Rheumatoid Wrist Deformities: Surgical Management
Key Takeaway
Rheumatoid arthritis frequently targets the wrist, initiating a cascade of destructive synovitis, ligamentous laxity, and progressive deformity. Early intervention through dorsal or volar synovectomy can prevent debilitating tendon ruptures and halt joint subluxation. When advanced articular collapse occurs, reconstructive options such as total wrist arthroplasty or arthrodesis become necessary. This guide details the biomechanics, surgical indications, and step-by-step operative techniques for managing rheumatoid wrist deformities.
Pathophysiology and Biomechanics of the Rheumatoid Wrist
The wrist is frequently the keystone of functional impairment in the rheumatoid upper extremity. Synovitis of the wrist is often the initial manifestation of rheumatoid arthritis (RA), presenting as a painful, boggy swelling on the dorsum of the joint. The relentless proliferation of rheumatoid pannus initiates a destructive cascade: capsular distension, ligamentous attenuation, cartilage degradation, and eventual subchondral bone erosion.
Biomechanically, the rheumatoid wrist undergoes a predictable pattern of collapse. The destruction of the radiocarpal ligaments—particularly the radioscaphocapitate and radiolunate ligaments—leads to ulnar translation and palmar subluxation of the carpus. Concurrently, the distal radioulnar joint (DRUJ) is compromised. Destruction of the triangular fibrocartilage complex (TFCC) and the stabilizing ligaments of the distal ulna results in dorsal subluxation of the ulnar head (Caput Ulnae Syndrome).
As the carpus translates ulnarly and subluxates volarly, the metacarpals angulate radially, which in turn contributes to the classic ulnar deviation of the digits at the metacarpophalangeal (MCP) joints. Furthermore, the extensor carpi ulnaris (ECU) tendon sheath is often destroyed, allowing the ECU to subluxate volarly. Once volar to the axis of rotation, the ECU ceases to act as a wrist extensor and becomes a deforming flexor force, exacerbating the palmar flexion and radial deviation of the wrist.
Clinical Pearl: The "hourglass" swelling on the dorsum of the wrist is pathognomonic for severe tenosynovitis. The swelling is constricted centrally by the intact extensor retinaculum, creating bulging proximal and distal to the ligament.
Clinical Presentation and Radiographic Evaluation
Patients typically present with chronic wrist pain, swelling, and progressive loss of motion. Tenosynovial swelling may initially be misdiagnosed as de Quervain tenosynovitis, trigger finger, or idiopathic carpal tunnel syndrome if the underlying rheumatoid etiology is not suspected.
Radiographic evaluation is critical for staging the disease and planning surgical intervention.
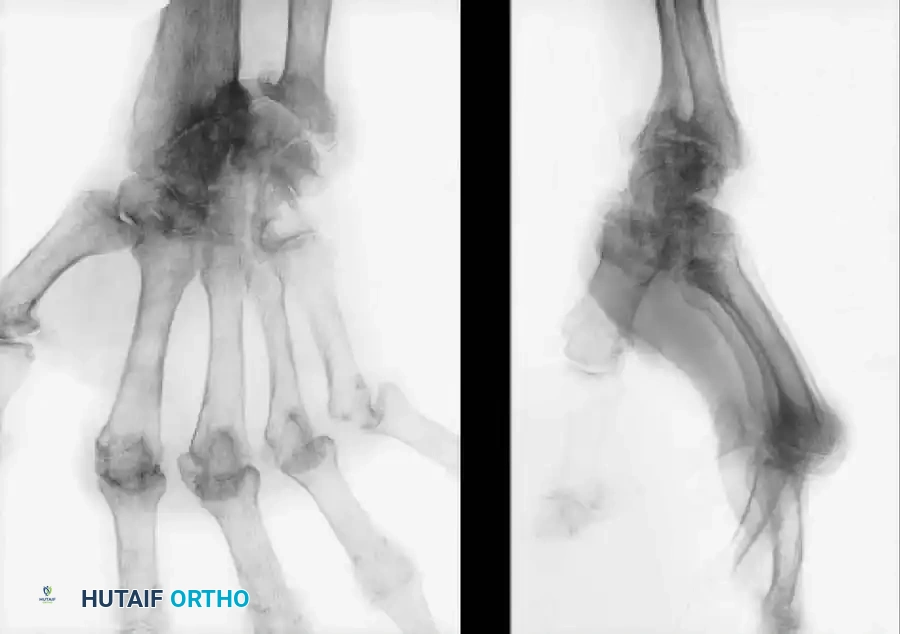
* Early signs: Periarticular osteopenia, soft tissue swelling, and a characteristic "small pit" or erosion at the base of the ulnar styloid.
