Management of Pelvic Ring and Sternoclavicular Joint Dislocations
Key Takeaway
Traumatic dislocations of the pubic symphysis, sacroiliac, and sternoclavicular joints represent severe, high-energy injuries requiring meticulous orthopedic management. While anterior sternoclavicular dislocations are often managed nonoperatively, posterior dislocations are true emergencies due to mediastinal compression risks. Pelvic ring disruptions demand precise restoration of the complex ligamentous anatomy to ensure biomechanical stability. This guide details evidence-based surgical indications, operative approaches, and complication management for these critical joint injuries.
Comprehensive Introduction and Patho-Epidemiology
Dislocations involving the symphysis pubis, sacroiliac (SI) joints, and the sternoclavicular (SC) joints represent a spectrum of severe osseoligamentous disruptions that occur almost exclusively in the setting of high-energy trauma. The adult pelvis is a highly stable, continuous ring; therefore, considerable kinetic energy is required to overcome the complex ligamentous structures that provide its inherent stability. Mechanisms of injury typically involve motor vehicle collisions, pedestrian-versus-auto accidents, industrial crush injuries, or falls from significant heights. Epidemiologically, these injuries exhibit a bimodal distribution, with high-energy mechanisms predominantly affecting young adult males, while low-energy falls may produce similar, albeit less displaced, fragility patterns in the osteoporotic elderly population.
The mortality associated with high-energy pelvic ring disruptions remains distressingly high, historically reported between 10% and 50% in patients presenting with hemodynamic instability. The immediate threat to life is primarily exsanguinating hemorrhage originating from the presacral venous plexus, disrupted cancellous bone surfaces, and, less commonly, the arterial branches of the internal iliac system (such as the superior gluteal or internal pudendal arteries). Consequently, the acute management of these injuries demands a multidisciplinary approach, integrating Advanced Trauma Life Support (ATLS) protocols, emergent mechanical stabilization (via pelvic binders or external fixation), and rapid hemostatic interventions such as preperitoneal pelvic packing or angiographic embolization.
High-energy axial loading that causes pelvic ring disruptions frequently results in concomitant injuries to the appendicular skeleton, most notably traumatic hip dislocations. Posterior dislocations of the hip are orthopedic emergencies requiring immediate closed reduction to mitigate the risk of devastating complications, specifically osteonecrosis of the femoral head. Furthermore, the transmission of massive traumatic forces through the axial skeleton can simultaneously disrupt other critical articulations, such as the sternoclavicular joint. Although sternoclavicular dislocations are relatively rare—accounting for less than 3% of all shoulder girdle injuries—a posterior (retrosternal) dislocation constitutes a true orthopedic and cardiothoracic emergency due to the perilous proximity of the displaced medial clavicle to the vital structures of the superior mediastinum.
Detailed Surgical Anatomy and Biomechanics
The structural integrity of the pelvic ring relies on an intricate balance between a robust posterior tension band and an anterior compressive strut. The sacroiliac joints constitute the posterior complex and are the primary weight-bearing articulations of the axial skeleton. They are stabilized by the interosseous sacroiliac ligaments, which are widely considered the strongest ligaments in the human body. These are supplemented by the anterior and posterior sacroiliac ligaments, as well as the accessory pelvic ligaments—namely, the sacrotuberous and sacrospinous ligaments. Disruption of this posterior complex, as seen in vertical shear (VS) or severe anteroposterior compression (APC-III) injuries, leads to profound vertical and rotational instability, completely uncoupling the spine from the lower extremities.
The anterior complex, centered around the pubic symphysis, acts as a critical secondary stabilizer, primarily resisting external rotation and tensile forces. The symphysis is an amphiarthrodial joint with an interposed fibrocartilaginous disc, supported by the superior and arcuate (inferior) pubic ligaments. Further dynamic and static stability is conferred by the interlacing fibers of the rectus abdominis and external oblique aponeuroses, which form a continuous fascial sleeve over the anterior ring. Biomechanically, while the anterior structures contribute only about 30% to the overall stability of the pelvic ring, their restoration is paramount for restoring the anatomical dimensions of the true pelvis and preventing pathological motion at the posterior SI joints during the gait cycle.
