Comprehensive Introduction and Patho-Epidemiology
Epidemiology and Natural History
Rheumatoid arthritis (RA) is a chronic, systemic inflammatory condition characterized by a symmetric polyarthropathy that predominantly targets synovial joints. In the context of orthopedic surgery, the foot and ankle represent one of the most frequently and severely affected anatomic regions. Epidemiological data indicates that the foot is the initial site of clinical presentation in approximately 17% of patients with rheumatoid arthritis. Furthermore, as the systemic disease progresses, up to 90% of patients with chronic rheumatoid arthritis will eventually develop clinically significant involvement of the foot and ankle. The forefoot is the most commonly involved area, bearing the brunt of the biomechanical and inflammatory insults associated with the disease.
The natural history of rheumatoid forefoot deformity is relentlessly progressive if the underlying inflammatory cascade is not adequately controlled. The disease typically begins with an insidious onset of poorly defined forefoot pain, subtle swelling, and difficulty with prolonged ambulation. As unrelenting synovitis persists, it invariably leads to the distension of the joint capsule and the progressive attenuation of the critical ligamentous structures surrounding the metatarsophalangeal (MTP) joints. The longer the active rheumatoid disease is present, the greater the likelihood the patient will develop rigid, end-stage deformities. Early intervention with disease-modifying antirheumatic drugs (DMARDs) has altered this natural history favorably, but a significant cohort of patients still progresses to joint dislocation and severe degeneration requiring complex surgical reconstruction.

Patients inevitably present with a constellation of localized symptoms directly related to their structural deformities. The classic rheumatoid forefoot presentation includes a severe hallux valgus deformity combined with dorsal subluxation or frank dislocation of the lesser MTP joints. Patients frequently complain of severe shoe wear-related irritation along the prominent medial eminence of the hallux and along the dorsal aspects of the proximal interphalangeal (PIP) joints of the lesser toes. As the lesser toes dislocate dorsally, the metatarsal heads are driven plantarly, resulting in intractable pain and the formation of thick, painful calluses on the plantar aspect of the forefoot.
Pathogenesis of Forefoot Deformity
The pathogenesis of rheumatoid forefoot deformity is a complex interplay between chronic inflammatory synovitis and the repetitive biomechanical forces of normal gait. Unrelenting synovitis leads to a hypertrophic pannus that actively destroys articular cartilage and subchondral bone while simultaneously distending the joint capsule. This chronic capsular distension causes a profound stretching and eventual incompetence of the primary ligamentous stabilizers of the MTP joint, most notably the plantar plate and the collateral ligaments. The combination of ligamentous laxity and the dynamic forces of walking leads to progressive soft tissue instability, advanced articular cartilage destruction, and significant subchondral bone resorption.
As residual laxity progresses, the lesser MTP joints undergo dorsal subluxation and eventual dislocation. This catastrophic failure of the plantar plate allows the proximal phalanx to migrate dorsally while the metatarsal head is driven plantarly, protruding through the attenuated plantar capsule. Consequently, the protective plantar fat pad, which normally provides essential cushioning for the metatarsal heads during the terminal stance phase of gait, is dragged distally by its attachments to the base of the proximal phalanx. This distal migration of the fat pad leaves the prominent metatarsal heads completely exposed to the plantar skin, exponentially increasing focal peak plantar pressures and leading to the development of severe, intractable plantar keratoses (IPKs) or even full-thickness ulcerations.

The first ray is similarly affected by the rheumatoid inflammatory process, most commonly developing a severe hallux valgus deformity, though an occasional hallux varus may develop depending on the specific pattern of capsular failure. As the first MTP joint becomes unstable and deviates into valgus, it loses its critical weight-bearing function. This functional incompetence of the medial column results in a massive transfer of biomechanical load to the already compromised lesser metatarsals, a phenomenon known as transfer metatarsalgia. The severe hallux valgus deformity also physically impinges upon the adjacent lesser toes, exacerbating their deformities and contributing to the classic "wind-swept" appearance of the rheumatoid forefoot.
Differential Diagnosis
While rheumatoid arthritis is a leading cause of severe, multi-digit forefoot deformity, the orthopedic surgeon must maintain a broad differential diagnosis when evaluating a patient with polyarticular forefoot pain and structural collapse. Inflammatory arthritides such as psoriatic arthritis, Reiter syndrome (reactive arthritis), and ankylosing spondylitis can present with similar patterns of MTP joint synovitis and progressive deformity. However, these seronegative spondyloarthropathies often exhibit distinct clinical features, such as asymmetric involvement, dactylitis ("sausage digits"), enthesopathy, and specific radiographic hallmarks like periostitis or "pencil-in-cup" deformities that help differentiate them from classic rheumatoid arthritis.
