Operative Repair and Reconstruction of the Thumb Ulnar Collateral Ligament
Key Takeaway
Surgical repair of the thumb ulnar collateral ligament (UCL) is indicated for acute complete ruptures, particularly those complicated by a Stener lesion. The procedure involves a dorsoulnar approach, identification and protection of the superficial radial nerve, and anatomic reattachment of the UCL to the proximal phalanx base using suture anchors or a pull-out wire. Provisional K-wire fixation of the metacarpophalangeal joint ensures construct stability during early healing.
INTRODUCTION AND BIOMECHANICAL PRINCIPLES
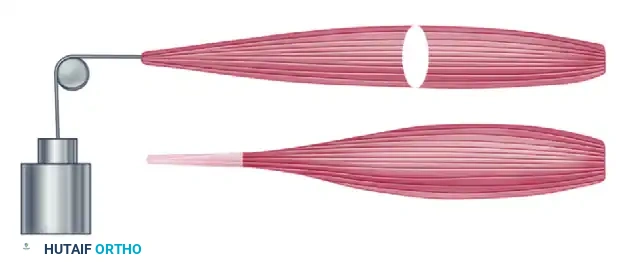
Rupture of the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint—historically termed "Gamekeeper's thumb" in the chronic setting and "Skier's thumb" in acute injuries—represents one of the most common and functionally debilitating ligamentous injuries of the hand. The thumb MCP joint is a diarthrodial ginglymus (hinge) joint, but its unique condylar anatomy permits a complex arc of flexion, extension, limited abduction, adduction, and pronation.
Stability of the thumb MCP joint is paramount for effective key pinch and cylindrical grasp. This stability is conferred by both static and dynamic restraints. The static stabilizers include the proper collateral ligament (PCL), the accessory collateral ligament (ACL), the volar plate, and the dorsal capsule. The dynamic stabilizers include the intrinsic muscles, primarily the adductor pollicis, and the extrinsic flexor and extensor tendons.
The proper UCL originates from the dorsal third of the metacarpal head and inserts onto the volar aspect of the proximal phalanx base. It is maximally taut in MCP joint flexion. Conversely, the accessory UCL lies volar to the proper ligament, inserting onto the volar plate, and is maximally taut in extension. A comprehensive understanding of this anatomy is critical, as surgical repair must restore the anatomical footprint to prevent chronic valgus instability and subsequent early-onset osteoarthritis.
Clinical Pearl: When examining a suspected UCL injury, testing must be performed in both full extension (isolating the accessory UCL and volar plate) and 30 degrees of flexion (isolating the proper UCL). A lack of a firm endpoint or valgus laxity greater than 30 degrees (or 15 degrees greater than the contralateral uninjured thumb) is diagnostic of a complete rupture.
PATHOPHYSIOLOGY: THE STENER LESION
The mechanism of injury typically involves a sudden, forceful radial deviation (valgus stress) and hyperextension of the thumb MCP joint. In complete ruptures, the ligament most commonly avulses from its distal insertion at the base of the proximal phalanx.
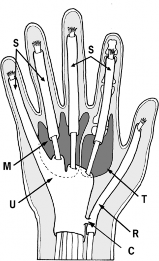
A critical pathoanatomic phenomenon associated with this injury is the Stener lesion. When the UCL avulses from the proximal phalanx, the adductor aponeurosis can interpose itself between the torn end of the ligament and its anatomical insertion site. The distal hemorrhagic end of the UCL flips proximally and superficially, resting over the adductor aponeurosis. Because the aponeurosis acts as a mechanical barrier, anatomical healing is biologically impossible without surgical intervention. The presence of a Stener lesion is an absolute indication for operative repair.
