Mastering the Operative Management of Olecranon Fractures
Key Takeaway
Olecranon fractures disrupt the extensor mechanism of the elbow and often require precise open reduction and internal fixation (ORIF) to restore articular congruity and triceps function. Surgical options include tension band wiring, intramedullary screw fixation, plate osteosynthesis, and fragment excision. The choice of technique depends on fracture comminution, patient age, and joint stability. Early active mobilization is critical to prevent postoperative stiffness and ensure optimal functional recovery.
RADIUS AND ULNA: OPERATIVE PRINCIPLES
Fractures of the forearm bones in adults frequently demand surgical intervention to restore the complex biomechanics of the upper extremity. Surgical indications encompass fractures of the olecranon, the head or neck of the radius, and the proximal third of the ulna associated with dislocation of the radial head (Monteggia lesions). Furthermore, operative management is routinely indicated for isolated displaced fractures of the ulnar or radial shafts, as well as diaphyseal fractures involving both bones.
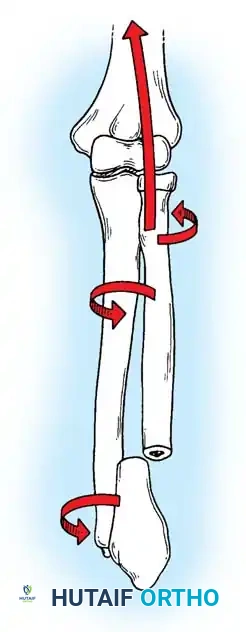
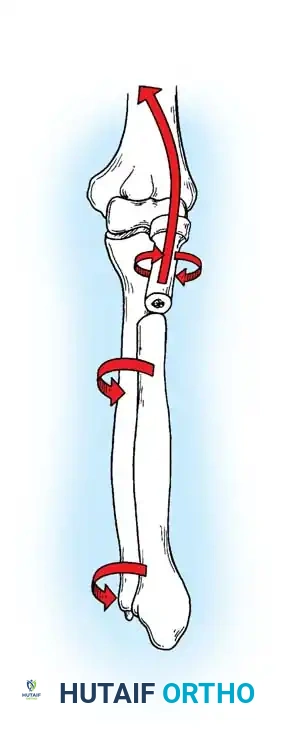
The primary goal of surgical intervention in the forearm and elbow is the exact restoration of anatomical alignment, axial length, and rotational stability. In the proximal ulna, the olecranon forms the greater sigmoid notch, articulating with the trochlea of the humerus. Any disruption here not only compromises the extensor mechanism but also threatens the intrinsic stability of the elbow joint.
FRACTURES OF THE OLECRANON
In adults, displaced fractures of the olecranon necessitate open reduction and internal fixation (ORIF). Because the olecranon is an intra-articular structure, reduction must be anatomically exact. Any residual irregularity or step-off of the articular surface inevitably leads to limited motion, delayed functional recovery, and early-onset post-traumatic osteoarthritis.
The chosen fixation construct must be biomechanically robust enough to withstand the powerful tensile forces of the triceps brachii. Rigid fixation allows for the initiation of gentle, active range-of-motion (ROM) exercises well before radiographic evidence of complete osseous union is visible.
Mechanism of Injury
Olecranon fractures typically result from two distinct mechanisms:
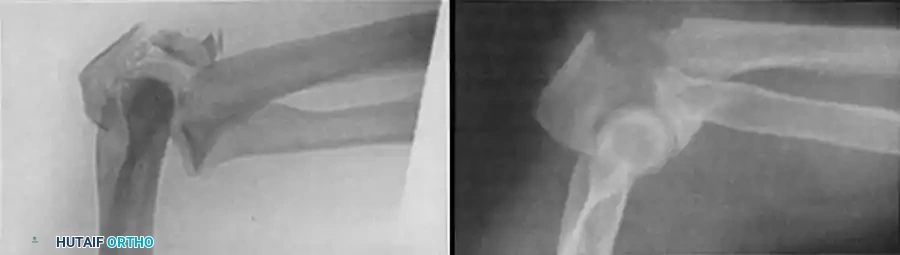
1. Direct Trauma: A direct blow or fall onto the tip of the elbow. This mechanism frequently results in comminuted fracture patterns and significant articular cartilage damage.
2. Indirect Trauma: A fall onto a partially flexed elbow accompanied by a sudden, forceful contraction of the triceps muscle. This indirect force avulses the olecranon, typically resulting in a transverse or oblique fracture pattern with a clean articular break.
Classification of Olecranon Fractures
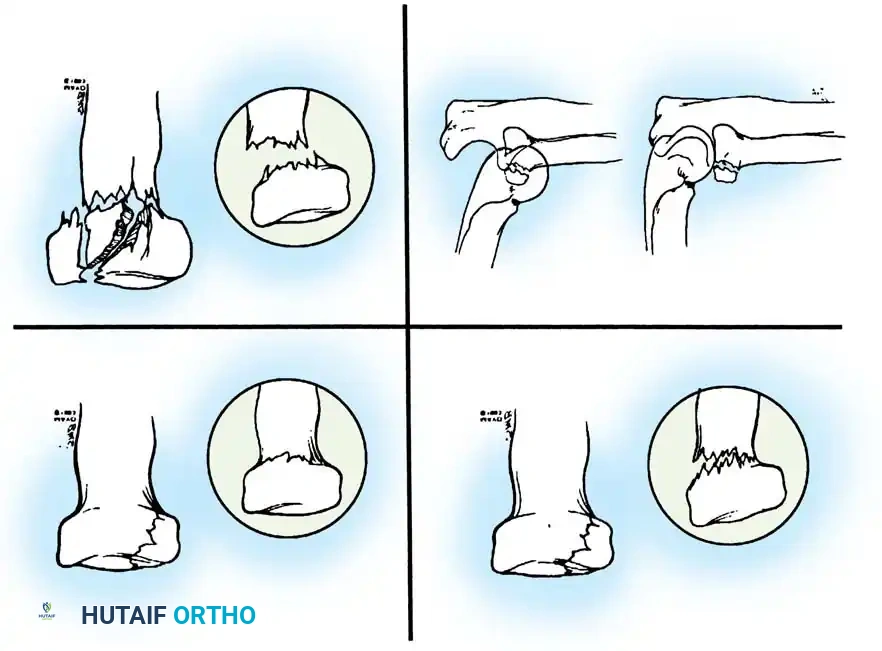
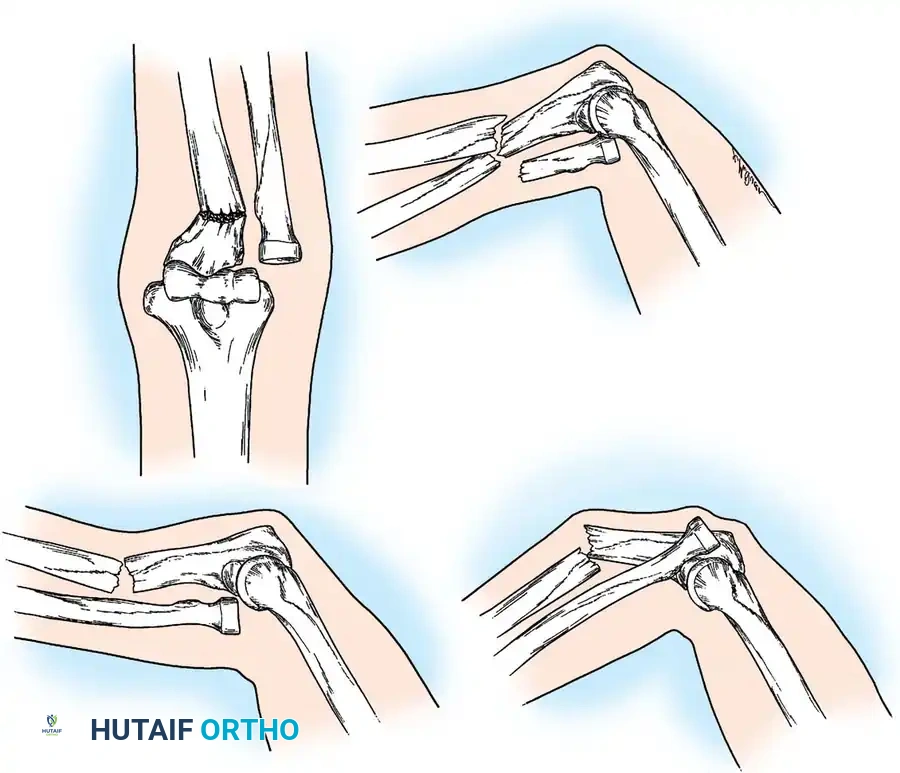
Schatzker classified olecranon fractures based on the fracture pattern and the mechanical considerations dictating the required type of internal fixation. Understanding this classification is paramount for preoperative planning.