In the upper extremity, the sternoclavicular (SC) joint serves as the sole true synovial articulation connecting the appendicular skeleton to the axial skeleton. It is a diarthrodial, saddle-shaped joint containing an intra-articular fibrocartilaginous disc that enhances joint congruency and absorbs shock. Because the articular surfaces possess minimal intrinsic osseous stability, the joint relies almost entirely on its robust ligamentous envelope. The primary restraint to superior displacement is the costoclavicular (rhomboid) ligament, while the interclavicular ligament and the anterior/posterior sternoclavicular capsular ligaments resist anteroposterior translation. The posterior capsule is significantly thicker and stronger than the anterior capsule, which explains why anterior dislocations are vastly more common than posterior ones. However, when the posterior capsule fails, the medial clavicle is driven into the superior mediastinum, directly threatening the trachea, esophagus, innominate artery, internal jugular vein, subclavian vessels, and the brachial plexus.
Concomitant injuries, such as traumatic posterior hip dislocations, introduce another layer of anatomical complexity. The vascular supply to the femoral head is predominantly derived from the medial femoral circumflex artery (MFCA), which traverses the posterior aspect of the femoral neck. During a posterior hip dislocation, the MFCA is subjected to extreme tension, torsion, or direct mechanical compression. This exquisite vascular vulnerability dictates the urgency of reduction; a delay beyond 6 hours exponentially increases the risk of irreversible ischemia and subsequent osteonecrosis (avascular necrosis) of the femoral head, profoundly altering the patient's long-term functional prognosis.
Exhaustive Indications and Contraindications
The primary goal in managing pelvic ring and sternoclavicular disruptions is the restoration of mechanical stability and anatomical alignment to protect neurovascular structures, facilitate early mobilization, and minimize long-term disability. The decision to proceed with operative intervention hinges on a meticulous assessment of the patient's hemodynamic status, the degree of osseoligamentous instability, and the presence of associated visceral or neurovascular injuries. Nonoperative management is strictly reserved for mechanically stable injury patterns (e.g., APC-I, LC-I without significant displacement) or anterior sternoclavicular dislocations in patients who are asymptomatic or have low functional demands.
Operative indications for the pelvic ring are generally defined by the failure of the anterior and/or posterior tension bands. Symphyseal diastasis greater than 2.5 cm is a definitive indication for internal fixation, as it represents complete failure of the anterior tension band and the pelvic floor musculature, typically associated with profound rotational instability (APC-II or APC-III). Similarly, any sacroiliac joint dislocation or fracture-dislocation with significant displacement (greater than 1 cm), vertical shear injuries, or highly unstable crescent fractures demand operative stabilization. In the acute trauma setting, hemodynamic instability unresponsive to initial volume resuscitation is an absolute indication for emergent provisional stabilization, utilizing a pelvic binder, external fixation, or preperitoneal packing prior to definitive internal fixation.
For the sternoclavicular joint, surgical indications are highly specific. Anterior dislocations are almost universally managed nonoperatively, as the functional deficit is minimal despite the cosmetic deformity. Surgical intervention for anterior dislocations is rarely indicated and is generally reserved for highly symptomatic, chronic, unreduced, or recurrent dislocations in elite, high-demand athletes. Conversely, posterior sternoclavicular dislocations represent a true orthopedic emergency. Surgical management is strictly indicated for irreducible posterior dislocations or when there is clinical evidence of mediastinal compression (stridor, dyspnea, venous congestion, or diminished distal pulses).
