Medial Clavicle Resection for Chronic Sternoclavicular Joint Dislocation
Key Takeaway
Chronic sternoclavicular joint dislocations, particularly posterior variants, can cause significant mediastinal compression. When open reduction is unstable or unachievable, resection of the medial end of the clavicle provides a safe, definitive solution. This procedure relieves compressive symptoms such as dysphagia and dyspnea while preserving shoulder girdle function. Meticulous subperiosteal dissection and, when necessary, stabilization to the first rib ensure optimal biomechanical and cosmetic outcomes.
Comprehensive Introduction and Patho-Epidemiology
Epidemiology of Sternoclavicular Joint Dislocations
Dislocations of the sternoclavicular (SC) joint are exceedingly rare orthopedic entities, accounting for less than 3% of all injuries sustained by the shoulder girdle and less than 1% of all joint dislocations in the human body. The inherent rarity of this injury is largely attributable to the formidable strength of the surrounding ligamentous complex, which typically yields to fracture of the clavicle before permitting true articular displacement. When dislocations do occur, they are predominantly anterior, outnumbering posterior dislocations by a ratio of approximately 9:1. Posterior dislocations, while statistically scarce, are of paramount clinical significance due to the immediate anatomical proximity of the displaced medial clavicle to the critical neurovascular and visceral structures residing within the superior mediastinum.
The demographic distribution of these injuries heavily favors young, active males, typically occurring in the second to third decades of life. This age predilection coincides with the delayed ossification and fusion of the medial clavicular epiphysis, which is the last epiphysis in the body to close, often remaining unfused until the age of 25. Consequently, many presumed acute SC joint dislocations in this demographic are, upon advanced imaging or direct surgical exploration, revealed to be Salter-Harris type I or II physeal fractures. High-energy trauma is the most common etiology, with motor vehicle collisions, high-velocity sports impacts (such as in rugby, American football, and ice hockey), and falls from significant heights representing the primary mechanisms of injury.
Pathomechanics of Chronic Dislocation
The transition from an acute injury to a chronic dislocation is characterized by a complex cascade of biomechanical and histopathological alterations. In the acute setting, closed reduction is often attempted; however, the SC joint is notoriously unstable post-reduction, particularly in anterior dislocations, due to the extensive disruption of the anterior capsule and the costoclavicular ligamentous complex. When these injuries are neglected, misdiagnosed, or fail to maintain concentric reduction, they inexorably evolve into a chronic state. Chronicity in the context of the SC joint is generally defined as a dislocation persisting for greater than three weeks, at which point the surrounding soft tissues undergo severe contracture, and the joint space becomes obliterated by dense fibrotic scar tissue.
In chronic anterior dislocations, the medial clavicle remains prominent subcutaneously. Over time, the constant mechanical friction and altered kinematics lead to the degradation of the intra-articular fibrocartilaginous disc and the onset of rapidly progressive post-traumatic osteoarthritis. Conversely, chronic posterior dislocations involve the medial clavicle being persistently tethered in the retrosternal space. The pathomechanics here are far more insidious, as the displaced bone exerts continuous, unyielding pressure on the mediastinal structures. The surrounding hematoma organizes into a dense, fibrous pseudocapsule that often adheres directly to the adventitia of the great vessels, the pleura, or the tracheal wall, making delayed closed reduction impossible and rendering surgical intervention exceptionally hazardous.
Evolution from Acute to Chronic Pathology
The natural history of a chronic SC joint dislocation varies drastically depending on the direction of the displacement. Chronic anterior dislocations are frequently well-tolerated from a purely functional standpoint. Many patients maintain near-normal shoulder kinematics and strength, complaining primarily of the unsightly cosmetic deformity or localized, mechanically induced pain during terminal ranges of shoulder elevation or protraction. As the articular cartilage undergoes fibrillations and eventual eburnation, patients may develop symptomatic degenerative joint disease, characterized by crepitus, effusions, and pain that is refractory to non-steroidal anti-inflammatory drugs (NSAIDs) and physical therapy.