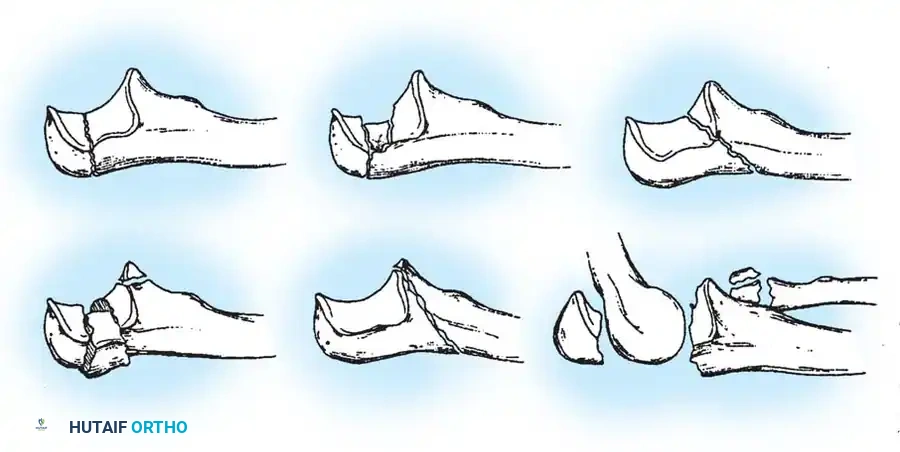
Fig. 54-52 A-F, Schatzker classification of olecranon fractures. (From Browner BD, Jupiter JB, Levine AM, et al, eds: Skeletal trauma, Philadelphia, Saunders, 1992.)
The Schatzker classification includes:
* Transverse: Typically avulsion injuries amenable to tension band wiring.
* Transverse-Impacted: Requires elevation of the impacted articular segment and bone grafting before fixation.
* Oblique: May require lag screw fixation in addition to a neutralization plate or tension band.
* Comminuted: High-energy injuries often requiring plate osteosynthesis to prevent shortening of the greater sigmoid notch.
* Oblique-Distal: Fractures extending distal to the coronoid process, compromising elbow stability.
* Fracture-Dislocation: Complex injuries requiring rigid plate fixation to restore the stabilizing buttress of the proximal ulna.
Surgical Decision Making: Fixation vs. Excision
The operative methods commonly employed include:
1. Open reduction and fixation with a figure-of-eight wire loop (Tension Band).
2. Medullary fixation (K-wires or screws).
3. A combination of intramedullary pins/screws and tension bands.
4. Contoured plate and screws.
5. Excision of the proximal fragment with triceps advancement.
Frequently, a combination of techniques is utilized. The choice depends heavily on the nature and location of the fracture, the degree of comminution, and the physiological age and functional demands of the patient.
Advocates of ORIF argue that this method:
1. Provides an anatomical reduction of the bony fragment, restoring a congruous articular surface.
2. Achieves rigid fixation, permitting early ROM.
3. Preserves the osseous architecture required for elbow stability.
4. Maintains the maximal extensor power of the triceps muscle.
Advocates of Fragment Excision (typically reserved for elderly, low-demand patients with severe comminution) argue that:
1. The risk of an incongruous articular surface is eliminated.
2. Hardware-related complications (e.g., painful subcutaneous prominence, device failure) are avoided.
3. Elbow stability and extensor power are not clinically impaired if less than 50% of the olecranon is excised and the triceps is securely advanced.
4. Immediate elbow motion can be instituted.
Clinical Pearl: A cadaveric biomechanical study by Moed et al. compared joint stresses in elbows treated with tension band wiring versus those with 50% excision of the proximal fragment. The joint stresses measured in the excision specimens were significantly higher, underscoring the biomechanical superiority of preserving the olecranon whenever feasible to prevent accelerated articular wear.
SURGICAL APPROACH AND POSITIONING
Patient Positioning
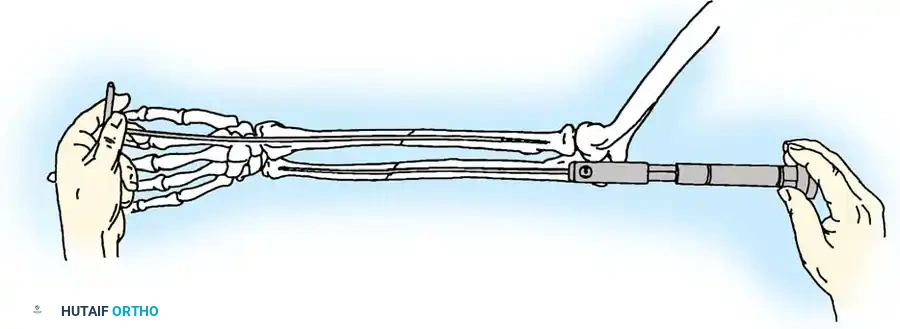
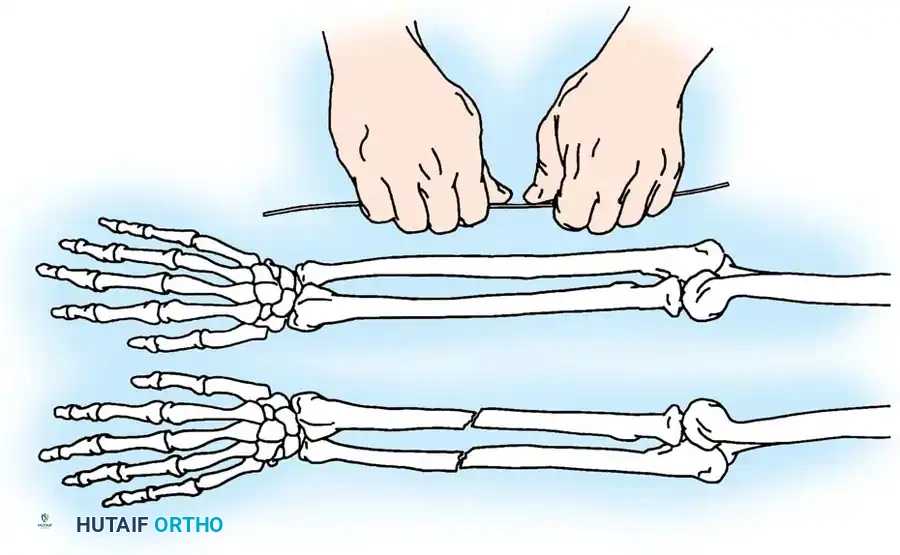
The patient may be positioned in the lateral decubitus position with the arm draped over a radiolucent post, or in the supine position with the arm brought across the chest. The lateral position often provides superior visualization and easier access for fluoroscopy. A sterile tourniquet is applied high on the arm.