| Pathology / Injury Type | Operative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Pubic Symphysis Diastasis | Diastasis > 2.5 cm; APC-II/III patterns; Open pelvic fractures; Concomitant urologic injury requiring repair. | Hemodynamic instability precluding definitive fixation (use ex-fix instead); Active pelvic infection. | Severe contamination (e.g., bowel spillage); Extreme medical comorbidities. |
| Sacroiliac Joint Dislocation | Displacement > 1 cm; Vertical shear (VS) injuries; Unstable crescent fractures; Spinopelvic dissociation. | Inadequate soft tissue envelope (Morel-Lavallée lesion) over the surgical approach site. | Pre-existing asymptomatic SI joint ankylosis; Non-ambulatory baseline status. |
| Posterior SC Joint Dislocation | Irreducible closed reduction; Signs of mediastinal compression (vascular, airway, esophageal). | Lack of cardiothoracic surgical backup (absolute for posterior approach). | Asymptomatic chronic posterior dislocation discovered incidentally. |
| Anterior SC Joint Dislocation | Highly symptomatic chronic instability in high-demand athletes; Skin tenting threatening necrosis. | Acute asymptomatic presentation; Sedentary patient. | General anesthesia risks outweighing cosmetic benefits. |
| Traumatic Hip Dislocation | Irreducible closed reduction; Incarcerated intra-articular fragments; Associated unstable acetabular fracture. | Medically unstable patient (damage control orthopedics applies). | Delayed presentation (>3 weeks) where primary arthroplasty may be preferred. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful outcomes in complex pelvic and sternoclavicular reconstructions. For pelvic ring injuries, the initial evaluation must include a standard anteroposterior (AP) radiograph of the pelvis, supplemented by inlet and outlet views to fully appreciate rotational and vertical displacement, respectively. However, a fine-cut computed tomography (CT) scan with 2D multiplanar and 3D volumetric reconstructions is the gold standard. The CT scan is indispensable for identifying occult posterior ring injuries, sacral dysmorphism (critical for safe percutaneous iliosacral screw placement), and the exact trajectory of fracture lines through the acetabulum or SI joints.
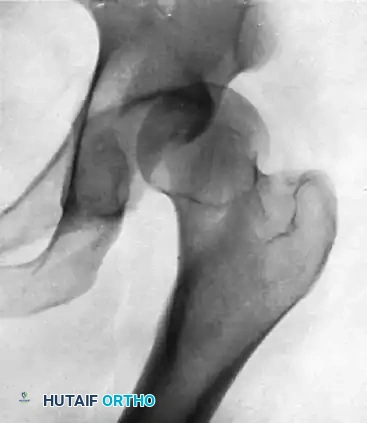
FIGURE A: Initial anteroposterior radiograph demonstrating a posterior dislocation of the hip, a frequent concomitant injury in high-energy pelvic trauma. Note the superior and lateral displacement of the femoral head relative to the acetabulum.
When planning for pubic symphysis plating, the surgeon must template the size and contour of the plate utilizing the 3D CT reconstructions. A multi-hole (usually 4 to 6 holes) 3.5mm or 4.5mm reconstruction plate or a specialized pre-contoured symphyseal plate is selected. Patient positioning is critical: the patient is placed supine on a fully radiolucent Jackson table or a flat trauma table. The entire abdomen, from the costal margin down to the mid-thighs bilaterally, is prepped and draped to allow for extensile approaches if necessary.
SURGICAL PEARL: Always ensure a Foley catheter is placed prior to the procedure to decompress the bladder and assist in identifying the urethra, which is highly susceptible to injury in anterior pelvic ring disruptions. In cases of suspected urethral transection (e.g., blood at the meatus, high-riding prostate), a retrograde urethrogram must be performed, and a suprapubic catheter may be required in coordination with urology.
For sternoclavicular joint dislocations, preoperative imaging must include a contrast-enhanced CT scan of the chest. Plain radiographs (such as the serendipity view) are historically significant but often difficult to interpret due to overlapping thoracic anatomy. The CT angiogram is paramount for assessing the exact relationship of the medially displaced clavicle to the great vessels and the trachea. When operating on a posterior SC joint dislocation, the patient is placed in a beach-chair or supine position with a substantial bump between the scapulae to allow the shoulders to fall posteriorly, aiding in the reduction of the clavicle. Crucially, a cardiothoracic surgeon must be available on standby, and the chest must be prepped for an emergent median sternotomy in the event of catastrophic hemorrhage upon reduction of the clavicle from the mediastinum.
