattern and planned approach.
- Classification Application: Use relevant classification systems (Ideberg, OTA, Mayo, Goss) to communicate and guide planning.
- Surgical Approach Selection: Based on the fracture location and displacement, select the optimal surgical approach. Many scapular fractures, especially glenoid and neck fractures, often require a posterior approach. Acromial or coracoid fractures may require superior or anterior approaches.
- Implant Selection: Plan for appropriate implant size and type. This typically involves 2.7 mm or 3.5 mm reconstruction plates, L- or T-plates for glenoid fixation, and small fragment plates for body or neck fractures. Consider specific glenoid fixation systems or modular plates.
- Contingency Planning: Anticipate potential challenges, such as comminution, soft tissue difficulties, or difficulty achieving reduction. Have additional implants, bone graft material, and alternative approaches ready.
- Surgical Consent: Thoroughly discuss the procedure, potential benefits, risks (infection, nerve injury, nonunion, stiffness), and expected outcomes with the patient.
Patient Positioning
Proper patient positioning is critical for adequate exposure, ease of surgical manipulation, and safety.
1. General Anesthesia: Administered by the anesthesia team. Consideration for regional blocks (e.g., interscalene block) for post-operative pain management.
2. Prone Position: Rarely used for scapula fractures, primarily for posterior approaches when extreme posterior access is needed or when combined with spinal surgery.
3. Lateral Decubitus Position:
* Indications: Most commonly used for posterior approaches (Judet approaches) to access the posterior glenoid, scapular neck, and body. Provides excellent exposure and allows for good intraoperative fluoroscopy access.
* Setup: Patient is positioned lateral with the injured side up. Adequate padding is essential at all pressure points (axilla, malleoli, knees). The non-operative arm is supported on an arm board. The operative arm is draped free or supported on a sterile arm holder, allowing for intraoperative manipulation. The head is supported in a neutral position. A beanbag or bolsters are used to stabilize the torso.
* Fluoroscopy: Ensure the C-arm can obtain true AP, Y-view, and axillary views of the scapula. This often requires careful positioning of the patient and the C-arm.

Patient positioned in lateral decubitus for posterior approach to the scapula.
4. Beach Chair Position:
* Indications: Useful for superior and anterior approaches, such as addressing acromial fractures, coracoid fractures, or anterior glenoid rim fractures. Offers advantages for managing associated clavicle fractures or rotator cuff pathologies.
* Setup: Patient is placed in a semi-sitting position with the torso elevated. The head is supported in a neutral position with a headrest. The operative arm is draped free, allowing for mobility. Pressure points (occiput, sacrum, heels) must be padded.
* Fluoroscopy: Ensure good AP and lateral views of the scapula and glenohumeral joint are achievable.
Prepping and Draping: The shoulder and entire arm, up to the neck and across the midline posteriorly and anteriorly, are prepped and draped to allow for extensive exposure and free manipulation of the extremity.
Detailed Surgical Approach and Technique
Surgical treatment of scapular fractures requires precise anatomical knowledge, meticulous dissection, and careful reduction and fixation techniques. The choice of surgical approach is dictated by the fracture pattern and location.
Posterior Approaches (Judet Approaches)
These are the workhorse approaches for fractures of the glenoid, scapular neck, and body. They utilize internervous planes to minimize muscle disruption.

Illustration of Judet surgical approaches to the scapula.
1. Standard Posterior Approach (Judet)
- Incision: A curvilinear incision parallel to the scapular spine, extending from the acromion medially towards the vertebral border and then curving inferiorly along the medial border of the scapula. Alternatively, a straight incision directly over the scapular spine can be used for more superior access.
- Internervous Plane: The critical aspect of this approach is developing the internervous plane between the deltoid and the triceps. The deltoid (innervated by the axillary nerve) is reflected laterally, and the triceps long head (innervated by the radial nerve) is retracted medially.
- Muscle Dissection:
- The skin and subcutaneous tissues are incised.
- The deltoid fascia is incised, and the deltoid muscle is elevated from its origin on the scapular spine and retracted laterally.
- The infraspinatus and teres minor muscles (both innervated by the suprascapular nerve and axillary nerve, respectively) are identified.
- For glenoid and neck fractures, the interval between the infraspinatus and teres minor is developed. This exposes the posterior capsule of the glenohumeral joint and the posterior aspect of the scapular neck. The suprascapular nerve and vessels are protected in the spinoglenoid notch.
- For more extensive exposure of the scapular body, the infraspinatus can be carefully elevated from the scapular fossa.