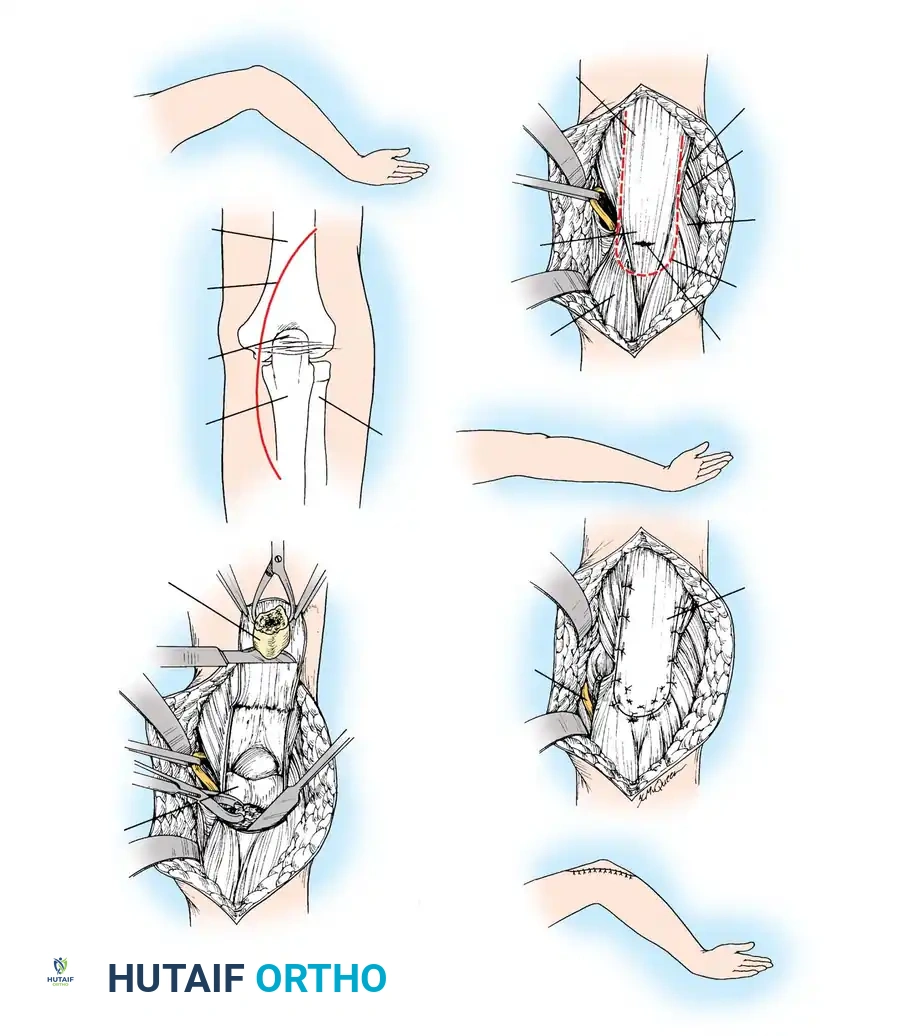
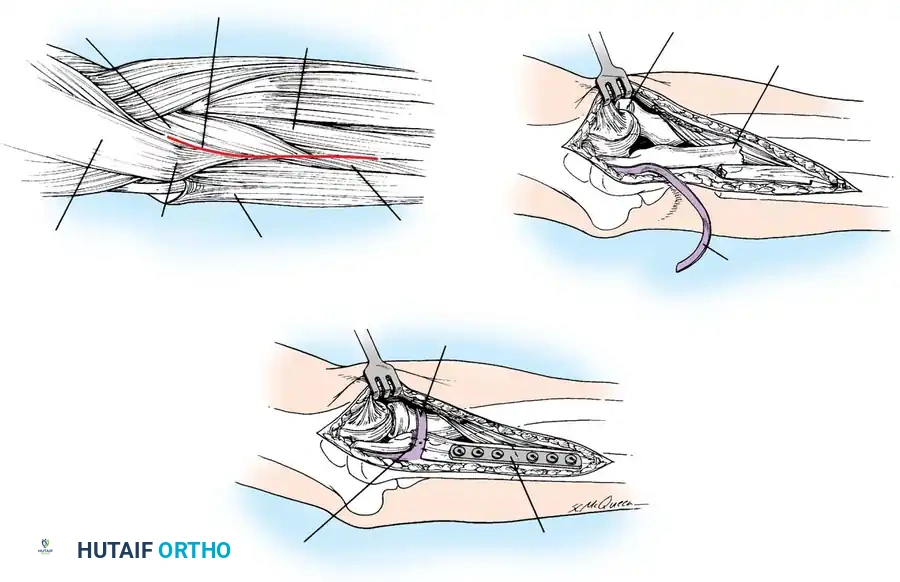
The Posterior Approach
- Make a longitudinal incision beginning 2.5 cm proximal to the tip of the olecranon.
- To avoid a painful scar directly over the bony prominence, curve the incision slightly lateral to the tip of the olecranon, then continue it distally along the subcutaneous border of the ulnar shaft for 7.5 cm.
- Incise the deep fascia in line with the skin incision.
- Identify and protect the ulnar nerve, particularly if the fracture extends medially or if plate fixation is planned. Routine transposition is not required unless the nerve is involved in the fracture site or hardware placement threatens it.
SURGICAL TECHNIQUES
1. Open Reduction and Fixation with Figure-of-Eight Wire Loop (Tension Band Principle)
The tension band principle is applicable to fractures of the olecranon that are non-comminuted and located well proximal to the coronoid process. It is most commonly used for transverse avulsion fractures.
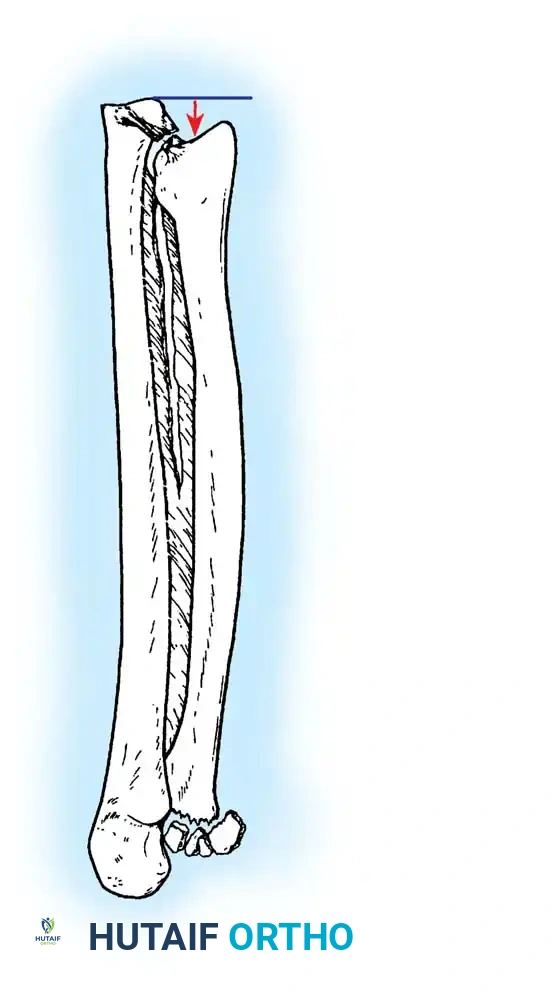
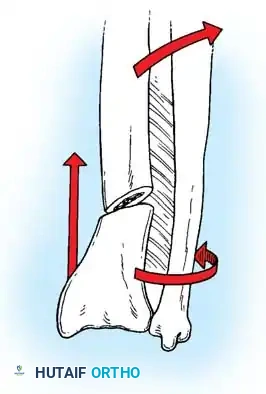
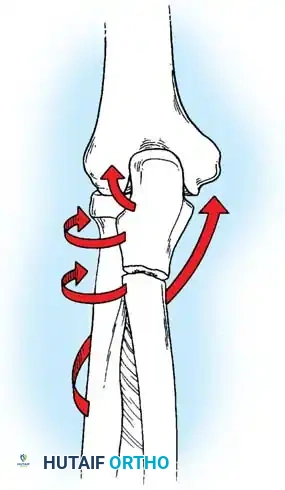
Biomechanics of the Tension Band:
The superficial (posterior) surface of the olecranon is the tension side of the bone. A figure-of-eight wire placed on this surface converts the tensile forces generated by the triceps into compressive forces across the articular fracture line, utilizing the humeral trochlea as a fulcrum.
Surgical Warning: A simple wire loop is biomechanically inferior to a figure-of-eight loop. If a simple loop is used—especially if its axis lies anterior to the mid-axis of the olecranon—the pull of the triceps will cause the fragments to separate posteriorly, leading to articular step-off and limited extension.
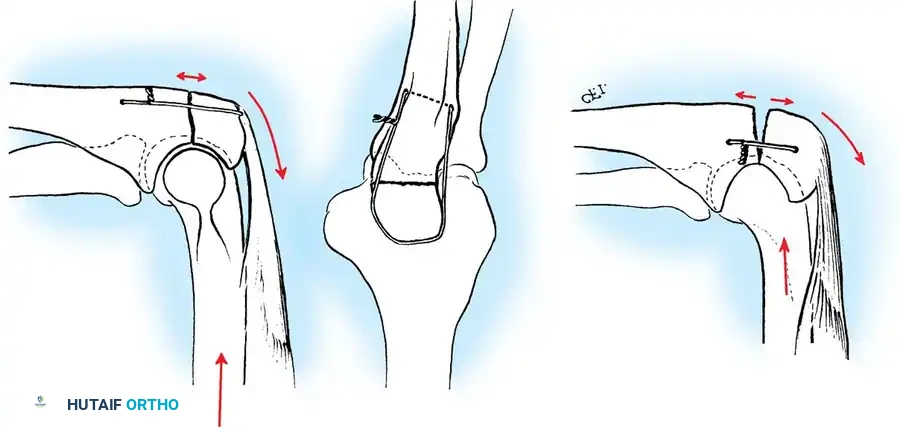
Fig. 54-53 A and B, Simple loop is not as satisfactory as figure-of-eight loop for fixing fracture of olecranon. C, Simple loop is insufficient when its long axis is in or anterior to long axis of olecranon.