Step-by-Step Surgical Approach and Fixation Technique
The operative approach to the anterior pelvic ring for pubic symphysis diastasis utilizes the classic Pfannenstiel incision. The incision is made transversely, approximately two fingerbreadths superior to the pubic symphysis, extending 10 to 15 centimeters. The subcutaneous tissues are sharply dissected down to the anterior rectus sheath. The sheath is incised transversely, and the rectus abdominis muscles are identified and split vertically along the linea alba. Extreme care must be taken at the inferior aspect of the dissection to identify and protect the spermatic cord in males or the round ligament in females, which exit the superficial inguinal ring laterally.
Once the rectus muscles are retracted laterally, the retropubic space of Retzius is developed via blunt dissection. The surgeon sweeps the bladder posteriorly, utilizing a malleable retractor to protect it throughout the procedure. The superior pubic rami and the disrupted symphyseal fibrocartilage are exposed. The symphysis must be meticulously debrided of interposed soft tissue and hematoma to facilitate an anatomical reduction. Reduction is typically achieved by placing pointed Weber reduction clamps on the superior pubic rami. Alternatively, a Jungbluth clamp can be utilized; this involves pre-drilling 3.5mm holes into the rami on either side of the symphysis, placing the clamp tines into the holes, and slowly compressing the joint to restore the physiological width (normally 2-5 mm). Once reduced, a 4-to-6 hole 3.5mm or 4.5mm reconstruction plate is contoured to the superior aspect of the pubic ring and secured with fully threaded cortical screws, ensuring bicortical purchase without penetrating the retro-pubic structures.
For the surgical management of the sternoclavicular joint, particularly irreducible posterior dislocations, modern techniques rely exclusively on robust soft-tissue reconstruction rather than rigid metallic fixation. A transverse incision is made centered over the medial clavicle, extending medially over the manubrium. The platysma is incised in line with the incision, and the periosteum of the medial clavicle and manubrium is exposed. The anterior capsule, though usually torn, is preserved for later repair. A towel clip is placed around the medial clavicle to apply anterior and lateral traction. A blunt periosteal elevator can be carefully inserted behind the clavicle to lever it anteriorly, taking extreme caution not to plunge into the mediastinum.
SURGICAL WARNING: THE DANGER OF HARDWARE MIGRATION
Historically, smooth K-wires or Steinmann pins were used to stabilize the SC joint. This practice is now universally condemned. Occasionally, a whole pin migrates, or the pin breaks, and parts of it may migrate directly into the heart, pulmonary artery, innominate artery, or aorta. Reports suggest that the incidence of significant, life-threatening complications approaches 25% when pins are used in sternoclavicular procedures. Never use unthreaded pins or wires across the sternoclavicular joint.
Once the SC joint is reduced, a figure-of-eight reconstruction is performed. Drill holes are carefully created in the medial clavicle and the manubrium. A specialized drill guide and a malleable retractor must be placed posterior to the bone to protect the underlying mediastinal structures. Heavy, non-absorbable tape (e.g., FiberWire) or a robust tendon autograft/allograft (such as a semitendinosus or gracilis graft) is passed through the drill holes in a figure-of-eight fashion. The graft or suture is tensioned and tied while an assistant holds the joint in perfect anatomic reduction. Finally, the remaining anterior capsule and the sternal head of the sternocleidomastoid muscle are meticulously imbricated and repaired over the construct to provide additional dynamic stability.
