Comprehensive Management of Pediatric Physeal and Forearm Fractures
Key Takeaway
The management of pediatric physeal and forearm fractures requires a profound understanding of skeletal immaturity, remodeling potential, and growth plate biomechanics. This comprehensive guide details evidence-based surgical protocols for complex pediatric trauma, including Salter-Harris injuries, Monteggia fracture-dislocations, and open fractures. By mastering elastic stable intramedullary nailing (ESIN) and physeal bar resections, orthopedic surgeons can optimize functional outcomes and prevent devastating growth arrests in the skeletally immature patient.
Introduction to Pediatric Skeletal Trauma
The management of pediatric fractures demands a paradigm entirely distinct from adult traumatology. The presence of the physis (growth plate), a thick and osteogenic periosteum, and the profound capacity for skeletal remodeling dictate both the conservative and operative algorithms employed by the orthopedic surgeon. Drawing upon decades of foundational literature—from the classic classifications of Salter and Harris to the modern intramedullary techniques pioneered by Lascombes and the Nancy group—this masterclass delineates the operative principles for managing complex pediatric physeal injuries, open fractures, and intricate forearm fracture-dislocations.
Physeal Injuries and Growth Arrest
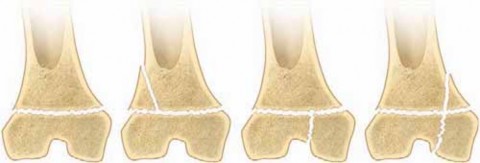
The physis is the weakest biomechanical link in the pediatric musculoskeletal system, failing under tension or shear forces before the adjacent ligaments or metaphyseal bone. While the Salter-Harris classification remains the universal language for these injuries, Peterson’s epidemiological and biomechanical additions—particularly regarding compression injuries (Type V) and previously unclassified patterns—highlight the nuanced reality of physeal trauma.
Biomechanics and Pathophysiology
The growth plate is composed of distinct histological zones: the resting, proliferative, hypertrophic, and provisional calcification zones. Most fractures propagate through the zone of hypertrophy, where the extracellular matrix is abundant but structurally weakest. However, compression forces can crush the resting and proliferative zones, leading to irreversible cellular death and subsequent osseous bridge (bar) formation.
Clinical Pearl: Always maintain a high index of suspicion for Type V compression injuries in high-energy axial load mechanisms. Initial radiographs are often deceptively normal. Contralateral comparative views and early MRI (as advocated by Smith et al.) are invaluable for detecting occult physeal edema and preventing delayed diagnosis of growth arrest.
Differentiating Trauma from Developmental Variants
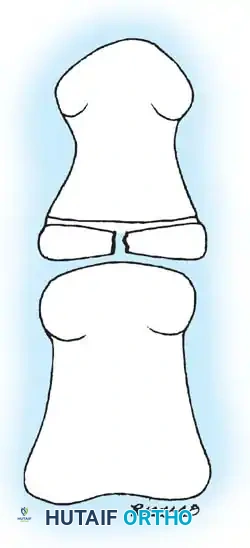
A critical skill for the pediatric orthopedic surgeon is distinguishing true physeal fractures from normal developmental variants. Misinterpretation can lead to unnecessary immobilization or unwarranted surgical intervention.
As illustrated above, fissuring of the physis in the proximal phalanx of the great toe is a documented developmental disorder that mimics a fracture line. This stereoradiographic phenomenon represents irregular ossification rather than a traumatic cleft. Clinical correlation—specifically the absence of localized tenderness, swelling, or a compatible mechanism of injury—is paramount in ruling out a true Salter-Harris injury.
Surgical Management of Partial Growth Arrest (Physeal Bar Resection)
When a physeal bar forms, it tethers growth, resulting in angular deformity, limb-length discrepancy, or both. The pioneering work of Langenskiöld and Bright established the operative principles for bar resection and interposition.
Indications for Resection:
* The patient has at least 2 years of remaining growth (or >2 cm of projected growth).
* The physeal bar involves less than 40-50% of the total cross-sectional area of the physis.
* Concomitant angular deformity is less than 15 degrees (if greater, a simultaneous corrective osteotomy is required).
Preoperative Planning:
Advanced imaging is mandatory. CT or MRI mapping (utilizing the Carlson and Wenger method) allows the surgeon to construct a 3D model of the bar, determining its exact location (peripheral vs. central) and volume.
Surgical Technique: Step-by-Step
1. Positioning and Approach: Position the patient supine on a radiolucent table. Use a tourniquet. The approach is dictated by the bar's location. For a peripheral bar, a direct approach over the tether is used. For a central bar, a metaphyseal window is created to access the bar from above, preserving the intact peripheral physis.