PREOPERATIVE PLANNING AND POSITIONING
Imaging
Standard posteroanterior, lateral, and oblique radiographs of the thumb are mandatory to rule out associated fractures, particularly avulsion fractures of the volar-ulnar base of the proximal phalanx. Stress radiography may be utilized but is often unnecessary if clinical examination is definitive, and it carries a theoretical risk of converting a non-displaced tear into a Stener lesion. Magnetic Resonance Imaging (MRI) or high-resolution ultrasound can definitively identify a Stener lesion if the clinical picture remains equivocal.
Patient Positioning and Anesthesia
- Anesthesia: The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia, depending on patient preference and comorbidities.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg (or 100 mm Hg above systolic blood pressure) after exsanguination with an Esmarch bandage to ensure a bloodless surgical field.
- Preparation: Standard surgical preparation and draping of the hand and forearm are performed.
SURGICAL APPROACH AND EXPOSURE
The Incision
The surgical approach must provide adequate exposure of the dorsoulnar aspect of the MCP joint while mitigating the risk of scar contracture.
- Make a slightly curved dorsoulnar longitudinal incision based radially, or alternatively, a bayonet-shaped incision.
- If utilizing the bayonet-shaped incision, place the transverse segment exactly at the joint level over the metacarpophalangeal joint to allow for optimal visualization of the capsular structures.
Nerve Identification and Protection
The terminal branches of the superficial radial nerve (SRN) are highly susceptible to iatrogenic injury during this approach. These branches innervate the lateral margins of the thumb pulp, and injury can result in debilitating neuromas or painful paresthesias.
- Carefully dissect through the subcutaneous tissue using blunt dissection (e.g., tenotomy scissors).
- Protect the superficial radial nerve terminal branches. Identify them as they pass distally on each side at the dorsolateral aspect of the metacarpophalangeal joint, deep to the subcutaneous fat.
- The nerve branches usually are retracted dorsally using silastic vessel loops, but they can be retracted volarly as well, depending on the specific anatomical location of the branch in relation to the incision.
Surgical Warning: Avoid aggressive traction on the superficial radial nerve branches. Neuropraxia of the SRN is one of the most common postoperative complications following UCL repair. Use gentle, dynamic retraction only when necessary.
DEEP DISSECTION AND PATHOLOGY IDENTIFICATION
Once the subcutaneous tissues are retracted, the dorsal expansion of the adductor aponeurosis comes into view.
- Inspect the area for a Stener lesion. If a Stener lesion is present, the ulnar collateral ligament can be seen with its distal hemorrhagic end flipped up in the subcutaneous tissue just proximal to the adductor aponeurosis. It often appears as a nodular, ecchymotic mass.
- Incise the adductor aponeurosis expansion longitudinally, parallel to the extensor pollicis longus (EPL) tendon.
- Carefully separate the thin tendinous sheets of the aponeurosis from the underlying joint capsule and the displaced UCL.
- Reflect the adductor aponeurosis volarly to fully expose the MCP joint capsule and the anatomical footprint of the UCL on the proximal phalanx.
ACUTE REPAIR BY SUTURE: SURGICAL TECHNIQUE
Joint Preparation and Provisional Fixation
Identify the ulnar collateral ligament and establish its failure site. In the vast majority of cases, this is an avulsion from the volar-ulnar base of the proximal phalanx.
- Debride the anatomical footprint on the proximal phalanx using a curette or a small rongeur to expose bleeding subchondral bone, which is essential for ligament-to-bone healing.
- In most cases, before the definitive repair, a 0.045-inch (1.14 mm) Kirschner wire (K-wire) is placed across the metacarpophalangeal joint to hold it in approximately 20 degrees of flexion and neutral adduction. This provisional fixation protects the repair from shear forces during the early phases of biological incorporation.
Fixation Options
If the ulnar collateral ligament has been detached from the proximal phalanx, it can be reinserted with a direct suture, a suture anchor, or a pull-out wire. While modern micro-suture anchors (1.3 mm to 2.0 mm) are frequently utilized for their biomechanical strength and lack of external hardware, the classic pull-out wire technique remains a highly reliable, time-tested method, particularly when suture anchors are unavailable or if the bone quality is poor.