In stark contrast, the evolution of a chronic posterior dislocation is fraught with the potential for severe, life-altering morbidity. The continuous retrosternal displacement can lead to a progressive thoracic outlet syndrome or direct visceral compromise. Patients may experience a gradual onset of dyspnea, particularly when supine, due to tracheal compression. Dysphagia may develop secondary to esophageal impingement, while venous engorgement of the ipsilateral upper extremity or face can indicate partial occlusion of the brachiocephalic vein. The chronic pressure can also lead to the formation of vascular pseudoaneurysms, venous thrombosis, or erosive fistulas into the respiratory or gastrointestinal tracts. Given this grim natural history, the threshold for surgical intervention in chronic posterior dislocations is exceedingly low.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Sternoclavicular Articulation
The sternoclavicular joint represents the sole true synovial articulation linking the entire appendicular skeleton of the upper extremity to the axial skeleton. It is classified as a diarthrodial saddle joint, but its osseous architecture is inherently precarious. The articular surface of the medial clavicle is bulbous and disproportionately larger than the shallow, reciprocally shaped clavicular notch of the manubrium sterni. In fact, less than half of the medial clavicular articular surface is in contact with the manubrium at any given time in the resting anatomical position.
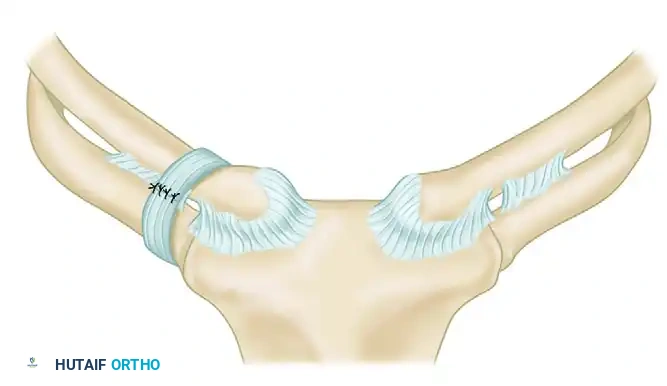
This profound osseous mismatch renders the joint inherently unstable from a purely structural standpoint. The upper portion of the medial clavicle extends significantly superior to the manubrium, providing attachment for the interclavicular ligament and the clavicular head of the sternocleidomastoid muscle. The articular surfaces are covered by hyaline cartilage, but the joint cavity itself is completely bisected by a dense, fibrocartilaginous intra-articular disc. This disc acts as a crucial shock absorber, mitigating the massive compressive forces transmitted from the upper extremity to the axial skeleton, and serves as a vital tether, resisting medial displacement of the clavicle over the manubrium.
Ligamentous Stabilizers and Capsular Anatomy
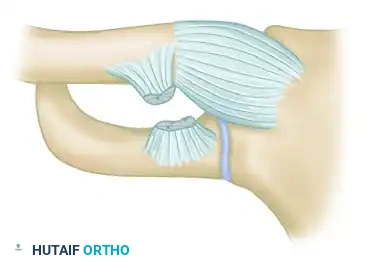
Given the lack of osseous congruency, the stability of the SC joint is entirely reliant upon a robust and complex network of capsuloligamentous restraints. The joint capsule itself is relatively thin inferiorly but is dramatically thickened anteriorly and posteriorly to form the anterior and posterior sternoclavicular ligaments. Biomechanical studies have unequivocally demonstrated that the posterior sternoclavicular ligament is the single most important structure for maintaining joint stability; it is the primary restraint against both anterior and posterior translation of the medial clavicle.