🔪 Surgical Technique: Tension Band Wiring
- Exposure: Expose the fracture site and clear the joint of hematoma and small osteochondral debris.
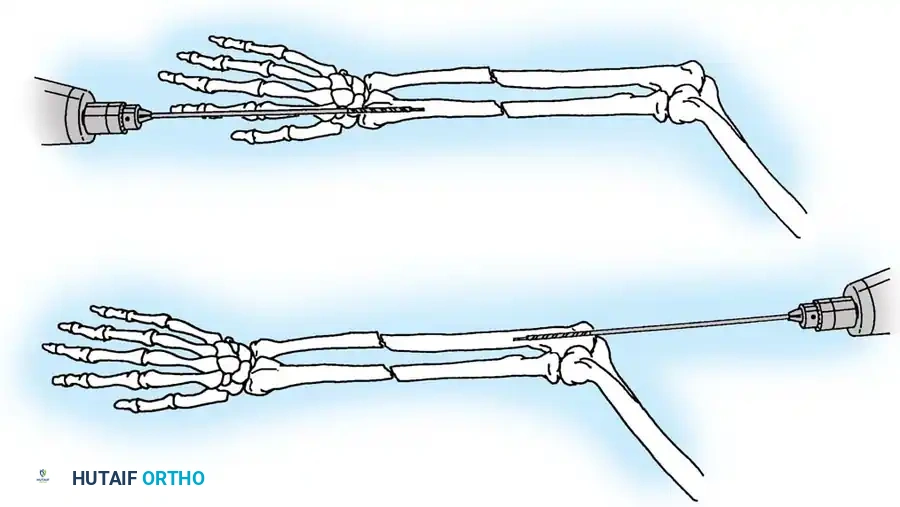
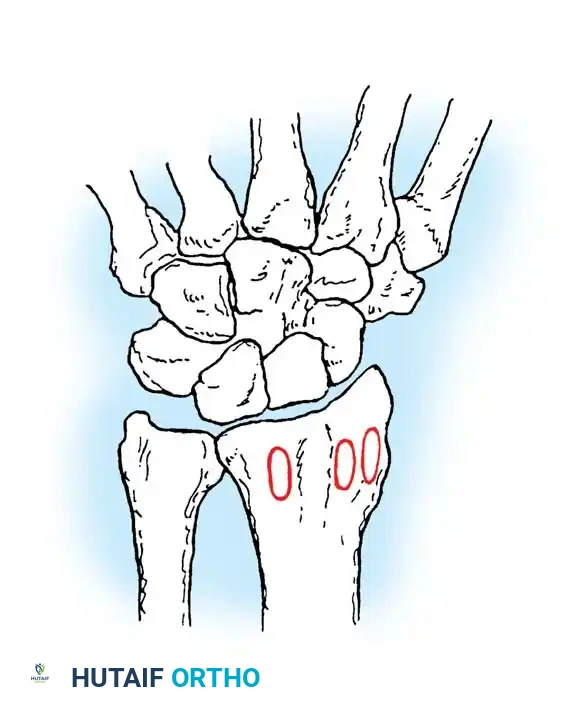
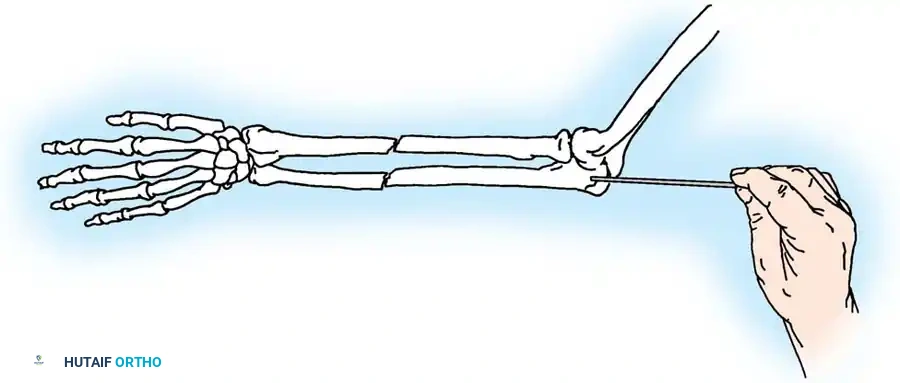
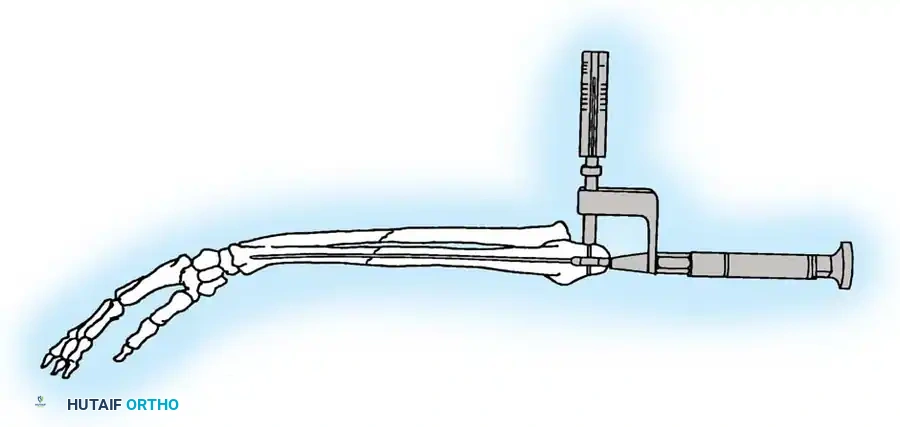
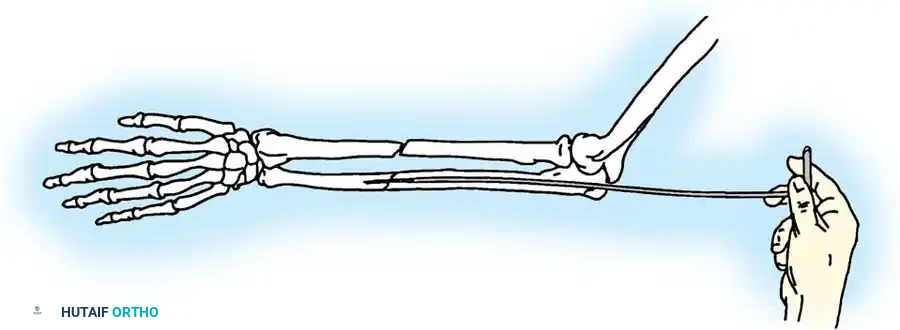
- Drill Hole: Drill a transverse hole from side to side in the distal ulnar fragment, approximately 2 to 3 cm distal to the fracture line. Ensure the hole is deep enough to avoid cutting through the posterior cortex.
- Wire Passage: Pass an 18-gauge (1.2 mm) stainless steel wire through the drill hole.
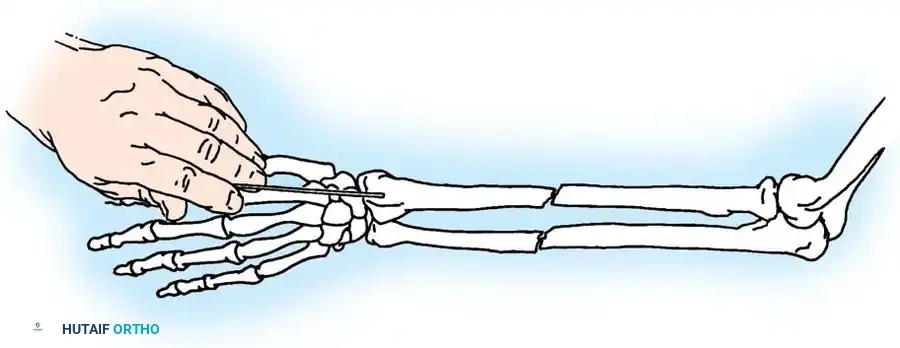
- Proximal Purchase: Pass the wire beneath the aponeurosis of the triceps muscle, directly adjacent to the bone, and around the tip of the olecranon. Alternatively, a transverse drill hole can be made in the proximal fragment if it is large enough.