The Pull-Out Wire Technique
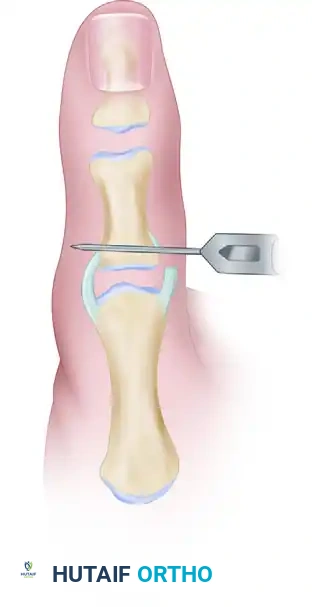
- To insert a pull-out wire, use a 0.035-inch or 0.045-inch Kirschner wire and drill a hole through the proximal end of the proximal phalanx, starting at the ulnar footprint and exiting on the radial cortex.
- Place a Bunnell or Krackow pull-out suture (using a non-absorbable or heavy absorbable suture, or a wire loop) through the avulsed, hemorrhagic end of the ligament.
- Pass the ends of the suture through the transosseous drill hole in the phalanx using a suture passer or a straight Keith needle.
- While holding the joint in slight flexion and applying a gentle ulnar-directed force to reduce the ligament to its footprint, tie the suture ends over a padded button on the radial side of the thumb.
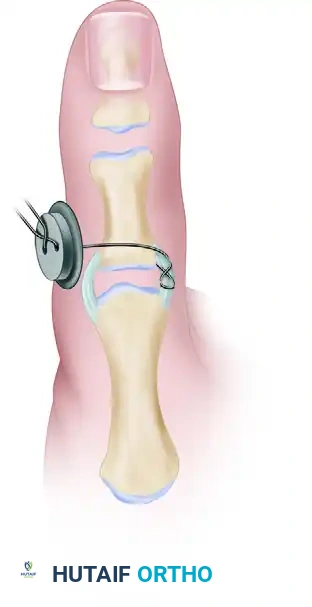
- Pass the twisted pull-out wire loop through the skin near the incision before final closure to facilitate removal in the clinic setting.
Alternative Transosseous Suture Technique
If the operating surgeon prefers not to use a Bunnell pull-out wire, or if one is unavailable, the following technique is highly recommended to achieve a knotless radial surface:
- After identifying the site of avulsion and preparing the bone bed, drill two divergent holes beginning on the ulnar base and exiting on the radial base of the proximal phalanx using a 0.035-inch Kirschner wire.
- Place a 3-0 Mersilene (or equivalent braided non-absorbable) grasping suture into the ligament.
- Pass the two limbs of the suture through the separate drill holes.
- With adequate dorsal exposure, tie this suture directly over the radial aspect of the proximal phalanx bone bridge for permanent placement.
Pitfall: When tying sutures over the radial cortex, ensure that the extensor mechanism and the radial collateral ligament are not inadvertently captured in the knot, which could lead to severe postoperative stiffness.
Management of Bony Avulsions
When the ligament disruption is associated with a significant avulsion bone fragment, the fragment must be assessed for size and comminution.
- If the tear is complete and the bone fragment is displaced but large enough to accept hardware, fixation with a small caliber Kirschner wire or even a minifragment screw (1.0 mm to 1.5 mm) is possible.
- Tension band wiring, although technically demanding and not part of routine management, may be utilized for larger fragments and precludes the use of a pull-out wire.
- If the fragment is small, comminuted, or osteoporotic, it should be excised, and the ligament advanced and repaired directly to the bone using the suture techniques described above.
CHRONIC ULNAR COLLATERAL LIGAMENT RECONSTRUCTION
In cases of chronic instability (typically presenting >6 weeks post-injury), direct repair is often impossible due to ligamentous retraction, atrophy, and poor tissue quality. Procedures designed to restore range of motion and stability for chronic ulnar collateral ligament injuries are numerous.