Crystal-induced arthropathies, specifically gout and pseudogout, must also be considered in the differential diagnosis. Gout classically presents with acute, exquisitely painful, monoarticular flares (podagra) predominantly affecting the first MTP joint, driven by the deposition of monosodium urate crystals. While chronic tophaceous gout can cause significant joint destruction and multi-digit deformity that mimics rheumatoid arthritis, the presence of tophi, characteristic radiographic "rat-bite" erosions with overhanging margins, and joint aspiration confirming negatively birefringent crystals will establish the correct diagnosis. Pseudogout, caused by calcium pyrophosphate dihydrate (CPPD) crystal deposition, can also mimic rheumatoid flares but is more commonly associated with chondrocalcinosis on imaging.
Furthermore, connective tissue disorders such as systemic lupus erythematosus (SLE) can present with significant forefoot deformities. Lupus arthropathy (Jaccoud's arthropathy) is classically characterized by severe, reducible deformities driven by periarticular soft tissue laxity rather than the aggressive erosive joint destruction seen in rheumatoid arthritis. Advanced primary or post-traumatic osteoarthritis, while typically lacking the systemic inflammatory component, can also cause severe joint space narrowing, osteophyte formation, and deformity, though it usually lacks the profound osteopenia and marginal erosions characteristic of RA. Finally, severe neurologic disorders, particularly those causing intrinsic muscle wasting (e.g., Charcot-Marie-Tooth disease), can lead to profound cavovarus foot types with secondary claw toe deformities that must be distinguished from inflammatory etiologies.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Anatomy
The forefoot represents a highly specialized biomechanical construct designed to absorb shock during heel strike and provide a rigid lever arm for propulsion during toe-off. The metatarsophalangeal (MTP) joints are condylar synovial joints formed by the articulation of the convex metatarsal heads with the concave bases of the proximal phalanges. The articular cartilage of the metatarsal heads extends further on the plantar aspect than on the dorsal aspect, reflecting the normal functional arc of motion which requires significant dorsiflexion during the propulsive phase of gait. In the normal, non-pathologic state, the proximal phalanx of the hallux inherently possesses a physiologic valgus orientation of 0 to 15 degrees relative to the first metatarsal shaft at the MTP joint.
The lesser metatarsals (two through five) are arranged in a specific parabolic cascade that is critical for the even distribution of plantar pressures during the stance phase of gait. The second metatarsal is typically the longest and most rigidly fixed at its base, making it a central pillar of the forefoot but also highly susceptible to overload when the first ray fails. The third, fourth, and fifth metatarsals are progressively shorter and exhibit increasing mobility at their tarsometatarsal articulations. When planning surgical reconstruction, particularly lesser metatarsal head resections, recreating a smooth, physiologic cascade is absolutely paramount to prevent postoperative transfer lesions and localized pressure points.
The structural integrity of the subchondral bone is frequently compromised in the rheumatoid forefoot due to chronic hyperemia and the direct inflammatory effects of the synovial pannus. This leads to profound periarticular osteopenia, making the bone exceptionally soft and challenging to achieve rigid internal fixation during reconstructive procedures. Furthermore, the inflammatory process creates marginal cortical erosions at the "bare areas" of the joint—regions enclosed by the capsule but not covered by protective articular cartilage. These erosions act as stress risers and further degrade the mechanical integrity of the joint articulation.
Ligamentous and Capsular Stabilizers
The stability of the metatarsophalangeal joints is dependent on a complex and highly coordinated network of static ligamentous restraints. The most critical of these structures is the plantar plate, a thick, fibrocartilaginous structure that originates from the plantar aspect of the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. The plantar plate serves as the primary static restraint to dorsal translation of the proximal phalanx and provides a smooth gliding surface for the flexor tendons. In the rheumatoid foot, the plantar plate becomes attenuated and eventually ruptures under the chronic stress of capsular distension and altered biomechanics, leading to the hallmark dorsal MTP dislocation.
Medial and lateral stability of the MTP joint is provided by the collateral ligament complex, which consists of the proper collateral ligaments and the accessory collateral ligaments. The proper collateral ligaments originate from the dorsal-lateral aspects of the metatarsal head epicondyles and insert into the plantar-lateral bases of the proximal phalanx. The accessory collateral ligaments originate slightly more plantarly and insert directly into the margins of the plantar plate, functionally suspending the plantar plate beneath the metatarsal head. Chronic synovitis stretches these collateral ligaments asymmetrically, contributing to the multiplanar deformities (e.g., medial or lateral deviation of the toes) frequently observed in advanced rheumatoid disease.