* Intermediate signs: Joint space narrowing, marginal erosions (particularly at the scaphoid waist and ulnar head), and early ulnar translation of the carpus.
* Advanced signs: Severe carpal collapse, complete loss of joint space, volar subluxation of the carpus off the radius, and severe DRUJ destruction.
Indications for Surgical Intervention
Surgical management is dictated by the stage of the disease, the presence of tendon ruptures, and the patient's functional demands.
- Prophylactic Synovectomy: Indicated for persistent dorsal or volar tenosynovitis that fails to resolve after 6 weeks of adequate medical management (including disease-modifying antirheumatic drugs [DMARDs] and biologic agents). The primary goal is the prevention of attritional tendon ruptures.
- Tendon Rupture: Immediate surgical exploration, synovectomy, and tendon repair/transfer are indicated when a patient presents with a sudden loss of active digit extension or flexion.
- Nerve Compression: Carpal tunnel syndrome secondary to volar rheumatoid tenosynovitis that is refractory to splinting and corticosteroid injections requires surgical decompression and volar tenosynovectomy.
- Advanced Articular Destruction: Painful, unstable, and destroyed joints require reconstructive procedures, such as total wrist arthroplasty (TWA) or total wrist arthrodesis.
Dorsal Tenosynovectomy and Joint Synovectomy
Dorsal synovectomy is a highly effective, lasting procedure for relieving pain and preventing extensor tendon rupture in the presence of florid proliferative tenosynovitis.
Preoperative Planning and Positioning
The patient is positioned supine with the arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Loupe magnification is highly recommended to ensure meticulous clearance of the pannus without injuring the delicate extensor tendons.
Surgical Technique: Step-by-Step (Technique 70-36)

- Incision: Make a dorsal longitudinal incision, centered over the wrist joint, curving only slightly ulnarward. The incision must be long enough to expose the distal ulna and the entire dorsal carpal ligament.
> Surgical Warning: Avoid sharp curves or aggressive skin flaps, as the rheumatoid skin is often fragile and vascularity can be easily compromised, leading to marginal necrosis. - Nerve Protection: Carefully identify and preserve the larger dorsal veins, the dorsal sensory branch of the ulnar nerve, and the superficial branch of the radial nerve.
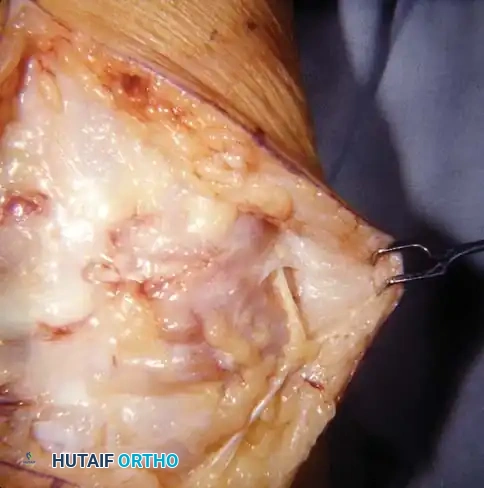
- Retinacular Flap Elevation: Raise a laterally based retinacular flap. Make transverse incisions at the proximal and distal ends of the extensor retinaculum. Crucially, at the proximal end, leave a 5 to 10 mm wide band of retinaculum intact to act as a pulley and prevent bowstringing of the extensor tendons postoperatively.

- Compartment Release: Connect the transverse retinacular incisions with a longitudinal incision over the sixth extensor compartment (ECU). Raise the flap from medial to lateral, sharply dividing the septa between the extensor compartments.
