Primary Plantar Plate Repair Through a Dorsal Approach: A Comprehensive Surgical Guide
Key Takeaway
The dorsal approach for primary plantar plate repair, often combined with a Weil osteotomy, provides excellent visualization and biomechanical restoration of the metatarsophalangeal joint. This technique addresses plantar plate insufficiency by directly repairing the detached ligamentous complex to the proximal phalanx. By shortening the metatarsal, the Weil osteotomy decompresses the joint, facilitating tension-free repair and correcting sagittal plane deformity while restoring toe stability.
Introduction to Plantar Plate Insufficiency
Plantar plate tears and subsequent metatarsophalangeal (MTP) joint instability represent a complex and frequently debilitating pathology in the forefoot. Historically, these deformities were managed with indirect soft-tissue balancing or excisional arthroplasties, which often failed to address the primary anatomic lesion. The evolution of forefoot surgery has shifted toward anatomic restoration.
Although direct repair of a plantar plate detachment can be technically challenging due to the deep plantar location of the structure, it provides superior, durable stability to the joint. Cooper and Coughlin pioneered approaches for adequate exposure of the plantar plate, and Gregg et al. subsequently reported highly successful clinical outcomes when primary plantar plate repair is combined with a Weil osteotomy.
The dorsal approach has become the gold standard for this procedure. It avoids the complications associated with plantar incisions—namely, painful plantar scarring and delayed wound healing—while allowing for simultaneous management of the bony architecture via a Weil osteotomy. This comprehensive guide details the indications, biomechanics, and step-by-step surgical execution of the primary plantar plate repair through a dorsal approach.
Surgical Anatomy and Biomechanics
The plantar plate is a thick, fibrocartilaginous structure composed primarily of type I collagen. It originates from the plantar aspect of the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. It serves as the primary static stabilizer of the MTP joint in the sagittal plane, resisting hyperextension forces during the terminal stance phase of gait.
Pathoanatomically, the vast majority of plantar plate tears occur at the distal insertion site (the base of the proximal phalanx) or just proximal to it. Attenuation or rupture of this structure leads to dorsal subluxation of the proximal phalanx. As the deformity progresses, the intrinsic musculature (lumbricals and interossei) shifts dorsally to the axis of rotation, converting them from plantarflexors to dorsiflexors, thereby exacerbating the crossover toe deformity.
💡 Clinical Pearl: The Role of the Weil Osteotomy
The Weil osteotomy is not merely a corrective procedure for metatarsal length; it is a critical exposure tool. By shortening the metatarsal and shifting the capital fragment proximally, the osteotomy decompresses the MTP joint. This relaxation of the soft tissues is what makes dorsal access to the plantar plate possible without excessive, joint-damaging traction.
Indications and Preoperative Evaluation
Clinical Indications
- Chronic, localized pain at the plantar aspect of the lesser MTP joints (most commonly the second MTP joint).
- Progressive dorsal subluxation or dislocation of the lesser toe.
- Transverse plane deformity (crossover toe).
- Positive dorsal drawer test (Lachman test of the MTP joint) indicating gross sagittal instability.
- Failure of conservative management (taping, orthotics, stiff-soled shoes, NSAIDs).
Imaging Modalities
- Weight-Bearing Radiographs: Essential for evaluating metatarsal cascade, joint congruency, and the presence of subluxation.
- Magnetic Resonance Imaging (MRI): The gold standard for visualizing the integrity of the plantar plate. High-resolution MRI can accurately identify the location and size of the tear, typically demonstrating a fluid cleft at the distal phalangeal insertion.
- Ultrasound: A dynamic, cost-effective alternative to MRI that allows for real-time assessment of the plantar plate during provocative maneuvers.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia or regional anesthesia (popliteal block) combined with monitored anesthesia care.
1. Position the patient supine on the operating table.
2. Place a small bump under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the foot points directly upward.
3. Apply a well-padded calf or thigh tourniquet to maintain a bloodless surgical field, which is critical for visualizing the delicate structures of the MTP joint.
4. Prep and drape the limb in a standard sterile orthopedic fashion.
Surgical Technique: Primary Plantar Plate Repair
1. Incision and Soft Tissue Dissection
Make a dorsal longitudinal incision centered over the affected interspace or directly over the affected MTP joint. Careful blunt dissection is required to protect the dorsal cutaneous nerves and the dorsal venous network.
Perform a longitudinal capsulotomy at the affected MTP joint. To mobilize the extensor mechanism:
* Divide the extensor digitorum brevis (EDB) tendon.
* Perform a Z-tenotomy of the extensor digitorum longus (EDL) tendon to allow for later lengthening and repair.
2. Joint Release and Weil Osteotomy
Achieving adequate exposure requires a complete release of the collateral ligaments. Carefully release the medial and lateral collateral ligaments from their metatarsal origins. This allows the proximal phalanx to be plantarflexed, opening the dorsal joint space.