- Figure-of-Eight: Carry one end of the wire obliquely across the posterior aspect of the fracture to the opposite side. Cross the other end over it to create a figure-of-eight configuration.
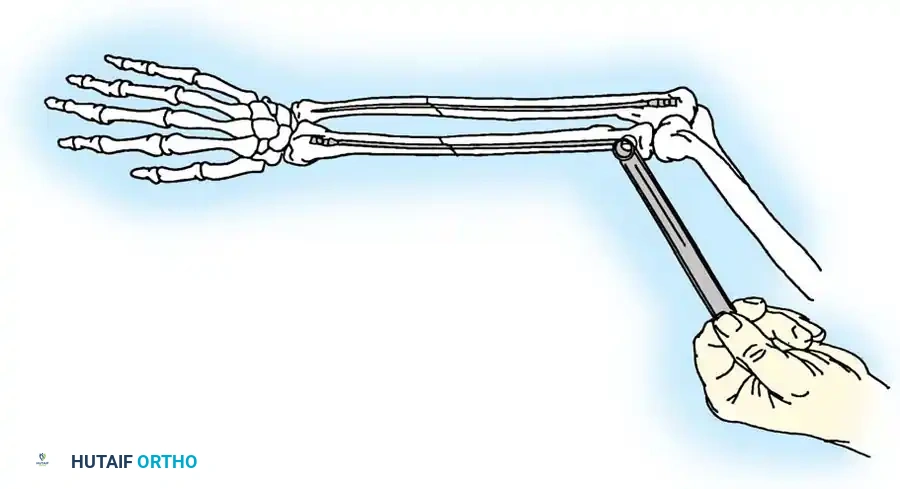
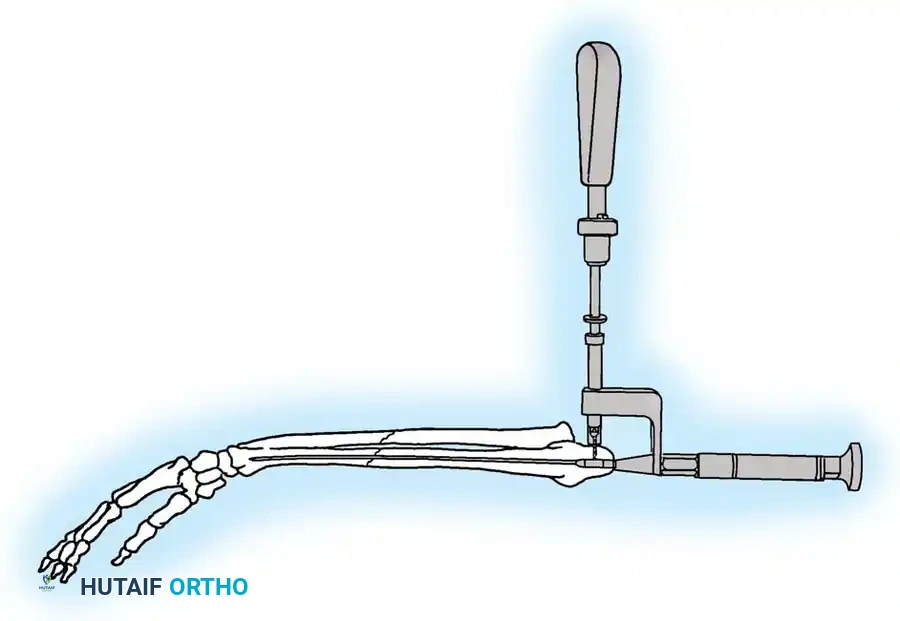
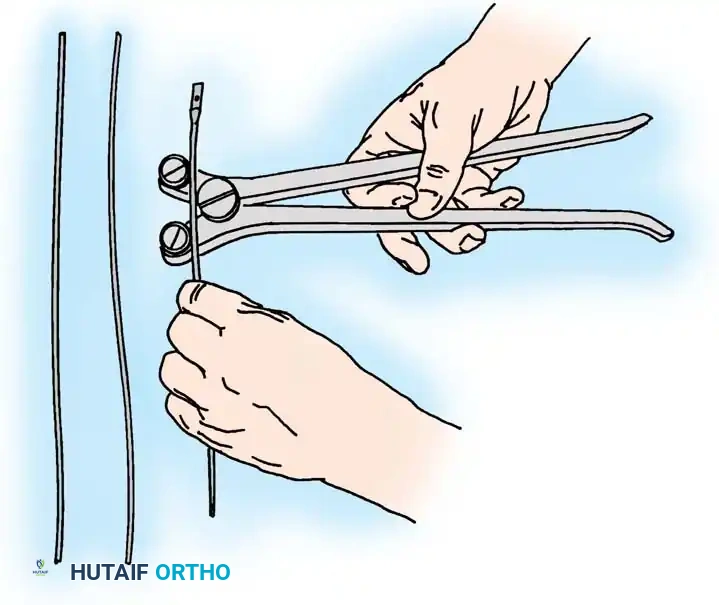
- Reduction and Compression: While an assistant grasps the proximal olecranon fragment with a large towel clip and exerts distal traction to anatomically reduce the fracture, twist the wire loop tightly.
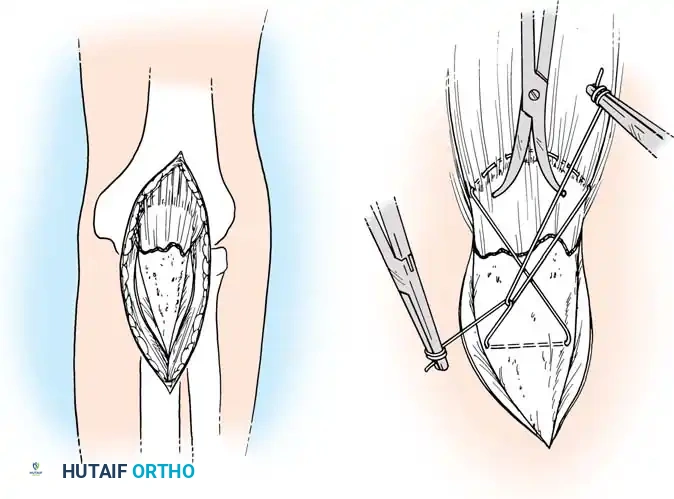
Fig. 54-54 Internal fixation of olecranon with tension band wire loop. Wire passed through hole drilled in distal fragment and through triceps aponeurosis adjacent to bone. Figure-of-eight loop adds stability to fracture and prevents distraction and posterior bowing.
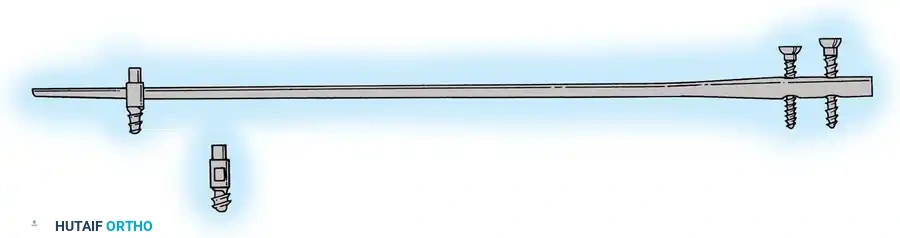
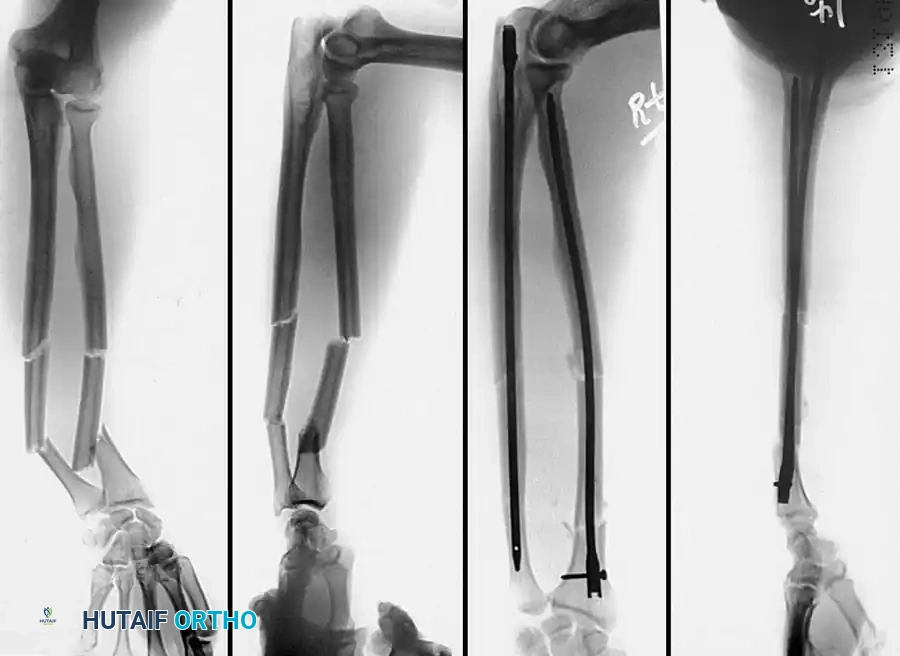
2. Intramedullary Fixation with Tension Band
If the fracture is more distal, or if there is a tendency for the proximal fragment to angulate posteriorly, a simple tension band wire is insufficiently stable. In these cases, intramedullary fixation (using Kirschner wires or a large cancellous screw) is combined with the tension band.