- Exposure: This approach provides excellent visualization of the posterior glenoid, scapular neck, and most of the scapular body.
2. Lateral Posterior Approach (Modified Judet)
- Incision: A more lateral approach, often a slightly curved incision running from the posterior aspect of the acromion distally towards the posterior axillary fold.
- Internervous Plane: Utilizes the interval between the posterior deltoid (axillary nerve) and the teres major/latissimus dorsi (lower subscapular nerve/thoracodorsal nerve).
- Muscle Dissection: The posterior deltoid is elevated and retracted superiorly and anteriorly. The infraspinatus and teres minor are retracted medially. The long head of the triceps is usually retracted inferiorly.
- Exposure: Provides good access to the lateral aspect of the scapula, including the glenoid, neck, and lateral body, particularly useful for fractures involving the glenoid or lateral pillar. This approach minimizes disruption to the medial muscular attachments.
Reduction and Fixation Principles for Glenoid, Neck, and Body Fractures
- Indirect Reduction: Initial gentle traction on the arm can help align major fragments.
- Direct Reduction:
- Fragment Identification: Identify all major fracture fragments using intraoperative fluoroscopy and direct visualization.
- Articular Reconstruction (Glenoid): The primary goal for intra-articular glenoid fractures is anatomical reduction of the articular surface. Small, pointed reduction clamps or Hohmann retractors can be used to manipulate fragments. K-wires are essential for temporary fixation.
- Neck and Body Reduction: For neck fractures, restore the glenoid-to-scapular body relationship. For body fractures, restore the overall contour. External manipulation or direct clamping can be used.
- Temporary Fixation: K-wires are invaluable for provisionally stabilizing fragments after reduction.
- Definitive Fixation:
- Plating: Small fragment plates (2.7 mm or 3.5 mm) are typically used. Reconstruction plates can be contoured to match the complex curves of the scapula. L- or T-plates are often employed for glenoid rim fractures.
- Screw Placement: Screws should achieve bicortical purchase where possible and be placed to provide maximum stability without endangering neurovascular structures. Lag screws are crucial for interfragmentary compression, especially for articular fragments. Neutralization plates are then applied to protect the lag screws.
- Glenoid Fixation: For Ideberg Type I and II fractures (rim), screws across the fragment into the glenoid neck are used. For Type III and V (body extension), plates along the lateral border of the scapular spine and lateral scapular border are common. For central fractures (Type IV, VI), more complex plating and potentially anterior approaches may be required.

Intraoperative fluoroscopy image showing plate and screw fixation of a scapular fracture.

Postoperative radiograph demonstrating internal fixation of a scapular fracture.
Anterior Approaches (e.g., Deltopectoral Approach)
- Indications: Primarily for coracoid fractures, anterior glenoid rim fractures, or when combined with anterior clavicle fixation.
- Incision: A curvilinear incision from the coracoid process inferiorly along the deltopectoral groove.
- Internervous Plane: Between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves). The cephalic vein is identified and retracted laterally or medially.
- Exposure: Allows access to the coracoid, anterior glenoid, and anterior aspect of the scapular neck. Care must be taken to protect the musculocutaneous nerve, which enters the coracobrachialis muscle.
Acromial and Coracoid Fractures
- Acromial Fractures: If significantly displaced (Mayo Type II or III) and causing impingement or deltoid dysfunction, open reduction and internal fixation may be warranted. A superior approach over the acromion is used. Fixation often involves small plates, tension band wiring, or screws.
- Coracoid Fractures: Surgical fixation is indicated if associated with significant superior shoulder instability (e.g., disruption of the coracoclavicular ligaments or a "floating shoulder") or significant displacement causing impingement. Fixation can be achieved with a single screw or small plate via an anterior approach.

Anatomical view highlighting the coracoid process and its attachments.
Intraoperative Considerations
- Neurovascular Protection: Meticulous dissection and careful retraction are crucial to protect the axillary nerve, suprascapular nerve, and surrounding vessels.
- Fluoroscopy: Essential throughout the procedure to confirm reduction, implant placement, and ensure no intra-articular screw penetration. Obtain true AP, Y-view, and axillary views.
- Soft Tissue Management: Minimize soft tissue stripping to preserve vascularity. Careful hemostasis.
- Articular Surface Assessment: For glenoid fractures, direct visualization and palpation of the articular surface (if possible) are critical to ensure anatomical reduction. Arthroscopy can be a useful adjunct for evaluating glenoid articular congruity in selected cases.