The costoclavicular ligament, also known as the rhomboid ligament, is a dense, bipartite structure that connects the inferior aspect of the medial clavicle to the superior surface of the first rib and its adjacent costal cartilage. It consists of an anterior fascicle, whose fibers run superiorly and laterally, and a posterior fascicle, whose fibers run superiorly and medially. This decussating arrangement allows the costoclavicular ligament to act as the primary restraint to superior displacement of the medial clavicle, counteracting the powerful upward pull of the sternocleidomastoid muscle. Finally, the interclavicular ligament spans the jugular notch, connecting the superomedial aspects of both clavicles and the superior manubrium, providing additional resistance to inferior depression of the distal shoulder girdle.
The Retrosternal Danger Zone and Neurovascular Proximity
A profound, three-dimensional understanding of the retrosternal anatomy is the most critical prerequisite for any surgeon undertaking a medial clavicle resection. The posterior aspect of the SC joint and the medial clavicle lie in perilous, millimeter-close proximity to some of the most vital anatomical structures in the human body, collectively referred to as the retrosternal "Danger Zone."
Directly posterior to the medial clavicle, separated only by the posterior joint capsule and the thin strap muscles (sternohyoid and sternothyroid), lie the great vessels. On the right side, the brachiocephalic (innominate) artery bifurcates into the right common carotid and right subclavian arteries directly behind the joint. Even more superficially, the right brachiocephalic vein lies mere millimeters from the posterior cortex of the clavicle. On the left side, the left brachiocephalic vein crosses the midline directly posterior to the manubrium and the left SC joint. Deeper to these vascular structures lie the trachea, the esophagus, the vagus nerve, the phrenic nerve, and the apical pleura of the lungs. The catastrophic potential of iatrogenic injury during dissection or osteotomy in this region cannot be overstated; a breach of the posterior periosteal envelope can result in instantaneous, massive, and potentially fatal hemorrhage.
Biomechanics of the Medial Clavicle
The clavicle acts as a dynamic strut, holding the glenohumeral joint away from the thorax to allow for maximum spatial mobility of the upper extremity. During normal shoulder kinematics, the SC joint undergoes significant multi-planar motion. For every 10 degrees of arm elevation, there are approximately 4 degrees of elevation at the clavicle. By the time the arm reaches maximum forward elevation, the medial clavicle has elevated up to 35 degrees, retracted posteriorly up to 35 degrees, and rotated posteriorly along its longitudinal axis by approximately 45 to 50 degrees.
Resection of the medial clavicle inherently alters this complex biomechanical linkage. However, clinical and cadaveric studies have shown that if the resection is strictly limited (typically to less than 1.5 to 2.0 cm) and the costoclavicular ligamentous complex is preserved or anatomically reconstructed, the remaining clavicular strut continues to function effectively. The preservation of the costoclavicular tether allows the clavicle to continue rotating and elevating without migrating superiorly or impinging against the manubrium. If the resection is excessive and violates the costoclavicular ligaments without subsequent stabilization to the first rib, the clavicle becomes a hypermobile, unstable segment, leading to severe dyskinesia, pain, and loss of shoulder power.
Exhaustive Indications and Contraindications
Clinical Presentation of Chronic Dislocations
The clinical presentation of a patient with a chronic SC joint dislocation is highly variable and directly correlates with the direction of the displacement. Patients with chronic anterior dislocations typically present with a visible, palpable bony prominence over the anteromedial chest wall. The overlying skin may be erythematous or thinned due to chronic friction. Functionally, these patients may report a clicking, popping, or grinding sensation during overhead activities, indicative of advanced intra-articular degeneration or subluxation over the manubrial edge. Pain is usually localized directly to the joint and is exacerbated by cross-body adduction or heavy lifting.
Conversely, patients with chronic posterior dislocations may present without an obvious cosmetic deformity, as the medial clavicle is hidden behind the sternum. Instead, their presentation is often dominated by symptoms of mediastinal compression. The orthopedic surgeon must maintain a high index of suspicion and specifically inquire about symptoms such as dysphagia (difficulty swallowing solid foods), dyspnea (shortness of breath, particularly when lying flat), stridor, or a persistent cough. Vascular compression may manifest as a feeling of fullness in the head, unilateral facial swelling, or venous engorgement and claudication of the ipsilateral arm. Neurological symptoms, including paresthesias or weakness radiating down the arm, may indicate secondary compression of the brachial plexus at the thoracic outlet.