Kirschner Wires vs. Cancellous Screws:
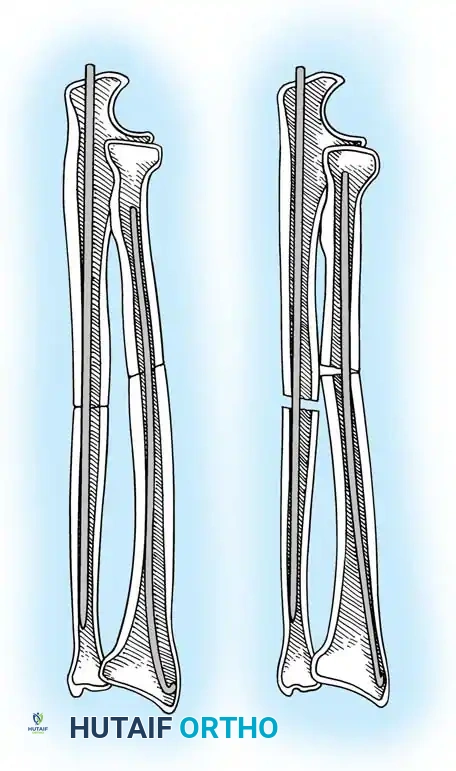
* K-wires: The AO technique utilizes two parallel K-wires (1.6 mm or 2.0 mm) driven down the medullary canal. To prevent proximal migration, the K-wires must engage the anterior cortex of the ulna distal to the coronoid.
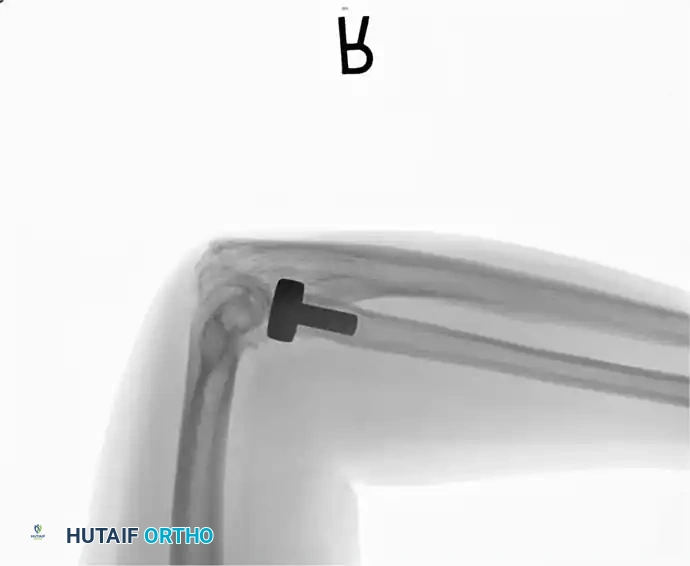
* Cancellous Screw: A biomechanical analysis by Murphy et al. demonstrated that a long 6.5-mm or 7.3-mm AO cancellous screw combined with a figure-of-eight wire provides a significantly stronger construct than K-wires. The screw must be long enough to achieve secure purchase in the ulnar diaphysis.

Fig. 54-55 Olecranon fracture repaired with long 6.5-mm AO cancellous screw and figure-of-eight tension band wire loop. Screw must engage cortex of diaphysis of ulna.
🔪 Surgical Technique: K-Wire and Tension Band (AO Technique)
- Reduction: Anatomically reduce the fragments and hold them temporarily with a reduction clamp.
- K-Wire Insertion: Introduce two parallel K-wires longitudinally from the tip of the olecranon across the fracture site. Direct them slightly anteriorly so they engage the anterior ulnar cortex distal to the coronoid process.
- Wire Loop: Pass an 18-gauge wire through a transverse drill hole in the distal fragment. Cross the wire in a figure-of-eight fashion over the posterior surface.
- Proximal Capture: Pass the wire around the protruding proximal ends of the K-wires.
- Double Twist: Weber and Vasey suggest twisting both limbs of the figure-of-eight loop. This double-twist modification ensures uniform compression across the fracture site.
- Securing K-wires: Bend the proximal ends of the K-wires 180 degrees, cut them short, and tap the bent ends deep into the triceps insertion and proximal bone to prevent symptomatic hardware prominence and migration.
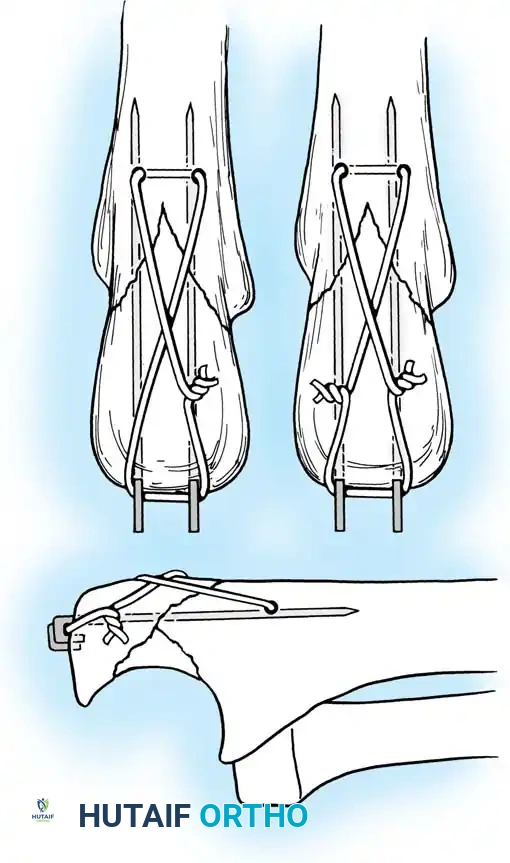
Fig. 54-56 A and B, Transverse olecranon fracture repaired with Kirschner wires and tension band technique. C, Double twist modification of wiring suggested by Weber and Vasey.
3. Excision of the Proximal Fragment
Excision is indicated primarily for elderly, low-demand patients with severe comminution where stable osteosynthesis is impossible, or when the articular surface cannot be congruously restored. Up to 50% of the olecranon can be excised without compromising elbow stability, provided the coronoid process and collateral ligaments remain intact.
🔪 Surgical Technique: Excision and Triceps Advancement
- Fragment Removal: Carefully dissect the comminuted fragments from the triceps tendon, preserving as much tendon length as possible.
- Joint Debridement: Inspect the joint and remove all intra-articular debris.
- Bone Preparation: Smooth the remaining proximal end of the ulna. If the midportion of the olecranon is comminuted but the proximal tip is intact, the central comminuted segment can be excised (Barford technique). The osteotomies must be directed accurately along the radius of the trochlear curve to reconstitute a smoothly curved notch.
- Triceps Advancement: Drill two or three longitudinal holes through the remaining proximal ulna. Pass heavy non-absorbable sutures (e.g., #2 or #5 FiberWire) through the triceps tendon using a Krackow stitch, pass them through the drill holes, and tie them securely over the posterior ulnar cortex with the elbow in 30 degrees of flexion.