2. Metaphyseal Windowing (Central Bars): Use a high-speed burr to create a cortical window in the metaphysis. Carefully curette the cancellous bone to expose the sclerotic bone of the physeal bar.
3. Bar Resection: Under direct visualization and fluoroscopic guidance, resect the osseous bridge using small curettes and a high-speed burr. The resection must continue until normal, pearly-white, cartilaginous physeal tissue is visualized circumferentially.
4. Verification: Insert a dental mirror or a small arthroscope into the cavity to ensure complete excision.
5. Interposition Material: To prevent recurrence, the dead space must be filled. Autologous fat (harvested from the gluteal fold) is the gold standard, as established by Langenskiöld. Cranioplast (methylmethacrylate) or bone wax can also be used, though fat is preferred for its biological compatibility and lower risk of extrusion.
6. Closure: The metaphyseal window is left open or loosely covered with periosteum to prevent pressure buildup.
Pediatric Open (Compound) Fractures
The management of open fractures in children differs subtly from adults. While the Gustilo-Anderson classification is applied, the robust pediatric periosteum and superior vascularity often yield lower infection rates and faster union.
Timing of Debridement
Historically, the "6-hour rule" dictated emergent surgical debridement. However, landmark studies by Skaggs et al. demonstrated that a delay of up to 24 hours in the surgical debridement of pediatric open fractures (specifically Gustilo Types I and II) does not significantly increase the infection rate, provided that intravenous antibiotics are administered immediately upon presentation.
Surgical Warning: This delayed approach does NOT apply to Gustilo Type III fractures, highly contaminated wounds (e.g., farm injuries, marine environments), or cases with vascular compromise. These remain absolute surgical emergencies.
Operative Protocol
- Irrigation and Debridement: Perform radical excision of all necrotic skin, fat, fascia, and muscle. Deliver the fracture ends from the wound to ensure thorough intramedullary irrigation. Use 3 to 9 liters of normal saline, depending on the Gustilo grade.
- Stabilization: Unlike adults where rigid intramedullary nailing or plating is standard, pediatric open fractures (especially of the tibia and forearm) are highly amenable to Elastic Stable Intramedullary Nailing (ESIN) or external fixation. ESIN avoids the periosteal stripping associated with plating, preserving the vital blood supply necessary for combating infection and promoting union.
Hand and Wrist Trauma in the Skeletally Immature
Fractures of the pediatric hand and wrist are ubiquitous, yet certain patterns demand specialized attention to prevent long-term disability.
Distal Radius Physeal Fractures
The distal radius physis contributes 75% of the longitudinal growth of the radius. Salter-Harris II fractures are the most common. While remodeling potential is massive in the sagittal plane, coronal plane translation and rotational malalignments remodel poorly.
* Pitfall: Repeated closed reduction attempts significantly increase the risk of iatrogenic physeal damage and subsequent premature closure. If an acceptable reduction cannot be achieved on the first or second attempt, proceed to closed reduction and percutaneous pinning (CRPP) with smooth K-wires.
Pediatric Scaphoid Fractures
Unlike adults, where waist fractures predominate, pediatric scaphoid fractures frequently involve the distal pole. However, as the child approaches adolescence, the fracture pattern shifts toward the waist and proximal pole, increasing the risk of nonunion.
* Management: Cast immobilization is sufficient for acute, non-displaced fractures. For displaced fractures or established nonunions (as discussed by Mintzer and Waters), operative intervention via a volar approach, utilizing non-vascularized bone grafting and headless compression screw fixation, is highly successful.
Complex Metacarpophalangeal (MCP) Dislocations
The "Kaplan lesion" represents a complex, irreducible dorsal dislocation of the MCP joint, most commonly affecting the index finger.
* Pathoanatomy: The metacarpal head is buttonholed between the lumbrical (radially) and the flexor tendons (ulnarly). The volar plate is avulsed proximally and becomes interposed between the base of the proximal phalanx and the metacarpal head, blocking closed reduction.
* Surgical Approach: A volar approach is classically described, but carries a high risk of iatrogenic injury to the radial digital nerve, which is tented superficially over the metacarpal head. Many modern surgeons prefer a dorsal approach, which allows direct longitudinal splitting of the volar plate to release the metacarpal head safely.
Complex Pediatric Forearm Fractures
Forearm fractures account for a massive proportion of pediatric trauma. While conservative management with closed reduction and casting is the mainstay, the limits of acceptable angulation decrease as the child ages.
