Comprehensive Introduction and Patho-Epidemiology
Accessing the posteromedial aspect of the ankle joint presents a unique and formidable anatomical challenge for the orthopedic surgeon. The dense arborization of the deltoid ligament complex, combined with the critical neurovascular structures housed within the tarsal tunnel, makes surgical exposure technically demanding and fraught with potential iatrogenic hazards. Historically, the medial malleolar osteotomy has remained the workhorse approach for massive, centrally or posteriorly located osteochondral lesions of the talus (OLTs). However, while an osteotomy provides unparalleled perpendicular access to the talar dome, it carries inherent and well-documented risks. These include delayed union, nonunion, malunion, intra-articular step-off, and hardware irritation, which collectively contribute to a complication rate approaching 30% in some historical cohorts.
Consequently, joint-sparing posteromedial arthrotomies have been meticulously developed to provide adequate visualization of the posterior talar dome and tibial plafond without the profound morbidity associated with an osseous transection. This paradigm shift towards joint-preserving approaches demands a rigorous understanding of dynamic ankle anatomy. The masterclass detailed in this chapter focuses on two highly effective, evidence-based surgical techniques: the posteromedial arthrotomy through an anteromedial approach (described by Thompson and Loomer) and the trans-sheath approach to the posteromedial ankle through the posterior tibial tendon sheath (described by Bassett et al.).
The patho-epidemiology of conditions necessitating these approaches is heavily skewed toward traumatic and degenerative intra-articular pathologies. Medial osteochondral lesions of the talus typically occur secondary to inversion and plantarflexion injuries. Unlike lateral talar lesions, which are often shallow and anterior, medial OLTs are characteristically deep, cup-shaped, and located in the posterior third of the talar dome. Furthermore, conditions such as synovial chondromatosis, pigmented villonodular synovitis (PVNS), and posterior ankle impingement syndromes (including symptomatic os trigonum or Stieda process pathology) frequently localize to this posterior recess. Mastering these joint-sparing arthrotomies allows the orthopedic surgeon to execute precise excision, curettage, bone grafting, and synovectomy while preserving the structural integrity of the medial mortise.
The Evolution of Posteromedial Access
The evolution of these techniques represents a critical intersection of anatomical discovery and clinical necessity. Early attempts at posterior arthrotomies often resulted in devastating medial instability due to inadvertent transection of the deep deltoid ligament, or profound neurological deficits secondary to tarsal tunnel violation. The techniques pioneered by Thompson, Loomer, and Bassett represent a refined understanding of anatomical "safe zones." By utilizing dynamic joint positioning—specifically extreme plantarflexion and dorsiflexion—the surgeon can sequentially translate the anterior and posterior aspects of the talar dome into a relatively small surgical window, maximizing exposure while minimizing soft tissue disruption.
Pathophysiological Considerations of the Posterior Talus
The posterior talus is uniquely vulnerable to shear forces during the terminal phases of gait, particularly when the ankle is loaded in plantarflexion. The articular cartilage in this region is subjected to high compressive loads, and once an osteochondral fragment becomes unstable, the ingress of synovial fluid into the subchondral bone leads to progressive cyst formation. These subchondral cysts can become massive, undermining the structural integrity of the entire medial talar dome. Arthroscopic management, while highly effective for smaller, superficial lesions, often proves inadequate for large cystic OLTs requiring structural bone grafting. In these scenarios, the open posteromedial arthrotomy provides the necessary access for comprehensive debridement, structural allograft or autograft impaction, and definitive restoration of the articular surface.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of medial ankle anatomy is non-negotiable when executing these approaches. The medial malleolus serves as the primary osseous landmark, but it is the intricate soft-tissue envelope surrounding it that dictates the surgical corridor. The surgeon must navigate a complex layered anatomy, respecting both the static stabilizers of the joint and the dynamic tendinous and neurovascular structures that traverse the region.