Stability at long-term follow-up has been associated with “anatomical repairs” in which the graft is directed to reconstruct both the proper and accessory ulnar collateral ligament limbs. We favor more anatomical type repairs such as those described by Glickel et al., Jobe, and others.
Graft Selection and Routing
- Graft Choice: A palmaris longus autograft is preferred due to its expendability and ideal diameter. If the palmaris longus is absent, common alternative autogenous sources include a portion of the flexor carpi radialis (FCR) or a toe extensor tendon.
- Technique: Drill holes are created at the anatomical origins and insertions of the UCL (the dorsal third of the metacarpal head and the volar-ulnar base of the proximal phalanx). The graft is routed in a figure-of-eight or a triangular configuration to recreate the vectors of both the proper and accessory ligaments.
- Fixation: Tendon anchor systems such as interference tenodesis screws and suture anchors are preferred by some surgeons for early construct stability. However, the adjunct provisional metacarpophalangeal joint stabilization in 20 degrees of flexion with Kirschner wires probably is sufficient during the graft incorporation period.
CLOSURE AND SOFT TISSUE BALANCING
Meticulous closure is essential to restore the dynamic stability of the thumb.
- With either the acute repair or chronic reconstruction technique, ensure the metacarpophalangeal joint is transfixed with a Kirschner wire in slight flexion and neutral adduction.
- Repair the dorsal capsule and the volar plate using 4-0 absorbable sutures to strengthen the repair further and prevent volar subluxation.
- Repair the dorsal adductor aponeurosis meticulously. This step is critical, as failure to restore the aponeurosis can lead to weakness in pinch grip and an extensor lag.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable monofilament sutures (e.g., 5-0 nylon).
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for ligamentous healing with the prevention of joint stiffness.
- Immediate Postoperative Phase: The thumb is immobilized in a bulky, well-padded thumb spica splint, maintaining the first web space to prevent adductor contracture.
- Immobilization: A custom-molded removable thermoplastic thumb spica brace or a fiberglass cast is worn for 3 to 4 weeks for comfort and protection.
- Hardware Removal: The pull-out wire (if utilized) and the transarticular Kirschner wire are removed in the clinic at 4 to 6 weeks postoperatively.
- Rehabilitation: Once the K-wire is removed, active range-of-motion (AROM) exercises for the MCP and interphalangeal (IP) joints are initiated. The spica splint is worn between exercise sessions and at night for an additional 2 to 4 weeks.
- Strengthening: Gentle strengthening, including putty exercises for key pinch and grip, begins at 6 to 8 weeks. Unrestricted heavy activity and sports are generally permitted at 10 to 12 weeks, though a protective playing splint may be recommended for contact sports up to 6 months postoperatively.
By adhering to strict anatomical principles, protecting the superficial radial nerve, and ensuring robust osseous integration of the ligament, surgeons can reliably restore stability and function to the thumb MCP joint, allowing patients to return to their highest level of occupational and athletic performance.
📚 Medical References
- ulnar collateral ligament injuries of the elbow in athletes, Am J Sports Med 28:16, 2000.
- Azar FM, Bernstein S, Kvitne RS, et al: Shoulder and elbow injuries in the throwing athlete. In Koval KJ, ed: Orthopaedic Knowledge Update 7, Rosemont, Ill, 2002, American Academy of Orthopaedic Surgeons. Baker CL, Brooks AA: Arthroscopy of the elbow, Clin Sports Med 15:261, 1996.
- Baker CL Jr, Jones GL: Arthroscopy of the elbow, Am J Sports Med 27:251, 1999.
- Baumgard SH, Schwartz DR: Percutaneous release of the epicondylar muscles for humeral epicondylitis, Am J Sports Med 10:233, 1982.
- Boyd HB, McLeod AC Jr: Tennis elbow, J Bone Joint Surg 55A:1183, 1973.