Complications, Incidence Rates, and Salvage Management
The management of pelvic ring and sternoclavicular joint dislocations is fraught with potential complications, ranging from mechanical failures to life-threatening vascular events. In pelvic ring injuries, the most common postoperative complication is hardware failure or loss of reduction, particularly in osteoporotic bone or in patients who are non-compliant with weight-bearing restrictions. Symphyseal plate breakage or screw pullout occurs in up to 15% of cases, though many of these are radiographically evident but clinically asymptomatic, requiring no further intervention. Infection is a devastating complication, particularly following open pelvic fractures or extensive Morel-Lavallée lesions, necessitating aggressive serial debridements, hardware removal if stability is compromised, and prolonged targeted intravenous antibiotic therapy.
Urologic and neurological complications are intimately associated with the initial trauma but can be exacerbated iatrogenically. Injury to the L5 or S1 nerve roots can occur during percutaneous iliosacral screw placement if the trajectory violates the sacral neural foramina. Intraoperative neuromonitoring (EMG/SSEP) and meticulous fluoroscopic or navigation-assisted techniques are mandatory to mitigate this risk. Furthermore, sexual dysfunction and chronic pelvic pain are reported in up to 40% of patients with severe pelvic ring disruptions, stemming from injury to the parasympathetic plexus (nervi erigentes) or post-traumatic SI joint arthrosis, which may eventually require SI joint arthrodesis as a salvage procedure.
In the context of associated hip dislocations, osteonecrosis of the femoral head is the most feared complication. Even with prompt and concentric closed reduction within the golden 6-hour window, patients remain at a 5% to 15% risk for late-onset osteonecrosis and post-traumatic osteoarthritis. This is due to the initial mechanical insult to the articular chondrocytes and the transient ischemia experienced before reduction. Delaying reduction beyond 6 hours increases this risk to over 50%.

FIGURE B: Radiograph taken 8 months after successful closed reduction of a posterior hip dislocation. The image reveals advanced osteonecrosis of the femoral head. Note the profound subchondral sclerosis, narrowed joint space, and early structural collapse of the femoral head, necessitating total hip arthroplasty as a salvage procedure.
For sternoclavicular joint reconstructions, complications include recurrent instability, graft failure, and neurovascular injury. Recurrent anterior instability occurs in approximately 10% of reconstructed SC joints, often due to premature return to heavy lifting or contact sports. Salvage management for failed SC joint reconstructions or severe post-traumatic arthrosis involves a medial clavicle excision (resection arthroplasty). However, the excision must be limited to the medial 1.5 cm to preserve the attachment of the costoclavicular ligament; violating this ligament will result in profound, intractable instability of the entire shoulder girdle.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Symphyseal Plate Failure | 10% - 15% | Patient non-compliance; Osteoporosis; Undiagnosed posterior ring instability. | Often observation if asymptomatic. Revision plating with dual plates or posterior stabilization if painful. |
| Iatrogenic Nerve Root Injury | 2% - 5% | Malpositioned iliosacral screws violating L5/S1 foramina. | Immediate screw removal/revision; Corticosteroid therapy; Gabapentinoids for neuropathic pain. |
| Femoral Head Osteonecrosis | 5% - 50% (Time-dependent) | Disruption of MFCA during posterior hip dislocation; >6 hr delay to reduction. | Core decompression (early stage); Total Hip Arthroplasty (late stage with structural collapse). |
| SC Joint Hardware Migration | Up to 25% (Historical) | Use of smooth K-wires or Steinmann pins across the SC joint. | Emergent cardiothoracic intervention for retrieval; Absolute avoidance of pins as primary prevention. |
| Recurrent SC Joint Instability | 5% - 10% | Graft stretching; Premature return to sport; Inadequate initial fixation. | Revision allograft reconstruction; Medial clavicle resection arthroplasty (preserving costoclavicular ligament). |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following surgical stabilization of the pelvic ring and sternoclavicular joint must be meticulously phased to protect the surgical reconstruction while preventing the deleterious effects of prolonged immobilization, such as deep vein thrombosis, pulmonary compromise, and severe joint contractures. For pelvic ring disruptions, the protocol is heavily dictated by the integrity of the posterior ring fixation. If the posterior ring is solidly fixed (e.g., via transiliac-transsacral screws or robust iliosacral screws), patients may be allowed touch-down weight-bearing (TDWB) or toe-touch weight-bearing on the affected side immediately postoperatively.