Osseous Architecture of the Medial Mortise
The medial malleolus is an extension of the distal tibia, characterized by an anterior colliculus, a posterior colliculus, and an intervening intercollicular groove. The anterior colliculus projects further distally than the posterior colliculus and serves as the primary attachment site for the superficial deltoid ligament. The posterior colliculus, though less prominent, is biomechanically critical as the attachment site for the deep posterior tibiotalar ligament. The intercollicular groove provides a pathway for the posterior tibial tendon. Understanding these osseous landmarks is essential, as the surgical approaches detailed herein rely on identifying these bony contours to safely incise the overlying retinacular structures.
The Deltoid Ligament Complex
The deltoid ligament is a robust, multifascicular structure divided into superficial and deep components. The superficial deltoid (comprising the tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments) primarily resists hindfoot eversion and valgus stress. However, it is the deep deltoid ligament—specifically the deep posterior tibiotalar ligament (DPTTL)—that is the paramount stabilizer of the ankle joint. The DPTTL is a thick, intra-articular but extra-synovial structure that originates from the posterior colliculus and inserts onto the medial surface of the talus. It is the primary restraint against lateral talar excursion and external rotation. The approaches detailed in this chapter are specifically designed to exploit anatomical intervals that remain either anterior or posterior to the DPTTL, thereby preserving this critical structure and preventing disastrous postoperative medial ankle instability.
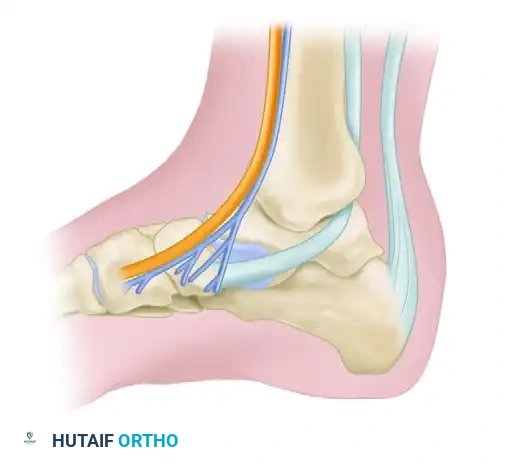
The Tarsal Tunnel and Neurovascular Bundle
Located immediately posterior and inferior to the medial malleolus, the tarsal tunnel is a fibro-osseous space roofed by the flexor retinaculum (laciniate ligament). From anterior to posterior, its contents include the Tibialis posterior tendon, the Flexor Digitorum longus tendon, the Posterior tibial Artery and Vein, the Tibial Nerve, and the Flexor Hallucis longus tendon (often remembered by the mnemonic "Tom, Dick, AND Very Nervous Harry"). The tibial nerve bifurcates within or just distal to the tunnel into the medial and lateral plantar nerves, and gives off the medial calcaneal branches.
Iatrogenic injury to the tibial nerve or its branches can result in debilitating, intractable postoperative neuralgia. Retraction in this area must be deliberate, gentle, and strictly protective. Furthermore, the surgeon must be acutely aware of the saphenous nerve and the great saphenous vein, which course anterior to the medial malleolus. These superficial structures are at high risk during the initial skin incision and superficial dissection of the anteromedial approach.
Exhaustive Indications and Contraindications
The decision to proceed with a posteromedial ankle arthrotomy must be based on a rigorous evaluation of the patient's pathology, functional demands, and the anatomical location of the lesion. While these approaches offer excellent joint-sparing access, they are not universally applicable to all medial ankle pathologies.
Indications for Posteromedial Arthrotomy
These approaches are primarily indicated for the management of complex intra-articular pathologies localized to the posterior half of the medial talar dome or the posterior tibial plafond. The most frequent indication is the surgical management of large, cystic, or structurally unstable osteochondral lesions of the talus (OLTs) that have failed conservative management or previous arthroscopic marrow stimulation. Specifically, lesions that require structural bone grafting, autologous chondrocyte implantation (ACI), or particulate juvenile articular cartilage allografting necessitate the broader exposure provided by an open arthrotomy.