Complications and Management
Complications associated with scapular fractures, whether treated operatively or non-operatively, can range from minor to severely debilitating. A thorough understanding of these potential issues and their management strategies is crucial for optimal patient outcomes.
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Nonunion/Malunion | Variable; higher in severely displaced fractures, inadequate fixation, or non-operative management of unstable patterns. Reported incidence <5% for body fractures, but can be higher for glenoid neck or articular fractures if initial reduction or fixation is suboptimal. Malunion can occur in 10-20% of cases, especially with body/neck fractures. | Nonunion: Revision ORIF with robust fixation, bone grafting (autograft or allograft), potentially plate augmentation. Address underlying causes (e.g., infection, poor biology). Malunion: Corrective osteotomy (scapular body or neck) to restore alignment and kinematics, especially if symptomatic (e.g., impingement, pain, restricted motion). Arthroplasty (e.g., reverse shoulder arthroplasty) for severe glenoid malunion with intractable pain and dysfunction in older patients. |
| Post-traumatic Arthritis (Glenoid) | Direct correlation with articular step-off and gap. >2-3 mm articular incongruity significantly increases risk. Incidence can be as high as 20-30% in complex glenoid fractures. | Early: Aggressive rehabilitation to maintain motion, pain management. Late: Arthroscopic debridement, capsular release, or synovectomy for mild cases. Glenohumeral arthroplasty (total shoulder arthroplasty or reverse shoulder arthroplasty) for severe, debilitating arthritis with persistent pain and loss of function. |
| Stiffness / Loss of Motion | Very common, especially after prolonged immobilization or extensive soft tissue dissection. Can range from 10-50%, depending on fracture type and rehabilitation adherence. | Early: Aggressive, guided physical therapy focusing on PROM, AAROM, and AROM within safe limits. Modalities for pain control. Late/Refractory: Manipulation under anesthesia (MUA) for intractable stiffness. Arthroscopic or open arthrolysis and capsular release. Prevention is key through early, appropriate rehabilitation. |
| Neurovascular Injury | Pre-existing: Up to 15-20% for brachial plexus injuries in high-energy trauma. Suprascapular nerve palsy often associated with neck fractures. Iatrogenic: Rare, but can occur with misguided hardware or excessive retraction. Axillary nerve injury (posterior approach), suprascapular nerve injury (spinoglenoid notch during posterior dissection). |
Pre-existing: Early diagnosis and neurology consultation. Observation for neuropraxia. Surgical exploration and repair/grafting if indicated (e.g., complete transection, non-recovering deficits). Iatrogenic: Immediate recognition and removal of hardware if compressive. Surgical exploration and nerve repair/grafting if transected. |
| Infection | Relatively low incidence for elective ORIF (1-5%), but can be higher in open fractures or polytrauma patients. | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics based on culture sensitivities. Retained hardware may need to be removed once the fracture has united or if infection persists. |
| Hardware Impingement/Failure | Variable, depends on implant selection, placement, and patient activity. Can occur with prominent plates/screws near the deltoid or rotator cuff insertion, or if fixation is inadequate for the forces applied. | Symptomatic hardware removal after fracture union. Revision fixation if hardware fails and nonunion develops. Careful pre-operative planning and intraoperative assessment of implant position relative to soft tissues. |
| Heterotopic Ossification (HO) | Can occur, particularly in conjunction with head trauma or extensive soft tissue injury. | Prevention: Low-dose radiation or NSAIDs (e.g., indomethacin) in high-risk patients. Treatment: Surgical excision of mature HO if symptomatic and causing significant loss of motion, usually after a quiescent phase. |
| Residual Pain | Common, can be due to malunion, post-traumatic arthritis, nerve injury, or soft tissue scarring. | Multimodal pain management, physical therapy, nerve blocks, consideration of hardware removal, or surgical correction of underlying pathology (e.g., osteotomy for malunion, arthroplasty for arthritis). Psychological support for chronic pain. |
| Associated Injury Complications | (e.g., Pneumothorax, Pulmonary contusion, Hemothorax, Rib fractures) Incidence 35-98% for associated injuries overall. Specific incidence varies by injury type. | Managed according to ATLS principles. Thoracic trauma management by chest tube drainage, ventilatory support, pain control, and surgical stabilization of rib fractures if indicated. Collaborative care with trauma surgeons, pulmonologists. These injuries must be managed concurrently with the scapular fracture. |
Prevention and Mitigation
Many complications can be minimized by:
* Meticulous Pre-operative Planning: Thorough understanding of fracture morphology and neurovascular anatomy.