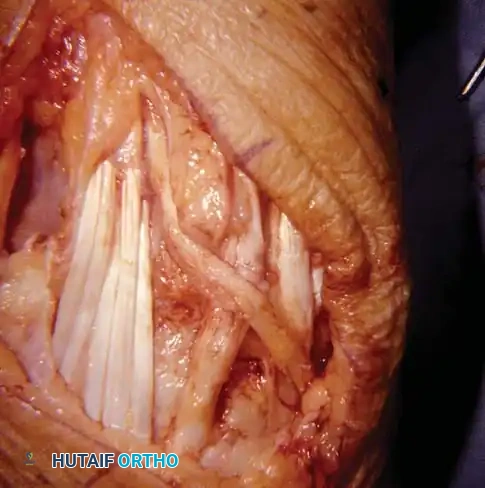
- Tenosynovectomy: Detach the dorsal carpal ligament from the radial side and reflect it as a continuous sheet. Meticulously excise the hypertrophied synovium from around the finger and radial wrist extensor tendons. Pay special attention to the Extensor Pollicis Longus (EPL) as it rounds Lister's tubercle, as this is a frequent site of attritional rupture.

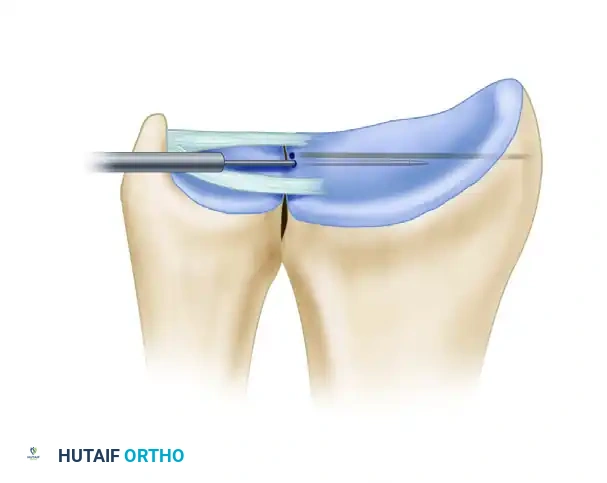
- DRUJ Management: Inspect the distal ulna and the DRUJ. If the attachments of the distal ulna to the radius and carpus are intact and the cartilage is preserved, do not disturb them. However, if the distal ulna is subluxated dorsally and denuded of cartilage, perform a distal ulnar resection (Darrach procedure). Excise approximately 1 cm of the distal ulna, smooth the remaining stump, and meticulously cover the medullary canal with local periosteum and capsular tissue to prevent painful impingement.
- ECU Relocation: Incise the sheath of the ECU near its insertion at the base of the fifth metacarpal. If the sheath is disintegrated and the tendon has subluxated palmarward (acting as a flexor), mobilize the tendon and return it to its anatomic dorsal position. Create a robust pulley using a strip of the dorsal retinaculum to maintain its reduction.
- Tendon Transfers: If preoperative assessment revealed an inability to actively dorsiflex and ulnarly deviate the wrist from a position of radial deviation, transfer the insertion of the Extensor Carpi Radialis Longus (ECRL) to the ECU tendon. This rebalances the wrist and corrects the deforming radial deviation force.
- Joint Synovectomy: Apply longitudinal traction to the hand to open the radiocarpal and midcarpal joints. Perform a thorough intra-articular synovectomy, removing pannus from between the carpal bones.
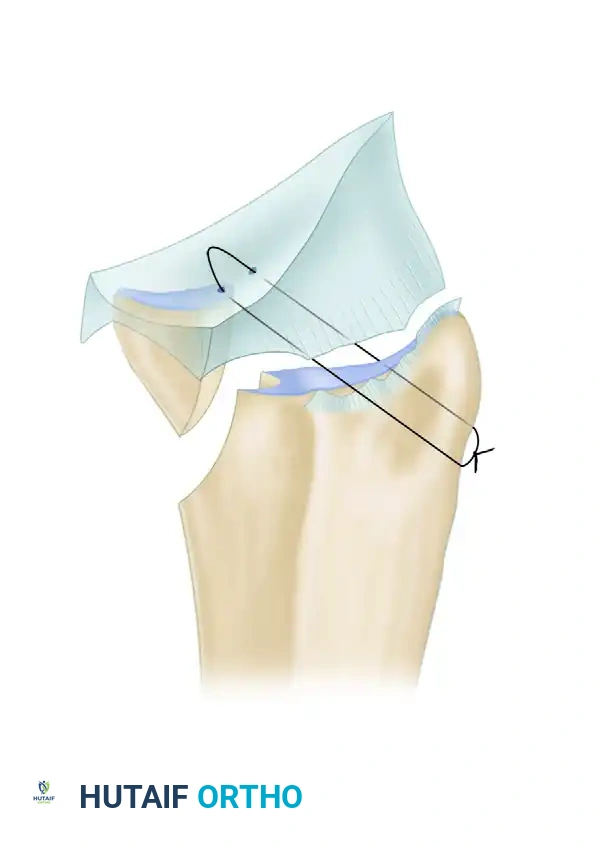
- Closure: Pass the elevated extensor retinacular flap deep to the long extensor tendons and suture its detached end in place medially. This provides a smooth gliding surface for the tendons and isolates them from the underlying radiocarpal joint, preventing recurrent pannus invasion.