Absolute and Relative Indications for Resection
The decision to proceed with a medial clavicle resection must be carefully weighed against the significant surgical risks. In the context of chronic posterior dislocations, the presence of any compressive mediastinal symptoms (respiratory, vascular, or esophageal) constitutes an absolute indication for surgical intervention. The risk of sudden, catastrophic vascular erosion or airway compromise in these patients far outweighs the risks of the surgical procedure itself. Even in asymptomatic chronic posterior dislocations, prophylactic resection is strongly considered in young, active patients due to the high likelihood of delayed complications and the progressive nature of the retrosternal fibrosis.
For chronic anterior dislocations, the indications are predominantly relative and heavily dependent on the patient's functional impairment and quality of life. Absolute indications in the anterior setting are rare but may include impending skin necrosis over a severely prominent medial clavicle. Relative indications include severe, intractable pain that has failed exhaustive conservative management (including activity modification, NSAIDs, and intra-articular corticosteroid injections), symptomatic post-traumatic osteoarthritis confirmed by imaging, and severe, unacceptable cosmetic deformity that causes significant psychological distress to the patient.
Contraindications to Surgical Intervention
Surgical intervention for chronic SC joint dislocations is not without its contraindications. Absolute contraindications include active, untreated local or systemic infection (such as osteomyelitis of the clavicle or systemic sepsis), and severe medical comorbidities that preclude the safe administration of general endotracheal anesthesia. A lack of cardiothoracic or vascular surgical backup in a facility is an absolute contraindication to attempting a medial clavicle resection for a posterior dislocation, given the potential for catastrophic intraoperative hemorrhage requiring immediate sternotomy.
Relative contraindications include asymptomatic chronic anterior dislocations in low-demand or elderly patients. In these scenarios, the functional deficit is minimal, and the risks of surgery, including postoperative instability, infection, and anesthetic complications, generally outweigh the potential benefits. Additionally, patients with profound psychiatric disorders or those who are unable or unwilling to comply with the strict, prolonged postoperative immobilization and rehabilitation protocols are poor candidates for this procedure, as non-compliance will inevitably lead to failure of the soft tissue reconstruction and recurrent instability.
| Indication Category | Anterior Dislocation | Posterior Dislocation |
|---|---|---|
| Absolute Indications | Impending skin necrosis, intractable pain failing >6 months conservative care. | Tracheal compression (dyspnea/stridor), esophageal compression (dysphagia), vascular compromise. |
| Relative Indications | Symptomatic osteoarthritis, unacceptable cosmetic deformity, popping/grinding limiting function. | Asymptomatic displacement in a young, high-demand athlete (prophylactic). |
| Absolute Contraindications | Active systemic/local infection, lack of cardiothoracic surgical backup. | Active systemic/local infection, lack of cardiothoracic surgical backup, inability to tolerate anesthesia. |
| Relative Contraindications | Asymptomatic presentation, elderly/low-demand patient, non-compliance with rehab. | Severe medical comorbidities, high surgical risk profile. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities
Standard orthogonal radiography is the initial step in evaluating any shoulder girdle trauma; however, the complex, overlapping osseous anatomy of the upper thorax renders standard anteroposterior (AP) views nearly useless for assessing the SC joint. The "serendipity view" is the most valuable plain radiograph. It is obtained with the patient supine, the cassette placed under the upper chest, and the X-ray beam angled 40 degrees cephalad, centered directly on the manubrium. In this view, an anteriorly dislocated clavicle will appear displaced superiorly relative to the interclavicular line, while a posteriorly dislocated clavicle will appear displaced inferiorly.