Plastic Deformation
Plastic bowing of the forearm occurs when the bone is stressed beyond its elastic limit but below its failure point. Microfractures occur on the concave side. If bowing exceeds 20 degrees, it severely restricts pronation and supination.
* Correction: Requires sustained, heavy manual pressure (often over a fulcrum) under general anesthesia to break the microfractures and restore alignment. If closed correction fails, osteoclasis or operative stabilization is required.
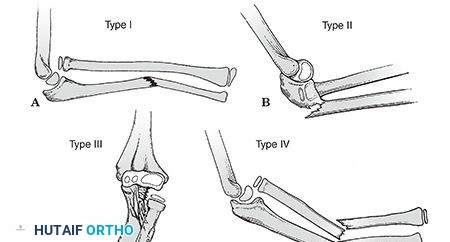
The Monteggia Lesion
Described by Bado, the Monteggia lesion is a fracture of the ulnar shaft with a concomitant dislocation of the radial head.
* The Golden Rule: The radiocapitellar line must bisect the capitellum in every radiographic view. Failure to recognize a radial head dislocation leads to chronic pain, restricted motion, and progressive valgus deformity.
* Operative Management: The key to reducing the radial head is restoring the anatomic length and alignment of the ulna. In children, if closed reduction of the ulna is unstable, intramedullary fixation of the ulna with a thick elastic nail or a smooth Steinmann pin is usually sufficient. Once the ulna is out to length, the radial head typically reduces spontaneously.
* Chronic/Missed Monteggia: Requires a complex reconstruction (e.g., Bell Tawse procedure), involving an ulnar opening wedge osteotomy to restore length and angulation, open reduction of the radial head, and annular ligament reconstruction using a slip of the triceps tendon.
Elastic Stable Intramedullary Nailing (ESIN) of the Forearm
When both-bone forearm fractures are unstable, irreducible, or occur in adolescents nearing skeletal maturity, ESIN is the gold standard.
Biomechanics of ESIN:
ESIN relies on the principle of three-point fixation. Two pre-bent titanium or stainless steel nails are inserted into the medullary canals. The elastic recoil of the nails against the inner cortical walls provides rotational and angular stability while allowing micromotion that stimulates robust callus formation.
Surgical Technique: Step-by-Step
1. Preoperative Planning: Measure the narrowest diameter of the diaphysis (the isthmus) of both the radius and ulna. The nail diameter should be approximately 40% of the canal diameter (typically 2.0 mm to 2.5 mm for pediatric forearms).
2. Positioning: Supine on a radiolucent hand table.
3. Ulnar Nailing:
* Make a 1 cm incision over the lateral aspect of the proximal ulna, 1-2 cm distal to the olecranon apophysis.
* Use an awl to breach the cortex at a 45-degree angle to the shaft.
* Pre-bend the nail to create a gentle bow (the apex of the bow should rest at the fracture site).
* Advance the nail across the fracture site under fluoroscopy.
4. Radial Nailing:
* Make a 1 cm incision over the lateral aspect of the distal radius, taking extreme care to protect the superficial branch of the radial nerve.
* Enter the bone proximal to the distal radial physis (Lister's tubercle can serve as a landmark, entering just radial to it).
* Advance the pre-bent nail proximally.
* Crucial Step: The bows of the radial and ulnar nails must face away from each other (divergent) to maximize the interosseous space and restore the radial bow. Failure to restore the radial bow will result in a permanent loss of pronation/supination.
5. Nail Trimming: Cut the nails leaving 1-2 cm protruding from the cortex to facilitate future removal. Bend the tips slightly away from the skin to prevent irritation, but ensure they are buried deep to the subcutaneous tissue.
6. Postoperative Protocol: A long-arm splint is applied for 2-3 weeks for soft tissue rest, followed by a removable brace. Range of motion exercises for the elbow and wrist are initiated early. Nails are typically removed at 6 to 9 months post-operatively, once complete cortical consolidation is visible on radiographs.
Conclusion
The operative management of pediatric orthopedic trauma is an exacting science that marries biomechanical principles with a profound respect for the biological potential of the growing skeleton. Whether executing a meticulous physeal bar resection, navigating the complexities of a Monteggia fracture-dislocation, or deploying elastic nails for diaphyseal stability, the surgeon's goal remains constant: to restore anatomy, preserve the physis, and facilitate the child's return to unimpeded growth and function. Mastery of these techniques, grounded in the foundational literature, is the hallmark of excellence in pediatric orthopedic surgery.
You Might Also Like