- Hemostasis: Elevate the hand, release the tourniquet, and achieve meticulous hemostasis. Insert a closed-suction drain, close the skin with interrupted non-absorbable sutures, and apply a bulky compression dressing with a volar plaster splint holding the wrist in a neutral position.
Volar Tenosynovectomy and Carpal Tunnel Release
Volar rheumatoid tenosynovitis is insidious. Even slight hypertrophy of the tenosynovium, which may be clinically undetectable, can cause severe compression of the median nerve within the rigid confines of the carpal tunnel. Furthermore, invasive pannus can erode the floor of the carpal tunnel—specifically the distal radius and the scaphoid—creating sharp osteophytes that fray and rupture the deep flexor tendons (the classic "Mannerfelt lesion"). The Flexor Pollicis Longus (FPL) and the index Flexor Digitorum Profundus (FDP) are most commonly affected.

Surgical Technique: Step-by-Step (Technique 70-37)
- Incision: Utilize an extended carpal tunnel approach. Make a volar longitudinal incision beginning distally in the mid-palm, proceeding proximally parallel to the thenar crease, crossing the wrist crease obliquely (to avoid flexion contractures), and extending approximately 7.5 cm proximal to the wrist joint.
- Nerve Identification: Open the deep fascia proximally in the forearm and identify the median nerve. Dissect distally, staying strictly on the ulnar side of the nerve to protect the recurrent motor branch and the palmar cutaneous branch.
- Ligament Release: Completely divide the transverse carpal ligament to expose the flexor tendons. Note that the distal border of the ligament extends further into the palm than is often appreciated; ensure complete release.
- Tenosynovectomy: Beginning proximally and proceeding distally, meticulously dissect the hypertrophied tenosynovium from each individual flexor tendon. This is a tedious process requiring magnification. Evaluate all tendons for partial erosions or complete ruptures.

- Floor Inspection: Retract the flexor tendons and the median nerve to inspect the volar radiocarpal capsule. Look for eroded areas and protruding osteophytes, particularly over the scaphoid and distal radius.
- Osteophyte Excision: Use a rongeur to resect any sharp bony prominences. Meticulously close the capsuloligamentous layer over the carpal bones to provide a smooth gliding floor for the flexor tendons.
> Surgical Warning: Do not close the deep transverse carpal ligament, as this will recreate the compressive forces on the median nerve. - Closure: Release the tourniquet, obtain strict hemostasis, insert a drain, and close the skin. Apply a compression dressing and a volar plaster splint from the proximal forearm to the distal palmar crease, maintaining the wrist in slight extension.
Wrist Arthroplasty and Arthrodesis in the Rheumatoid Patient
When the articular surfaces are destroyed and the wrist is painful and unstable, reconstructive options must be considered. The choice between arthroplasty and arthrodesis depends on bone stock, tendon integrity, patient demands, and the status of the contralateral limb. If bilateral wrist reconstruction is required, every effort should be made to perform an arthroplasty on at least one side to preserve personal hygiene and functional independence.