The dorsal capsule of the MTP joint is relatively thin and provides minimal mechanical restraint to dislocation. However, it is intimately associated with the extensor tendons. A specialized plantar fat pad normally resides directly beneath the metatarsal heads, anchored in place by fibrous septae connecting to the plantar plate and the skin. This fat pad provides essential viscoelastic cushioning and protection for the metatarsal heads against the extreme sheer and compressive forces of walking. When the plantar plate fails and the proximal phalanx dislocates dorsally, it drags the plantar plate and the attached fat pad distally, leaving the prominent metatarsal heads completely devoid of their natural protective cushioning.
Musculotendinous Balance and Biomechanics
Dynamic stability of the forefoot relies on an exquisite balance between the extrinsic musculature (originating in the leg) and the intrinsic musculature (originating within the foot). The extrinsic muscles, specifically the extensor digitorum longus (EDL), extensor digitorum brevis (EDB), flexor digitorum longus (FDL), and flexor digitorum brevis (FDB), cross multiple joints and exert powerful forces on the forefoot. The intrinsic muscles, including the lumbricals and interossei, are critical modulators of these forces. The intrinsic muscles normally run plantar to the transverse axis of the MTP joint and dorsal to the axis of the PIP joint, thereby acting to plantarflex the MTP joint and extend the interphalangeal joints.
In the pathogenesis of the rheumatoid foot, as the primary static stabilizers fail and the MTP joint begins to subluxate dorsally, a catastrophic biomechanical shift occurs. The axis of the intrinsic muscles migrates from a plantar position to a position dorsal to the MTP joint center of rotation. Once this occurs, the intrinsic muscles lose their ability to plantarflex the MTP joint; instead, they become paradoxical dorsiflexors, actively exacerbating the dorsal subluxation. This loss of active MTP flexion and interphalangeal extension leads directly to the classic, rigid claw-toe deformity seen in advanced disease.
Furthermore, the windlass mechanism, driven by the plantar fascia, becomes severely compromised. Normally, dorsiflexion of the toes during terminal stance tightens the plantar fascia, elevating the longitudinal arch and locking the midtarsal joints to create a rigid lever for propulsion. In the rheumatoid foot with dislocated MTP joints and a deviated hallux, the plantar fascia cannot effectively engage. The loss of the windlass mechanism, combined with the loss of medial column weight-bearing due to hallux valgus, results in a profoundly inefficient, painful, and apropulsive gait pattern that forces the patient to ambulate with a protective, shuffling cadence.
Exhaustive Indications and Contraindications
Clinical Evaluation and Imaging
A meticulous clinical evaluation is the cornerstone of managing the rheumatoid forefoot. The examiner must begin by inspecting the foot with the patient in a weight-bearing, standing position to fully appreciate the dynamic nature of the deformities. The examiner should look specifically for the degree of hallux valgus orientation, the presence of pronation of the first ray, and its impingement on the adjacent lesser toes. The dorsal and plantar aspects of the forefoot must be carefully inspected and palpated. MTP instability can vary from subtle, reducible subluxation to rigid, irreducible dislocation. Palpation of the plantar aspect will often reveal severely prominent metatarsal heads and thick, painful calluses (IPKs) that are a primary source of the patient's disability.
A comprehensive examination must also include a detailed assessment of the range of motion for the ankle joint, subtalar joint, midtarsal joints, and MTP joints. Rheumatoid arthritis frequently involves the hindfoot and midfoot, leading to conditions such as pes planovalgus secondary to posterior tibial tendon dysfunction or subtalar joint arthritis. Failure to recognize and address proximal deformities will inevitably compromise the results of any fore
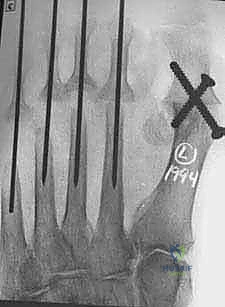
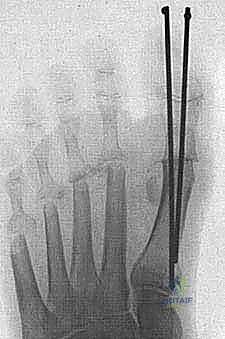
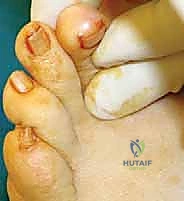
Clinical & Radiographic Imaging Archive