Despite the utility of the serendipity view, a high-resolution Computed Tomography (CT) scan without contrast is the absolute gold standard and is mandatory for preoperative planning in all chronic SC joint dislocations. Axial, coronal, and sagittal reconstructions, along with 3D volume-rendered images, provide unparalleled detail regarding the exact direction and magnitude of the dislocation, the presence of marginal fractures, and the degree of periarticular ossification or degenerative change. Most importantly, the CT scan allows the surgeon to precisely measure the distance between the posterior cortex of the displaced clavicle and the underlying great vessels, trachea, and esophagus.
Multidisciplinary Surgical Planning
The management of a chronic posterior SC joint dislocation requires a highly coordinated, multidisciplinary approach. The orthopedic surgeon must never operate in a silo when addressing this pathology. If the preoperative CT scan demonstrates the medial clavicle abutting or compressing the brachiocephalic vein, superior vena cava, or aortic arch, a CT Angiography (CTA) or formal arteriography/venography is indicated to rule out pseudoaneurysm formation, venous thrombosis, or direct adherence of the vessel wall to the bony cortex.
Furthermore, it is an absolute requirement that a cardiothoracic or vascular surgeon be formally consulted preoperatively and be immediately available (on standby) during the procedure. The operating room must be fully equipped for an emergency median sternotomy or thoracotomy. Blood products must be typed, crossed, and available in the operating room prior to the skin incision. This level of preparation is not overly cautious; it is a mandatory safety standard, as the massive hemorrhage resulting from an iatrogenic tear of the brachiocephalic vein can be fatal within minutes if not immediately controlled via a sternal splitting approach.
Anesthetic Considerations and Patient Positioning
The procedure is performed under general endotracheal anesthesia. Regional anesthesia (such as an interscalene block) may be used as an adjunct for postoperative pain control but is insufficient as the primary anesthetic modality due to the medial location of the incision and the potential need for airway management or emergency sternotomy. The endotracheal tube must be secured firmly to the contralateral side of the mouth and taped away from the operative field to ensure unobstructed access to the sternum and medial neck.
The patient is typically positioned in the beach-chair (semi-Fowler) position at approximately 30 to 45 degrees of elevation, or completely supine. A critical positioning maneuver is the placement of a vertical bump or rolled towel directly between the patient's scapulae. This allows both shoulders to fall posteriorly, which effectively opens the anterior aspect of the SC joint and pulls the medial clavicle slightly away from the mediastinum. The surgical preparation and draping must be extensive. It must expose the entire affected shoulder girdle, the ipsilateral neck, the anterior chest down to the costal margin, and the entire contralateral sternum and medial clavicle. This wide sterile field is essential to allow for an immediate, unhindered transition to a median sternotomy should a vascular catastrophe occur.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Subperiosteal Dissection
The surgical approach begins with a transverse incision, approximately 6 to 8 centimeters in length, centered directly over the medial end of the clavicle and extending slightly over the manubrium. The incision is carried down through the subcutaneous fat and the platysma muscle, maintaining meticulous hemostasis using electrocautery. Deep to the platysma, the investing layer of the deep cervical fascia is encountered, revealing the clavicular head of the sternocleidomastoid (SCM) muscle inserting on the superior aspect of the clavicle, and the clavicular origin of the pectoralis major muscle inferiorly.
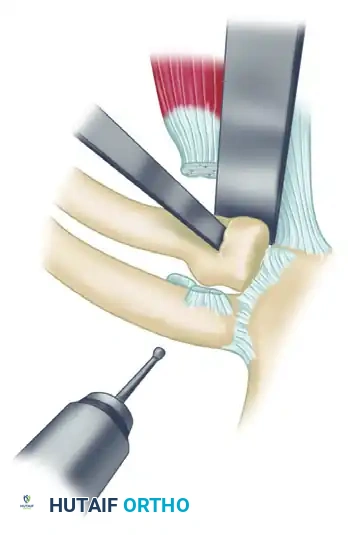
The periosteum of the medial clavicle is then incised longitudinally along its anterior midline. At this juncture, the most critical phase of the operation commences: the subperiosteal dissection. Using a sharp Cobb elevator or a specialized curved periosteal elevator (such as a Doyen rib elevator), the surgeon must meticulously peel the periosteum off the bone circumferentially. It is absolutely imperative that the surgeon stays strictly within the subperiosteal plane, particularly along the posterior cortex. The posterior periosteal sleeve is often the only physical barrier remaining between the surgeon's instruments and the thin-walled brachiocephalic vein. In chronic cases, dense fibrosis may make this elevation difficult, requiring patient, millimeter-by-millimeter dissection.