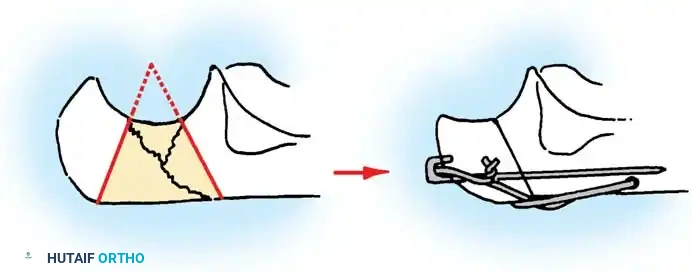
Fig. 54-57 Technique of excision of central one third of olecranon process (Barford, 1972). It is critical to err by making the radius of the notch too large, rather than too small.
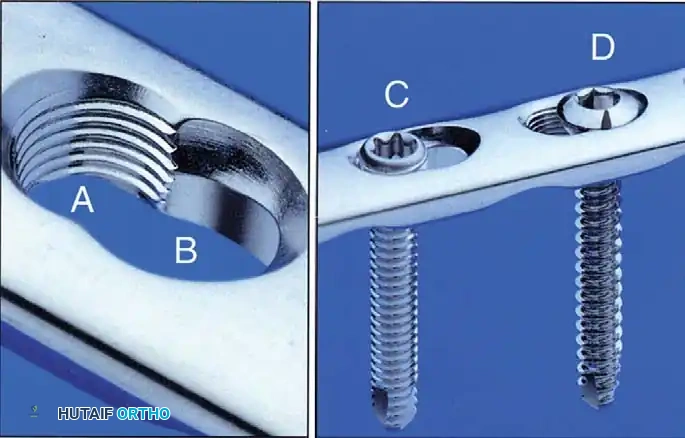
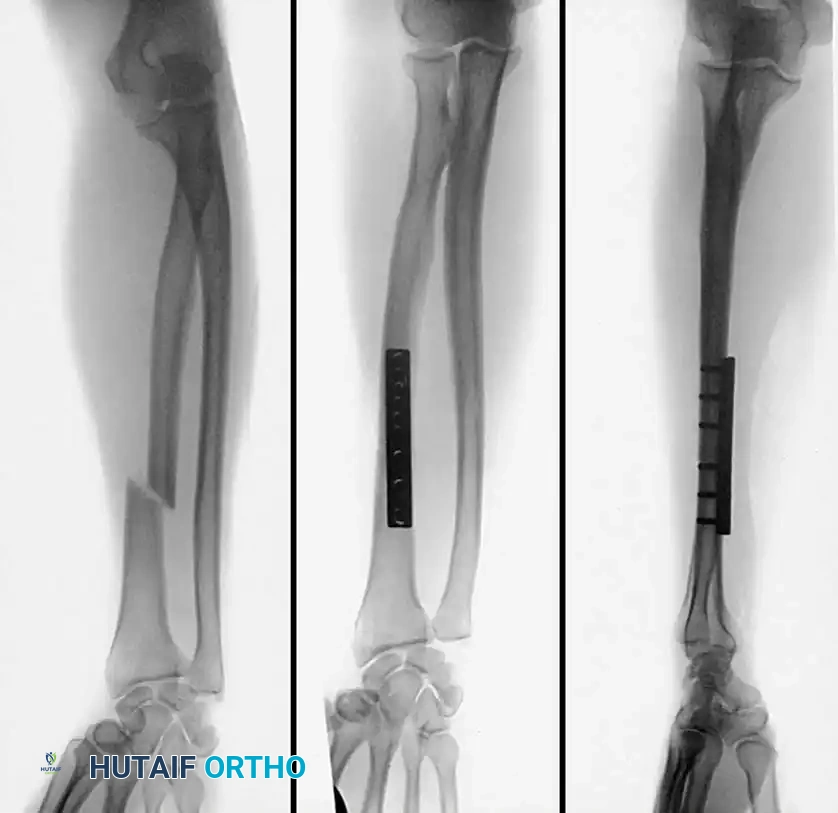
4. Plate Osteosynthesis
If comminution with bone loss prevents the use of a tension band compression technique—due to the risk of shortening the olecranon and narrowing the greater sigmoid notch—plate fixation is mandatory. Plating is also the gold standard for Monteggia fracture-dislocations, oblique fractures extending distally, and fractures involving the coronoid process.
Construct Design:
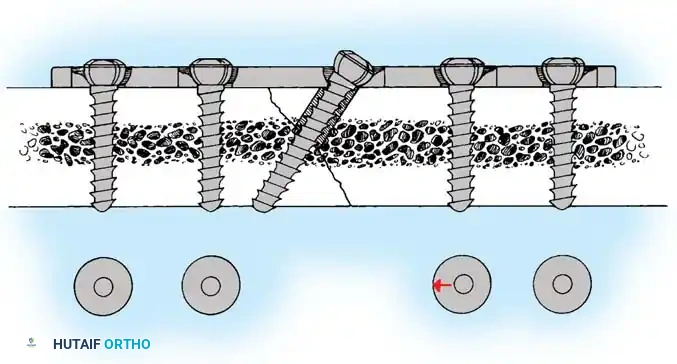
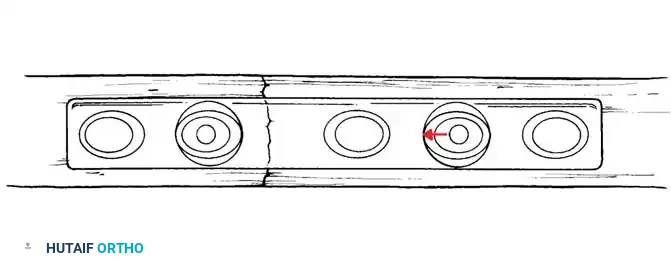
Hand-contoured reconstruction plates or modern, anatomically precontoured locking plates (e.g., Acumed, Synthes) provide rigid, stable fixation. The plate is applied to the posterior (tension) surface of the ulna.
Clinical Pearl: When applying a posterior plate, use unicortical screws for the holes immediately adjacent to the articular surface to avoid inadvertent penetration into the radioulnar or ulnohumeral joints.
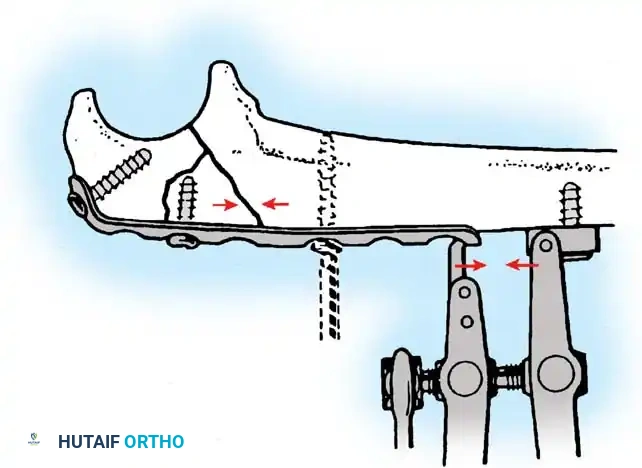

Fig. 54-58 A-C, Plate fixation can be used to stabilize comminuted fractures of the olecranon. Precontoured plates offer excellent proximal purchase with locking screws. (From Heim U, Pfeiffer KM: Internal fixation of small fractures, 3rd ed, Berlin, 1988, Springer-Verlag.)
🔪 Surgical Technique: Plate Fixation
- Reduction: Restore the articular block. Temporary K-wires can be used to hold comminuted articular fragments.
- Plate Application: Apply a precontoured olecranon plate to the posterior aspect of the proximal ulna. The proximal portion of the plate often wraps over the tip of the olecranon to capture the proximal fragment with multiple locking screws.
- Fixation: Secure the plate distally to the ulnar shaft using standard cortical or locking screws. If an oblique fracture line is present, a lag screw can be placed independently or through the plate to achieve interfragmentary compression.