During the first 6 weeks, the primary focus is on strict adherence to weight-bearing restrictions, deep vein thrombosis (DVT) prophylaxis (typically low-molecular-weight heparin for 28 to 35 days), and early mobilization out of bed to a chair. Active and passive range of motion of the hips, knees, and ankles is encouraged to prevent stiffness. From weeks 6 to 12, clinical and radiographic assessments dictate the progression of weight-bearing. Once bridging callus is visualized or fracture lines begin to obscure on radiographs, patients are systematically advanced to partial, and eventually full, weight-bearing. Core strengthening and pelvic stabilization exercises are introduced. Return to heavy manual labor or high-impact sports is generally restricted until 6 to 9 months postoperatively, contingent upon full radiographic union and the restoration of symmetric lower extremity strength.
Following sternoclavicular joint reconstruction, the upper extremity must be rigorously protected to allow the soft-tissue graft or capsular repair to integrate and heal. The patient is immediately placed in a specialized figure-of-eight harness or a well-fitted shoulder sling for 4 to 6 weeks. During Weeks 0 to 4, absolute immobilization of the SC joint is required. Gentle pendulum exercises at the glenohumeral joint may be permitted depending on the security of the fixation, but active forward elevation, abduction, and cross-body adduction are strictly prohibited to prevent immense sheer forces across the medial clavicle.
Entering Weeks 4 to 8, the sling is gradually weaned. The patient begins active-assisted range of motion under the strict guidance of a physical therapist, limiting forward elevation to 90 degrees and avoiding terminal extension. From Weeks 8 to 12, the protocol progresses to full active range of motion, and the initiation of periscapular, deltoid, and rotator cuff strengthening begins. Isometric exercises transition to light isotonic resistance. Months 4 to 6 focus on work-hardening and sport-specific drills. Return to heavy lifting, overhead occupational tasks, or contact sports is generally restricted until at least 6 months postoperatively, and only after clinical stability is unequivocally confirmed and the patient demonstrates symmetrical shoulder girdle strength without apprehension.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative management for pelvic ring and sternoclavicular joint injuries is deeply rooted in landmark orthopedic literature. The biomechanical understanding of pelvic ring stability was revolutionized by the foundational work of Pennal, Tile, and later Young and Burgess, whose classification system remains the universally accepted language for describing the vector of force and resulting instability patterns. Their work established the critical distinction between rotationally unstable (but vertically stable) injuries and those with complete global instability, directly informing the surgical indications we adhere to today.
Regarding surgical technique and outcomes, the seminal papers by Matta and Tornetta established the standard for anatomical reduction of the pelvic ring. Matta's criteria demonstrated a direct correlation between the quality of the anterior and posterior reduction (with residual displacement <1 cm considered excellent) and long-term functional outcomes, significantly reducing the incidence of post-traumatic pelvic pain and gait abnormalities. Furthermore, the pioneering work of Routt et al. popularized the use of fluoroscopically guided percutaneous iliosacral screws, drastically reducing the morbidity, blood loss, and infection rates historically associated with extensile open posterior approaches.
In the realm of sternoclavicular joint management, the literature is unequivocally defined by a paradigm shift away from metallic fixation. Early reports in the mid-20th century highlighted the catastrophic, often fatal, complications of K-wire migration into the mediastinum. The definitive guidelines now universally condemn this practice. The modern gold standard was established by Waters et al., who biomechanically validated and clinically advocated for the figure-of-eight suture and tendon graft stabilization techniques. Their longitudinal studies demonstrated that soft-tissue reconstruction of the costoclavicular and sternoclavicular ligaments provides superior multidirectional stability, excellent patient-reported outcome measures (PROMs), and completely eliminates the risk of hardware migration, cementing it as the definitive standard of care for unstable sternoclavicular dislocations.