Osteotomy and Medial Clavicle Resection
Once the medial 3 centimeters of the clavicle have been completely freed from their periosteal envelope, the bone is grasped with a heavy bone-holding forceps, such as a Lewin clamp or a pointed reduction forceps. The clavicle is gently lifted anteriorly and superiorly, drawing it away from the retrosternal danger zone. A malleable retractor (e.g., a Copper retractor) is carefully slid behind the posterior cortex of the clavicle, inside the periosteal sleeve, to physically protect the mediastinal structures during the osteotomy.
The exact site of the osteotomy is determined by the integrity of the costoclavicular (rhomboid) ligaments. If the ligaments are intact, the resection must be strictly limited to the bone medial to their insertion (typically 1.5 to 2.0 cm). If the ligaments are completely destroyed, a slightly larger resection (up to 2.5 cm) may be performed to ensure adequate decompression. The osteotomy is performed using a narrow oscillating saw or a sharp osteotome, taking great care not to plunge posteriorly.
Following the primary resection, the remaining medial stump of the clavicle will present with a sharp, rectangular edge. If left unmodified, this anterosuperior corner will create an unsightly, painful subcutaneous prominence. Therefore, a rongeur or a high-speed burr must be used to aggressively bevel and contour the anterosuperior cortex, creating a smooth, rounded stump that sits flush beneath the soft tissues.
Periosteal Plication and Soft Tissue Management
After the resection and contouring are complete, the surgical bed is thoroughly irrigated, and absolute hemostasis is achieved. If the costoclavicular ligaments were intact and the remaining clavicular stump is determined to be completely stable (exhibiting no superior or anterior translation when the arm is manipulated), the surgeon may proceed directly to soft tissue closure. The empty periosteal sleeve, which previously housed the resected medial clavicle, is now a redundant, thick tube of fibrous tissue.
This periosteal sleeve must not be excised; rather, it is utilized as a vital biological stabilizer. Using heavy, non-absorbable sutures (e.g., #2 FiberWire or Ethibond), the empty periosteal sleeve is tightly plicated and imbricated upon itself, and then securely sutured over the raw bony end of the remaining clavicular stump. This robust "purse-string" or vest-over-pants closure acts as a dense, fibrous tether, effectively capping the bone and preventing any delayed anterior or superior migration of the clavicle into the subcutaneous tissues.
Management of Instability and First Rib Stabilization
In the majority of chronic dislocation cases, particularly those requiring a resection of 2.0 cm or more, the costoclavicular ligaments are found to be completely incompetent, attenuated, or intentionally resected. This leaves the remaining clavicular strut highly unstable. Without the downward tethering force of the costoclavicular ligaments, the unopposed pull of the sternocleidomastoid and trapezius muscles will inevitably draw the clavicular stump superiorly, leading to severe pain, cosmetic deformity, and functional impingement. In these scenarios, surgical stabilization of the medial clavicle to the first rib is an absolute necessity.
The anterior aspect of the first rib is carefully exposed, remaining strictly subperiosteal to avoid injury to the subclavian vein, which crosses the rib laterally. A stabilization graft is then selected; robust options include a strip of autologous fascia lata, a semitendinosus allograft, or heavy synthetic tape (e.g., 3-mm cotton Dacron tape). Two vertical drill holes are created in the medial stump of the clavicle. The graft is carefully passed under and around the first rib, brought superiorly, and passed through the drill holes in the clavicle.