- Bone Grafting: If significant metaphyseal void exists after elevating impacted articular fragments, autogenous cancellous bone graft or allograft should be packed into the defect prior to final plate tightening.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of olecranon fracture surgery relies
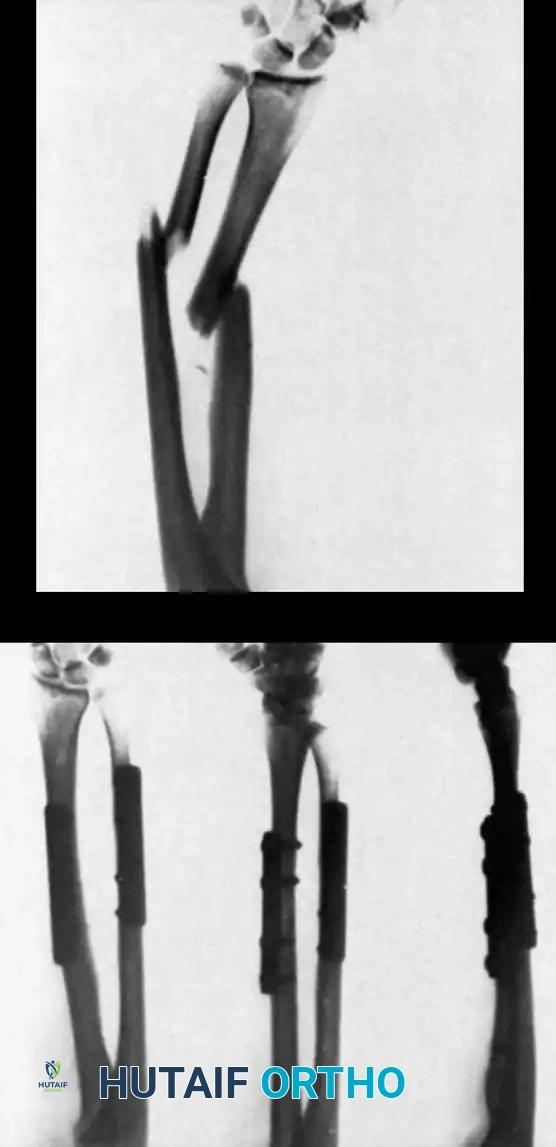
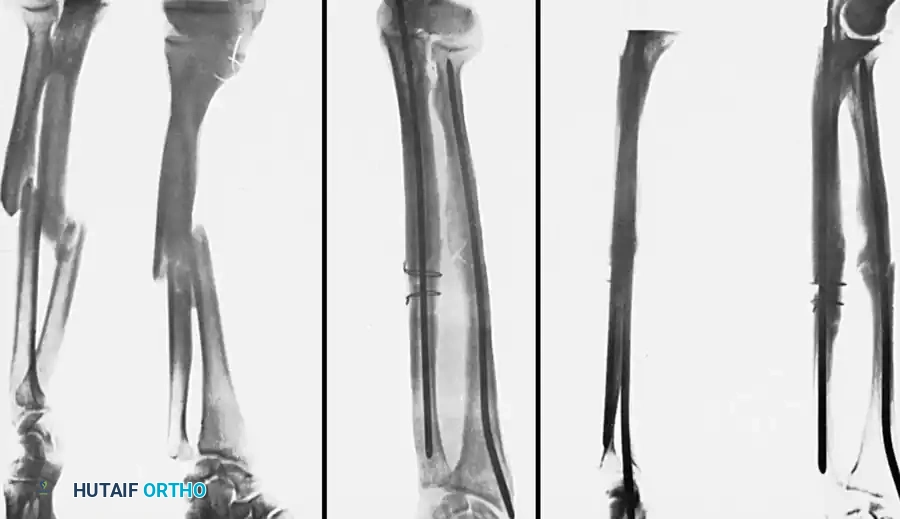
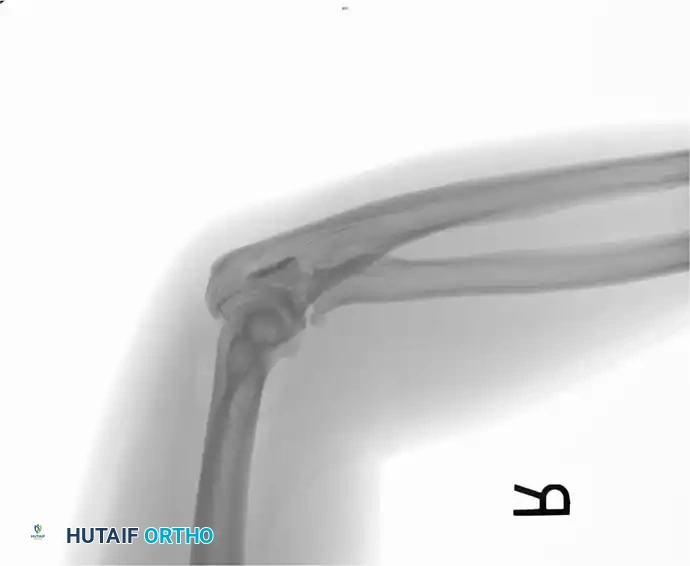
Associated Surgical & Radiographic Imaging










📚 Medical References
- Olecranon fractures in children: I. A clinical review; II. A new classifi cation and management algorithm, J Pediatr Orthop 19:559, 1999.
- Fowles JV, Kassab MT: Observations concerning radial neck fractures in children, J Pediatr Orthop 6:51, 1986.
- Fowles JV, Kassab MT, Moula T: Untreated posterior dislocation of the elbow in children, J Bone Joint Surg 66A:921, 1984.
- Furry KL: Comminuted fractures of the radial head, Clin Orthop Relat Res 353:40, 1998.
- Futami T, Tsukamoto Y, Fujita T: Rotation osteotomy for dislocation of the radial head: 6 cases followed for 7 (3-10) years, Acta Orthop Scand 63:455, 1992.
- Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children, J Pediatr Orthop 17:321, 1997.
- Gicquel P, De Billy B, Karger CS, et al: Olecranon fractures in 26 children with a mean follow-up of 59 months, J Pediatr Orthop 21:141, 2001.
- Gicquel P, Giacomelli M-C, Karger C, et al: Surgical technique and preliminary results of a new fi xation concept for olecranon fractures in children, J Pediatr Orthop 23:398, 2003.
- Gillingham BL, Rang M: Advances in children’s elbow fractures, J Pediatr Orthop 15:419, 1995 (editorial). Gillingham BL, Wright JG: Convergent dislocation of the elbow, Clin Orthop Relat Res 340:198, 1997.
- Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique), J Pediatr Orthop 17:325, 1997.
- Grantham SA, Kiernan HA: Displaced olecranon fractures in children, J Trauma 15:197, 1975.
- Graves SC, Canale ST: Fractures of the olecranon in children: long-term follow-up, J Pediatr Orthop 13:239, 1993.
- Gruber MA, Healy WA: The posterior approach to the elbow revisited, J Pediatr Orthop 16:215, 1996.
- Hallet J: Entrapment of the median nerve after dislocation of the elbow, J Bone Joint Surg 63B:408, 1981.
- Hansen PE, Barnes DA, Tullos HS: Arthroscopic diagnosis of an injury pattern in the distal humerus of an infant, J Pediatr Orthop 2:569, 1982.
- Hasler CC, Von Laer L, Hell AK: Open reduction, ulnar osteotomy and external fi xation for chronic anterior dislocation of the head of the radius, J Bone Joint Surg 87B:88, 2005.
- Hassmann GC, Brunn F, Neer CS: Recurrent dislocation of the elbow, J Bone Joint Surg 57A:1080, 1975.
- Herring JA, Sullivan JA: Instructional case: recurrent dislocation of the elbow, J Pediatr Orthop 9:483, 1989.
- Hirayama T, Takemitsu Y, Yagihara K, et al: Operation for chronic dislocation of the radial head in children: reduction by osteotomy of the ulna, J Bone Joint Surg 69B:639, 1987.
- Jakob R, Fowles JV, Rang M, et al: Observations concerning fractures of the lateral humeral condyle in children, J Bone Joint Surg 57B:430, 1975.
- Javed A, Gúichet JM: Case report: arthrography for reduction of a fracture of the radial neck in a child with a nonossifi ed radial epiphysis, J Bone Joint Surg 83B:542, 2001.
- Jeffery CC: Fracture of the head of the radius in children, J Bone Joint Surg 32B:314, 1950.
- Kapel O: Operation for habitual dislocation of the elbow, J Bone Joint Surg 33A:707, 1951.
- Kasser JR, Richards K, Millis M: The triceps-dividing approach to open reduction of complex
You Might Also Like