* Appropriate Surgical Technique: Gentle tissue handling, precise reduction, stable fixation, and careful neurovascular protection.
* Early and Guided Rehabilitation: Initiating motion within safe limits as soon as feasible to prevent stiffness, while protecting the repair.
* Prophylactic Measures: Antibiotics for surgical prophylaxis, thromboembolism prophylaxis, and sometimes HO prophylaxis.
* Comprehensive Trauma Management: Addressing all associated injuries in a timely and coordinated fashion.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation following scapular fracture fixation is a critical component of successful outcomes, aiming to restore pain-free motion, strength, and function. Protocols must be tailored to the specific fracture pattern, the stability of fixation, and the patient's individual healing capacity and goals. Collaboration between the orthopedic surgeon and physical therapist is essential.
General Principles
- Protection of Fixation: The primary concern in the early phase is to protect the surgical repair while initiating motion.
- Gradual Progression: Rehabilitation should be phased, with a progressive increase in activity and load as healing progresses.
- Pain Management: Adequate pain control is vital to allow patient participation in therapy.
- Patient Education: Patients must understand the importance of adherence to the protocol and the rationale behind restrictions.
Phased Rehabilitation Protocol
Phase 1: Immobilization and Early Protected Motion (Weeks 0-6)
- Goals: Protect surgical repair, minimize pain and swelling, prevent stiffness, and initiate early passive motion.
- Immobilization:
- Sling immobilization is typically used for 4-6 weeks, with removal for exercises and hygiene only.
- No active shoulder motion is allowed.
- Elbow, wrist, and hand active range of motion (AROM) exercises should begin immediately to prevent stiffness in these joints.
- Passive Range of Motion (PROM):
- Pendulum exercises: Started early (Day 1-3 post-op) to encourage gentle motion without active muscle contraction.
- Codman exercises: Gentle circumduction movements to the tolerance of the patient.
- Assisted PROM: Therapist-assisted or patient self-assisted external rotation (limited to 0-30° initially), flexion (limited to 0-90°), and abduction (limited to 0-45°). These limits are often dictated by the fracture stability and surgeon preference. No aggressive stretching or end-range mobilization.
- Precautions:
- No active abduction or elevation against gravity.
- No lifting, pushing, or pulling with the affected arm.
- Avoid external rotation past neutral if glenoid anterior fracture fixation.
- Avoid internal rotation past neutral if glenoid posterior fracture fixation.
Phase 2: Active Assisted and Active Motion (Weeks 6-12)
- Goals: Restore full, pain-free active range of motion, initiate gentle strengthening, and improve neuromuscular control.
- Progression from Sling: Gradual weaning from the sling around 6 weeks post-op, depending on radiographic evidence of healing and clinical assessment of stability.
- Active Assisted Range of Motion (AAROM):
- Continue with therapist-assisted or self-assisted exercises, gradually increasing range of motion in all planes.
- Pulley exercises, wand exercises.
- Active Range of Motion (AROM):
- Begin active motion without assistance, first in supine, then progressing to upright positions.
- Focus on achieving functional overhead motion (flexion, abduction) and rotational movements.
- Gentle Strengthening (Isometrics):
- Initiate isometric contractions for rotator cuff muscles and scapular stabilizers (e.g., internal rotation, external rotation, abduction, adduction) with the arm in a neutral, protected position.
- No resisted exercises with weights yet.
- Scapular Stabilization: Focus on exercises to improve periscapular muscle control and stability (e.g., scapular retraction, protraction, depression, elevation).
Phase 3: Progressive Strengthening and Functional Return (Weeks 12-24+)
- Goals: Restore full strength, power, endurance, and return to pre-injury activities.
- Progressive Resistive Exercises (PREs):
- Gradual introduction of resistance with elastic bands, light weights, and eventually machine weights.
- Target all major muscle groups of the shoulder girdle: rotator cuff, deltoid, pectoralis, latissimus, rhomboids, trapezius, serratus anterior.
- Concentric and eccentric strengthening.
- Proprioceptive Training:
- Exercises to improve joint position sense and dynamic stability (e.g., rhythmic stabilization, balance exercises).
- Functional and Sport-Specific Training:
- For athletes or individuals with demanding occupations, incorporate exercises mimicking their specific activities.
- Gradual return to sport or work, with close monitoring for pain or symptoms.
- Return to Activity:
- Light, non-contact activities may resume around 4-6 months, depending on strength, range of motion, and comfort.