While an assistant holds the clavicle firmly in an anatomically reduced, depressed position, the graft is tensioned and tied (or sutured to itself) in a figure-of-eight or cerclage configuration. This reconstruction effectively substitutes for the deficient costoclavicular ligaments. To further protect the repair, the clavicular head of the sternocleidomastoid muscle is often detached from its insertion, eliminating the primary superior deforming force. The wound is then closed in layers, meticulously reapproximating the platysma and skin.
Complications, Incidence Rates, and Salvage Management
Intraoperative Neurovascular Catastrophes
The most feared and potentially lethal complication associated with medial clavicle resection is massive intraoperative hemorrhage resulting from an iatrogenic injury to the retrosternal great vessels, most commonly the right brachiocephalic vein or the superior vena cava. While the exact incidence is exceedingly low (reported at less than 0.5% in experienced hands), the mortality rate of this specific complication is alarmingly high if not managed instantaneously. The mechanism of injury is almost universally a violation of the posterior periosteal sleeve during the dissection phase, or a plunging oscillating saw blade during the osteotomy.
If a massive venous or arterial bleed is encountered, the surgeon must immediately pack the retrosternal space tightly with laparotomy sponges and apply direct, unyielding manual pressure. No blind clamping should ever be attempted in this region, as it will inevitably result in further avulsion of the fragile vessels or collateral injury to the vagus or phrenic nerves. The standby cardiothoracic surgeon must be called into the room immediately, and the surgical team must rapidly transition to a median sternotomy to obtain proximal and distal control of the injured vessel and perform a definitive vascular repair.
Postoperative Instability and Recurrence
Postoperative instability of the remaining clavicular stump is the most common mechanical complication following medial clavicle resection, occurring in 5% to 15% of cases. This complication is almost entirely iatrogenic, resulting from a failure to recognize the incompetence of the costoclavicular ligaments during the index procedure, or a failure to perform an adequate first rib stabilization. When the clavicle is left un-tethered, the powerful superior pull of the sternocleidomastoid muscle causes the stump to migrate superiorly into the base of the neck.
Clinically, patients with postoperative instability present with a highly visible, painful, and mobile subcutaneous mass that exacerbates with any shoulder motion. They often report a feeling of profound weakness and fatigue in the shoulder girdle. Salvage management for this complication requires revision surgery. The surgical bed must be re-explored, the fibrotic scar tissue excised, and a formal, robust reconstruction of the costoclavicular tether must be performed using a massive structural allograft (such as an Achilles tendon bone-block allograft) passed around the first rib and secured through transosseous tunnels in the clavicle.
Cosmetic Deformity and Functional Deficits
Cosmetic dissatisfaction is a frequent, albeit less clinically severe, complication following medial clavicle resection. If the surgeon fails to adequately bevel and contour the anterosuperior cortex of the resected stump, the sharp bony edge will tent the skin, creating a visible and palpable spike that is particularly prominent in thin individuals. Furthermore, even with a perfect surgical technique, the excision of the medial clavicle inherently leaves a visible depression or asymmetry at the base of the neck, which must be discussed extensively with the patient during the preoperative informed consent process.
Functional deficits are relatively rare if the clavicle is properly stabilized. However, inadequate resection (removing less than 1.0 to 1.5 cm) can lead to a complication known as "stump impingement." During terminal shoulder protraction or cross-body adduction, the inadequately resected clavicular stump may persistently abut the manubrium, causing severe, localized pain and a mechanical block to motion. Salvage management for stump impingement requires a minor revision procedure to resect an additional 1.0 cm of bone, taking care not to violate the previously reconstructed costoclavicular tether.
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Massive Hemorrhage | < 0.5% | Violation of posterior periosteum, plunging saw. | Immediate packing, emergency median sternotomy, vascular repair. |
| Clavicular Instability | 5% - 15% | Failure to reconstruct incompetent costoclavicular ligaments. | Revision surgery with robust allograft stabilization to the first |