Using a microsagittal saw, perform a Weil osteotomy. The saw blade should be oriented parallel to the plantar weight-bearing surface of the foot. To prevent plantar displacement of the metatarsal head (which can lead to transfer metatarsalgia), remove a small, 1- to 2-mm wedge of bone from the dorsal aspect of the capital fragment.
3. Joint Decompression and Plantar Plate Exposure
Once the osteotomy is complete, push the metatarsal head proximally. Provisionally fix the toe in a maximally shortened position using a 1.2-mm Kirschner wire (K-wire) driven from dorsal to plantar, securing the capital fragment to the metatarsal shaft.
Apply longitudinal traction to the toe. This maneuver, combined with the shortened metatarsal, provides excellent visualization of the plantar plate.
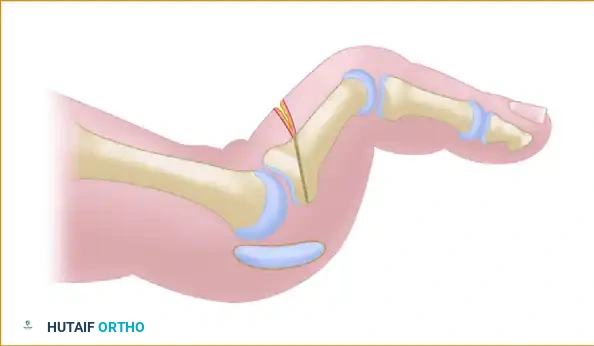
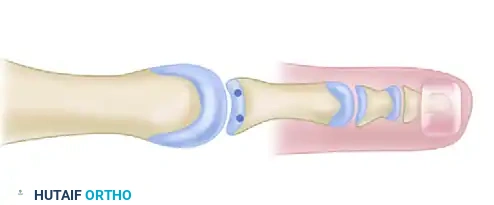
⚠️ Surgical Warning: Footprint Preparation
If the plantar plate is partially or completely detached from the base of the proximal phalanx, it is imperative to freshen the plantar rim of the proximal phalanx. Use a curette or a small motorized burr to decorticate the bone down to a bleeding bed. Failure to adequately prepare this footprint will result in poor biological healing of the fibrocartilage to the bone, leading to recurrent instability.
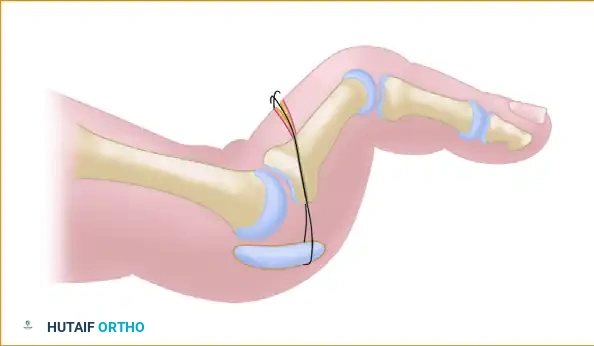
4. Drilling the Proximal Phalanx
With the footprint prepared, the proximal phalanx must be drilled to accept the repair sutures.
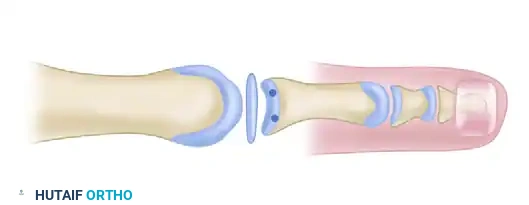
Using a 1.6-mm K-wire, drill two distinct holes from the dorsal cortex of the proximal phalanx, aiming obliquely to exit at the freshened plantar rim. Ensure these holes are placed medially and laterally to create a wide base for the suture bridge, which will maximize the contact area between the plantar plate and the bone.
5. Suture Passing
Passing the suture through the plantar plate can be challenging due to the limited space and the dense nature of the tissue. Use a specialized suture passing device (e.g., a mini-lasso or a pigtail passer).
Pass a heavy, non-absorbable braided suture (such as a 1/10 Ethibond or a modern #0 ultra-high-molecular-weight polyethylene suture) across the plantar plate, proximal to the disruption. Retrieve the suture ends and pass them back through the previously drilled medial and lateral holes in the proximal phalanx, bringing the suture ends out dorsally.
6. Osteotomy Fixation and Plate Advancement
Before tying the plantar plate sutures, the Weil osteotomy must be definitively fixed. Remove the provisional 1.2-mm K-wire. Adjust the metatarsal head to its optimal position (typically 2 to 3 mm of shortening, depending on the preoperative cascade).
Fix the Weil osteotomy using a 1.3-mm or 2.0-mm titanium “twist-off” screw (e.g., DePuy/Johnson & Johnson, Leeds, UK) or a standard cortical screw. Ensure the screw head is countersunk to prevent dorsal impingement.
With the metatarsal rigidly fixed, tie the two suture ends over the dorsal phalangeal cortex. As the knot is secured, the plantar plate is advanced and compressed directly onto the bleeding bony bed of the proximal phalanx base.