- Contact sports or heavy overhead work typically requires 6-12 months or longer. Full recovery can take up to a year or more.

Postoperative rehabilitation emphasizing early passive range of motion.
Special Considerations
- Delayed Union/Nonunion: If healing is delayed, rehabilitation may need to be modified, potentially slowing progression or requiring further intervention.
- Stiffness: More aggressive stretching and mobilization may be indicated, potentially with MUA or arthrolysis if conservative measures fail.
- Nerve Injuries: Specific therapy protocols addressing nerve recovery may be needed, potentially involving bracing or adaptive equipment.
- Associated Injuries: Rehabilitation must also account for any concomitant injuries (e.g., rib fractures, clavicle fractures) which may influence the pace and type of exercises.
Summary of Key Literature and Guidelines
The management of scapular fractures has evolved significantly, moving from largely non-operative treatment to a more nuanced approach guided by detailed imaging and a better understanding of glenohumeral biomechanics. Key literature and guidelines emphasize the importance of fracture morphology, articular involvement, and stability of the superior shoulder suspensory complex (SSSC) in guiding treatment decisions.
Classification Systems and Prognostic Indicators
The Ideberg classification for glenoid fractures remains a cornerstone in guiding management, with Types I and II often managed non-operatively unless significantly displaced or unstable, while Types III-VI generally necessitate operative intervention due to significant articular disruption and instability. Similarly, the Goss classification for "floating shoulder" injuries highlights the importance of the SSSC. Disruption of both the clavicle and glenoid neck/body, particularly with significant displacement or compromise of the coracoclavicular ligaments, points towards an unstable injury requiring surgical stabilization. Studies by Hovelius et al. and Rommens et al. have underscored the long-term sequelae of malunited scapular neck and glenoid fractures, specifically post-traumatic arthritis and chronic pain, advocating for anatomical reduction where indicated.
Operative vs. Non-Operative Paradigm
While minimally displaced scapular body and spine fractures continue to be managed non-operatively with good outcomes, the literature supports operative fixation for:
* Glenoid fractures with >2-3 mm articular step-off or gap, or those causing glenohumeral instability (e.g., Karakas et al., Mayo et al.).
* Scapular neck fractures with significant angulation (>20-30°) or translation (>1 cm), particularly those leading to a medialized glenoid and compromised glenohumeral alignment (e.g., Cole et al., Zlowodzki et al.).
* Displaced acromial fractures causing impingement or deltoid dysfunction (e.g., Poehling et al., Mayo Classification).
* Coracoid fractures causing significant instability or impingement.
* Unstable "floating shoulder" injuries, where fixation of at least one component (often the clavicle or glenoid neck) is recommended to restore stability (e.g., Levy et al., van Noort et al.).
Surgical Approaches and Fixation Techniques
The posterior Judet approaches remain the standard for complex glenoid, neck, and body fractures, offering versatile exposure with acceptable morbidity. Modern fixation techniques employ anatomically contoured plates (e.g., reconstruction plates, L- and T-plates) with bicortical screw fixation and lag screw principles to achieve stable internal fixation. Advances in imaging, particularly 3D CT reconstruction, have significantly improved pre-operative planning and intraoperative navigation, leading to better anatomical reductions and lower complication rates.
Outcomes and Complications
Long-term studies suggest that operatively treated displaced scapular fractures generally yield superior functional outcomes compared to non-operative management, particularly concerning pain relief and improved range of motion, provided anatomical reduction and stable fixation are achieved (e.g., Nordqvist and Petersson, Giannoudis et al.). However, the literature also highlights a range of complications, including nonunion, malunion, post-traumatic arthritis (especially after glenoid fractures), neurovascular injury, and stiffness. Zlowodzki et al.'s meta-analysis emphasized that articular incongruity, even if subtle, is a significant predictor of post-traumatic arthritis. Early and appropriate rehabilitation protocols are crucial to mitigate stiffness and maximize functional recovery.
Current Trends and Future Directions
Current trends emphasize individualized treatment plans, balancing the risks of surgery against the potential for long-term dysfunction from malunion. There is ongoing research into optimal fixation strategies for complex glenoid fractures, the role of arthroscopy-assisted fixation, and the long-term impact of various rehabilitation protocols. The high association with other serious injuries continues to underscore the need for a comprehensive, multidisciplinary approach to patient care.

Postoperative AP radiograph of a fixed scapular fracture.

Postoperative Y-view radiograph showing stable fixation.
Clinical & Radiographic Imaging