- Burnham R, Gregg R, Healy P, et al: The effectiveness of topical diclofenac for lateral epicondylitis, Clin J Sports Med 8:78, 1998.
- Chung B, Wiley JP: Effectiveness of extracorporeal shock wave therapy in the treatment of previously untreated lateral epicondylitis: a randomized controlled trial, Am J Sports Med 33:461, 2005.
- Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athletes’ elbow, Instr Course Lect 48:383, 1999.
- Coel M, Yamada CY, Ko J: MR imaging of patients with lateral epicondylitis of the elbow (tennis elbow): importance of increased signal of the anconeus muscle, AJR Am J Roentgenol 161:1019, 1993.
- Cohen MS, Hastings H II: Posttraumatic contracture of the elbow: operative release using a lateral collateral ligament sparing approach, J Bone Joint Surg 80B:805, 1998.
- Cohen MS, Hastings H II: Operative release for elbow contracture: the lateral collateral ligament sparing approach, Orthop Clin North Am 30:133, 1999.
- Conway JE, Jobe FW, Glousman RE, et al: Medial instability of the elbow in throwing athletes: treatment by repair or reconstruction of the ulnar collateral ligament, J Bone Joint Surg 74A:67, 1992.
- Coonrad RW, Hooper WR: Tennis elbow: its course, natural history, conservative and surgical management, J Bone Joint Surg 55A:1177, 1973.
- Demirtas RN, Oner C: The treatment of lateral epicondylitis by iontophoresis of sodium salicylate and sodium diclofenac, Clin Rehabil 12:23, 1998.
- Dlabach JA, Baker CL: Lateral and medial epicondylitis in the overhead athletes, Oper Tech Orthop 11:46, 2001.
- Duke JB, Tessler RH, Dell PC: Manipulation of the stiff elbow with the patient under anesthesia, J Hand Surg 16A:19, 1991.
- Edwards SG, Calandruccio JH: Autologous blood injections for refractory lateral epicondylitis, J Hand Surg 28:272, 2003.
- Enzenauer RJ, Nordstrom DM: Anterior interosseous nerve syndrome associated with forearm band treatment of lateral epicondylitis, Orthopedics 14:788, 1991.
- Fridén J, Lieber RL: Physiologic consequences of surgical lengthening of extensor carpi radialis brevis muscle-tendon junction for tennis elbow, J Hand Surg 19A:269, 1994.
- Gabel GT, Morrey BF: Operative treatment of medial epicondylitis: infl uence of concomitant ulnar neuropathy at the elbow, J Bone Joint Surg 77A:1065, 1995.
- Galloway M, DeMaio M, Mangine R: Rehabilitative techniques in the treatment of medial and lateral epicondylitis, Orthopedics 15:1089, 1992.
- Gellman H: Tennis elbow (lateral epicondylitis), Orthop Clin North Am 23:75, 1992.
- Glynn JJ, Niebauer JJ: Flexion and extension contracture of the elbow: surgical management, Clin Orthop Relat Res 117:289, 1976.
- Hamilton CD, Glousman RE, Jobe FW, et al: Dynamic stability of the elbow: electromyographic analysis of the fl exor pronator group and the extensor group in pitchers with valgus instability, J Shoulder Elbow Surg 5:347, 1996.
- Husband JB, Hastings H II: The lateral approach for operative release of post-traumatic contracture of the elbow, J Bone Joint Surg 72A:1353, 1990.
- Jupiter JB, O’Driscoll SW, Cohen MS: The assessment and management of the stiff elbow, Instr Course Lect 52:93, 2003.
- Kannus P, Jozsa L: Histopathological changes preceding spontaneous rupture of a tendon: a controlled study of 891 patients, J Bone Joint Surg 73A:1507, 1991.
- Kelley JD, Lombardo SJ, Pink M, et al: Electromyographic and cinematographic analysis of elbow function in tennis players with lateral epicondylitis, Am J Sports Med 22:359, 1994.