Additional indications include the retrieval of posterior intra-articular loose bodies that are inaccessible via standard anterior arthroscopic portals, particularly in the setting of synovial chondromatosis. Open synovectomy for extensive pigmented villonodular synovitis (PVNS) involving the posterior recess is another strong indication. Furthermore, these approaches can be utilized for the reduction and internal fixation of select posterior pilon fractures or complex medial malleolar fractures with posterior extension, as well as the management of severe posterior ankle impingement syndromes where arthroscopic resection is deemed unsafe or anatomically unfeasible.
Absolute and Relative Contraindications
Absolute contraindications include active superficial or deep infection (unless the procedure is specifically for irrigation and debridement of a septic joint), severe peripheral arterial disease compromising the vascularity of the medial skin flap, and the presence of advanced Charcot neuroarthropathy, which severely distorts the local anatomy and precludes reliable soft-tissue healing.
Relative contraindications revolve around the specific geometry of the lesion. Massive, centrally located OLTs that require perfectly perpendicular access for the insertion of osteochondral autograft transfer system (OATS) plugs may still necessitate a formal medial malleolar osteotomy. If the lesion extends too far anteriorly, a purely posterior approach will provide inadequate visualization, leading to iatrogenic cartilage damage during instrumentation. Severe preexisting medial ankle instability is also a relative contraindication, as the surgical dissection, even when meticulously performed, may exacerbate capsular laxity.
| Category | Specific Conditions | Clinical Rationale / Impact |
|---|---|---|
| Primary Indications | Large/Cystic Posterior Medial OLTs | Allows for structural bone grafting and cartilage restoration techniques not feasible arthroscopically. |
| Primary Indications | Posterior Loose Bodies / Synovial Chondromatosis | Enables complete evacuation of the posterior recess and comprehensive synovectomy. |
| Primary Indications | Complex Posterior Pilon/Malleolar Fractures | Provides direct visualization of the posterior articular surface for anatomical reduction. |
| Absolute Contraindications | Active Local Infection or Cellulitis | High risk of introducing superficial pathogens into the deep articular space. |
| Absolute Contraindications | Severe Peripheral Arterial Disease (PAD) | High risk of medial wound necrosis and catastrophic flap failure. |
| Relative Contraindications | Central OLTs requiring perpendicular OATS | Joint-sparing approaches do not allow the perpendicular drill angle required for OATS plug insertion; osteotomy preferred. |
| Relative Contraindications | Advanced Charcot Neuroarthropathy | Severely distorted anatomy increases neurovascular risk and risk of postoperative breakdown. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful posteromedial arthrotomy. The surgeon must precisely map the intra-articular pathology to determine whether the Thompson/Loomer anteromedial approach, the Bassett trans-sheath approach, or a formal medial malleolar osteotomy is the most appropriate surgical strategy.
Advanced Imaging and Templating
Standard weight-bearing anteroposterior, lateral, and mortise radiographs of the ankle are mandatory to assess overall joint alignment, joint space narrowing, and the presence of macroscopic loose bodies or osteophytes. However, advanced cross-sectional imaging is indispensable. Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating OLTs. The surgeon should utilize a 9-grid anatomical mapping system on the MRI to precisely localize the lesion. T2-weighted sequences are critical for assessing the integrity of the overlying articular cartilage and identifying subchondral edema or cystic changes.
If significant osseous involvement is suspected, a fine-cut Computed Tomography (CT) scan provides superior cortical detail. CT is particularly useful for preoperative templating of structural bone grafts or for mapping the exact size and location of posterior osseous impingement lesions (e.g., a large os trigonum). The surgeon must mentally superimpose the anticipated surgical window over the CT or MRI images to confirm that the planned dynamic maneuvers (plantarflexion/dorsiflexion) will sufficiently expose the target pathology.