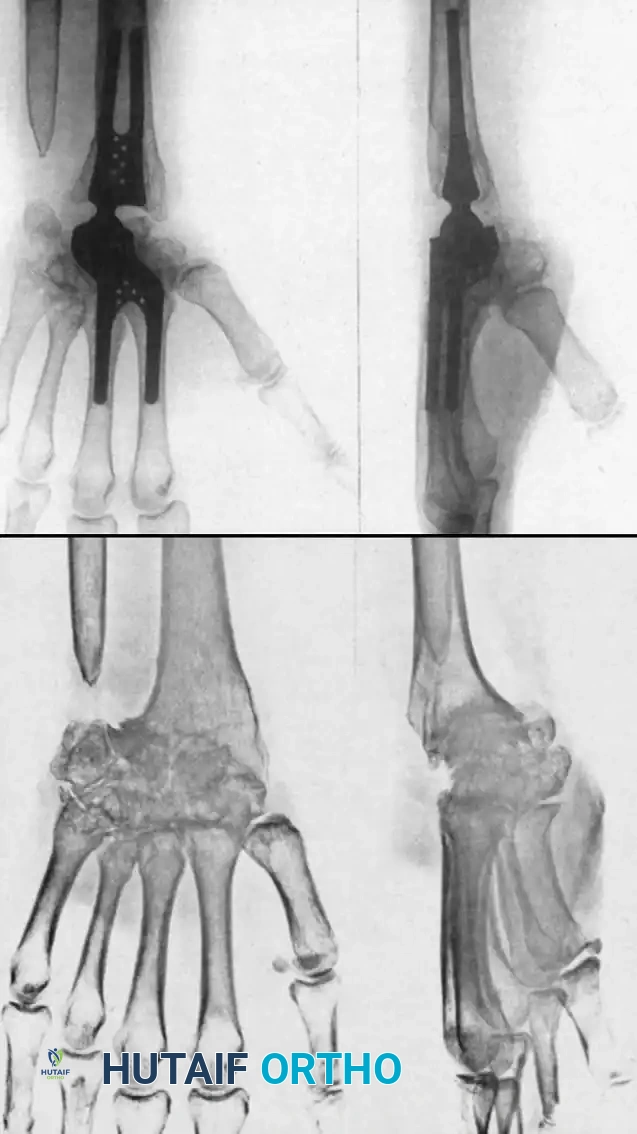
Silicone Implant Arthroplasty (Swanson)
Silicone spacer arthroplasty remains a viable option for low-demand rheumatoid patients with advanced disease (Stage III or IV) and poor bone stock that precludes the use of metal-on-plastic total wrist systems. The procedure requires minimal bone resection and acts as a dynamic spacer to maintain alignment while a fibrous capsule forms.
While pain relief is initially excellent, surgeons must counsel patients on the high complication rates associated with silicone implants over time. Long-term studies indicate a prosthetic fracture rate ranging from 10% to 52%, and progressive radiographic settling with bone resorption in up to 75% of cases. Despite these radiographic failures, clinical satisfaction often remains acceptable in low-demand individuals.
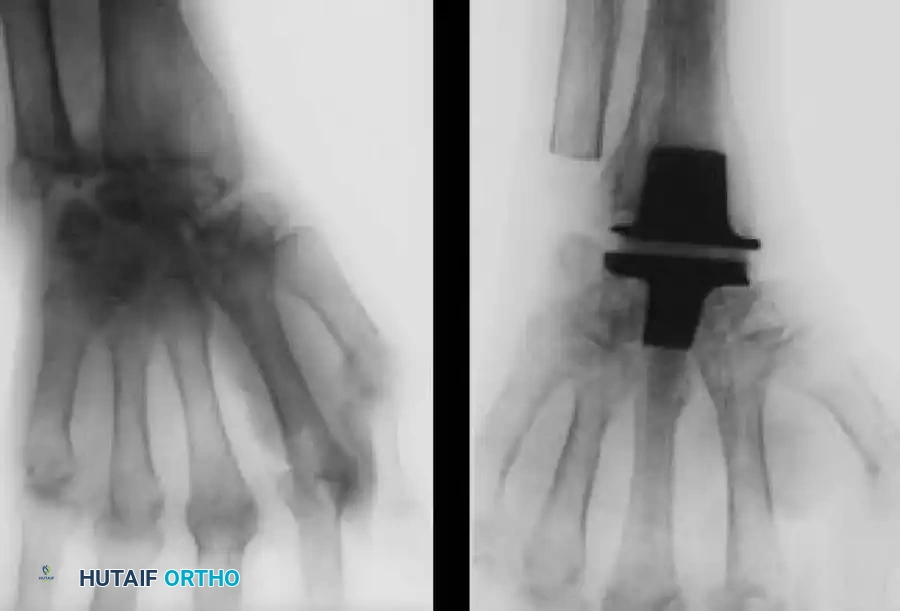
Total Wrist Arthroplasty (TWA)
Total joint arthroplasty offers the distinct advantages of preserving functional motion, providing a fixed fulcrum for tendon excursion, and achieving stable fixation. Modern designs are generally semi-constrained to allow for physiologic kinematics while preventing dislocation.