- Kraushaar BS, Nirschl RP, Cox W: A modifi ed lateral approach for release of posttraumatic elbow fl exion contracture, J Shoulder Elbow Surg 8:476, 1999.
- Kuklo TR, Taylor KF, Murphy KP, et al: Arthroscopic release for lateral epicondylitis: a cadaver model, Arthroscopy 259:15, 1999.
- Kurvers H, Verhaar J: The results of operative treatment of medial epicondylitis, J Bone Joint Surg 77A:1374, 1995.
- Labelle H, Guibert R, Joncas J, et al: Lack of scientifi c evidence for the treatment of lateral epicondylitis of the elbow: an attempted meta-analysis, J Bone Joint Surg 74B:646, 1992.
- Mills GP: The treatment of “tennis elbow,” BMJ 1:12, 1928.
- Morrey BF: Post-traumatic contracture of the elbow, J Bone Joint Surg 72A:601, 1990.
- Morrey BF: Surgical treatment of extraarticular elbow contracture, Clin Orthop Relat Res 370:57, 2000.
- Morrey BF: The post-traumatic stiff elbow, Clin Orthop Relat Res 431:26, 2005.
- Morrey BF, Askew LJ, An KN, et al: Rupture of the distal tendon of the biceps brachii: a biomechanical study, J Bone Joint Surg 67A:418, 1985.
- Murphy BJ: MR imaging of the elbow, Radiology 184:525, 1992.
- Nathan PA: Surgical treatment of ulnar nerve entrapment at the elbow, J Hand Surg 18B:245, 1992.
- Newey ML, Patterson MH: Pain relief following tennis elbow release, J R Coll Surg Edinb 39:60, 1994.
- Nicola TL: Elbow injuries in athletes, Prim Care 19:283, 1992.
- Nirschl RP: Elbow tendinosis/tennis elbow, Clin Sports Med 11:851, 1992.
- Nirschl RP: Lateral extensor release for tennis elbow, J Bone Joint Surg 76A:951, 1994.
- Nirschl RP, Ashman ES: Tennis elbow tendinosis (epicondylitis), Instr Course Lect 53:587, 2004.
- Noteboom T, Cruver R, Keller J, et al: Tennis elbow: a review, J Orthop Sports Phys Ther 19:357, 1994.
- O’Driscoll SW, Morrey BF: Arthroscopy of the elbow: diagnostic and therapeutic benefi ts and hazards, J Bone Joint Surg 74A:84, 1992.
- Ollivierre CO, Nirschl RP, Pettrone FA: Resection and repair for medial tennis elbow: a prospective analysis, Am J Sports Med 23:214, 1995.
- Organ SW, Nirschl RP, Kraushaar BS, et al: Salvage surgery for lateral tennis elbow, Am J Sports Med 25:746, 1997.
- Osgood RB: Radiohumeral bursitis, epicondylitis, epicondylalgia (tennis elbow), Arch Surg 4:420, 1922.
- Peppers TA, Jobe CM, Dai QG, et al: Fixation of humeral prostheses and axial micromotion, J Shoulder Elbow Surg 7:414, 1998.
- Porretta CA, Janes JM: Epicondylitis of the humerus, Mayo Clin Proc 33:303, 1958.
- Posch JN, Goldberg VM, Larrey R: Extensor fasciotomy for tennis elbow: a long-term follow-up study, Clin Orthop Relat Res 135:179, 1978.
- Regan W, Wold LE, Coonrad R, et al: Microscopic histopathology of chronic refractory lateral epicondylitis, Am J Sports Med 20:746, 1992.
- Runge F: Zur Genese und Behandlung des Schreibekrampfes, Berl Klin Wochenschr 10:245, 1873.
- Schenck RC Jr, Athanasiou KA, Constantinides G, et al: A biomechanical analysis of articular cartilage of the human elbow and potential relationship to
You Might Also Like