7. Joint Pinning
To protect the repair during the initial healing phase, pass a 1.6-mm K-wire longitudinally through the tip of the toe, across the distal and proximal interphalangeal joints, and across the MTP joint into the metatarsal. The toe must be held in a neutral position (0 degrees of dorsiflexion/plantarflexion) during this pinning.
Adjunctive Procedure: Flexor Digitorum Longus (FDL) Transfer
In cases of severe, chronic deformity where the plantar plate is severely attenuated or the tissue quality is exceptionally poor, an FDL transfer may be utilized as an adjunct to augment the repair.
FDL Transfer Technique
- Harvest the FDL tendon distally and route it dorsally.
- Apply tension to the FDL tendon while an assistant holds the ankle in a strict neutral position (90 degrees). This is critical for setting the appropriate resting tension.
- Fixation Option A: Loop the tip of each FDL slip back on itself. Secure it to the trailing edge of each side of the lateral band and to itself using non-absorbable sutures. Section any excess tendon.
- Fixation Option B: Alternatively, suture the two tendon slips to one another over the dorsum of the phalanx. Note that this leaves a small, palpable knot beneath the skin.
- Fixation Option C (Bone Tunnel): In a modification of the technique, after distal release, the FDL can be passed through a drill hole in the proximal phalanx and sutured to the extensor mechanism at the appropriate tension.
Tensioning and Alignment Checks
With the ankle extended to neutral, evaluate the resting cascade of the toes. The MTP joint should rest in a neutral or slightly flexed position. The proximal interphalangeal (PIP) joint should rest in neutral or with less than 10 degrees of flexion.
💡 Clinical Pearl: Sequencing Multiple Digits
If the same procedure is being performed for the central three digits, always correct the second toe first, as it is usually the most severely affected. The FDL tendons of the third and fourth digits will be pulled distally through the common tendon slip in the midsole as the second toe FDL is sutured under tension. Correcting the second toe first makes tension adjustment significantly easier and more accurate in the third and fourth toes.
Closure and Hemostasis
Before closing the skin, deflate the tourniquet. Obtain meticulous hemostasis using electrocautery or gentle compression. Hematoma formation in the dorsal forefoot can lead to severe pain, wound dehiscence, and excessive scarring.
Repair the Z-lengthened EDL tendon at the appropriate resting tension. Close the capsular and subcutaneous layers with absorbable sutures. Close the skin with 4-0 monofilament nylon or a suture of the surgeon’s choice using a tension-free technique (e.g., vertical mattress sutures if swelling is present).
Postoperative Care and Rehabilitation Protocol
The success of a plantar plate repair relies heavily on strict adherence to the postoperative rehabilitation protocol. The repair must be protected from dorsiflexion forces while the fibrocartilage heals to the bone.
- Immediate Postoperative Phase (0-2 Weeks):
- A short-leg, well-padded cast extending past the toes is applied in the operating room.
- The foot must be strictly elevated for the first 48 to 72 hours to minimize edema. Bathroom privileges are allowed.
- Crutches are optional; weight-bearing to tolerance is generally allowed on the heel or flat foot, depending on surgeon preference and bone quality. The patient is usually off crutches within 1 week.
- Intermediate Phase (2-4 Weeks):
- The cast is removed and replaced at the 2-week mark (at which point sutures are typically removed) and again at 4 weeks.
- The transarticular K-wire is generally removed in the clinic between 3 to 4 weeks postoperatively.
- Transition Phase (4-6 Weeks):
- At 4 weeks, the patient is transitioned into a deep, wide toe box, soft-vamp shoe or a rigid postoperative boot.
- Taping the toe in slight plantarflexion is highly recommended to prevent dorsal drift.
- Rehabilitation Phase (6+ Weeks):
- Active toe exercises (plantarflexion) are encouraged at 6 weeks.
- Passive dorsiflexion should be avoided until 8 to 10 weeks to prevent stretching out the repair.
- Return to high-impact activities or sports is typically delayed until 3 to 4 months postoperatively.
Complications and Pitfalls
While highly successful, the dorsal approach to plantar plate repair carries specific risks:
1. Floating Toe Deformity: Often caused by over-lengthening of the metatarsal during the Weil osteotomy or failure to adequately tension the plantar plate/FDL transfer.
2. MTP Joint Stiffness: The most common complication. Strict adherence to the K-wire removal timeline (3-4 weeks) and initiation of active plantarflexion exercises at 6 weeks mitigates this risk.
3. Avascular Necrosis (AVN) of the Metatarsal Head: Rare, but can occur due to aggressive soft tissue stripping combined with the intra-articular osteotomy. Preserve the plantar soft tissue attachments to the capital fragment.
4. Recurrent Instability: Usually secondary to inadequate footprint preparation on the proximal phalanx, poor suture fixation, or premature return to unprotected weight-bearing and dorsiflexion.
You Might Also Like