Implants such as the Meuli, Volz, and Biaxial wrist prostheses have shown excellent early to mid-term results in pain relief and motion preservation. However, the Achilles heel of TWA remains distal component loosening. The carpal bones in RA are often osteopenic and cystic, providing poor purchase for the distal pegs or screws.
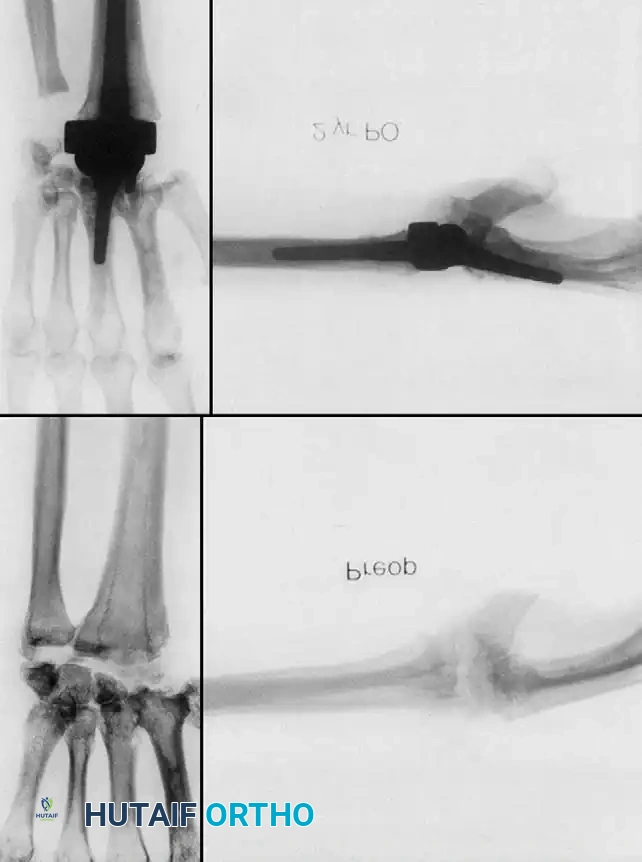
Complications, including distal loosening, subsidence, and periprosthetic fracture, lead to an overall revision rate of 9% to 35%. Adequate muscle balance, correctable preoperative wrist contractures, and meticulous surgical technique are absolute prerequisites for a successful TWA.

Wrist Arthrodesis
Total wrist arthrodesis is the gold standard for the young, high-demand patient, or the patient with profound bone loss, irreparable tendon ruptures, or failed arthroplasty. Fusion from the radius to the third metacarpal provides a stable, painless, and powerful wrist. The wrist is typically fused in 10 to 15 degrees of extension to maximize grip strength. While all radiocarpal and midcarpal motion is sacrificed, pronation and supination are preserved (provided the DRUJ is addressed via a Darrach or Sauvé-Kapandji procedure).
Postoperative Rehabilitation Protocols
Regardless of the procedure performed, meticulous postoperative care is essential to optimize outcomes in the rheumatoid patient.
- Immediate Postoperative Phase (0-14 days): The wrist is immobilized in a bulky compression dressing and plaster splint. Strict elevation is enforced to minimize edema. Active range of motion (ROM) of the fingers and thumb is encouraged immediately to prevent tendon adhesions and stiffness.
- Suture Removal (10-14 days): Wounds are inspected, and sutures are removed. Hematomas must be evacuated promptly to prevent infection and wound breakdown.
- Intermediate Phase (3-6 weeks): For synovectomies, the rigid splint is transitioned to a removable orthosis at 3 weeks, and active wrist ROM is initiated under the guidance of a hand therapist. For arthroplasties, immobilization may be maintained slightly longer depending on the implant stability, followed by a graduated ROM program.
- Long-Term: Strengthening is introduced cautiously. Patients must be educated on joint protection techniques to preserve the longevity of their reconstructions and protect adjacent joints from accelerated wear.
You Might Also Like