Anesthesia and Patient Positioning
The choice of anesthesia typically involves a general anesthetic or a regional neuraxial block (spinal or epidural), supplemented with a popliteal sciatic nerve block and a saphenous nerve block for optimal postoperative analgesia.
Patient positioning is critical and dictates the ease of the surgical approach. While the patient can be placed in the prone position to allow direct posterior access, this severely limits the ability to address concurrent anterior pathology and complicates airway management. Therefore, the supine position with the ipsilateral hip and knee flexed and externally rotated (the "figure-of-four" position) is the most universally accepted and highly recommended setup. A bump is placed under the contralateral hip to facilitate external rotation of the operative limb. This position allows the surgeon to sit comfortably on the medial side of the table, looking directly down onto the medial malleolus, while permitting simultaneous access to the anterior ankle if an anteromedial arthrotomy or arthroscopy is concurrently required.
Tourniquet Application and Equipment Setup
A well-padded pneumatic tourniquet is placed on the proximal thigh or proximal calf. A bloodless surgical field is absolutely critical during these approaches to ensure immediate identification of the fine capsular layers and to prevent inadvertent injury to the posterior tibial artery or tibial nerve. Exsanguination is achieved with an Esmarch bandage prior to tourniquet inflation. The surgical tray must be equipped with specialized retractor systems, including small Ragnell retractors, Senn retractors, mini-Hohmann retractors, and smooth lamina spreaders. For the management of OLTs, specialized ring curettes, microfracture awls, and bone grafting instrumentation must be readily available.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a posteromedial arthrotomy demands meticulous soft-tissue handling and a deep respect for the dynamic mobility of the ankle joint. The two approaches detailed below utilize distinct anatomical corridors but share the common goal of maximizing articular exposure while preserving the deep deltoid ligament.
The Anteromedial Approach with Posterior Extension (Thompson and Loomer)
The Thompson and Loomer technique is an ingenious dual-window concept. It leverages the dynamic mobility of the ankle joint to sequentially expose the anterior and posterior halves of the superomedial talar dome. It is particularly useful for lesions that span the mid-to-posterior aspect of the talus.
1. Superficial Incision and Anterior Exposure
The procedure begins with a 10-cm curved incision, convex posteriorly, centered just posterior to the medial malleolus. This curvilinear design is critical as it allows for the development of both anterior and posterior full-thickness skin flaps without creating apex necrosis. Dissection is carried sharply through the subcutaneous tissues. The surgeon must meticulously identify and protect the great saphenous vein and the saphenous nerve, retracting them anteriorly. The medial joint capsule is exposed anterior to the medial malleolus. A 2-cm longitudinal incision is made in the anteromedial capsule, extending precisely from the distal anterior tibia to the talar neck, taking care not to violate the anterior fibers of the deep deltoid ligament.
2. Dynamic Anterior Inspection
With the anterior window established, the surgeon places a smooth lamina spreader or a mini-Hohmann retractor to separate the tibia and talus. The ankle is then forced into maximal plantarflexion. This dynamic maneuver translates the talus anteriorly, effectively extruding the anterior one-half to two-thirds of the superomedial talar dome out of the mortise. If the osteochondral defect is fully visualized within this window, the surgeon proceeds with definitive treatment—typically sharp excision of the unstable cartilage, aggressive curettage of the necrotic subchondral bone base, and microfracture drilling to stimulate marrow elements.
3. Posterior Extension and Tarsal Tunnel Protection
If the preoperative MRI dictates, or intraoperative inspection reveals, that the lesion extends too far posteriorly to be completely instrumented from the anterior window, the approach must be extended. The skin flap is mobilized posteriorly to expose the flexor retinaculum overlying the posterior tibial tendon. A careful, superficial incision is made in the flexor retinaculum.
At this juncture, strict adherence to anatomical safe zones is required. The surgeon must not expose, dissect, or examine the neurovascular contents of the tarsal tunnel. Instead, a blunt retractor (such as a smooth Langenbeck or a broad Ragnell) is placed over the posterior tibial tendon, and the entire neurovascular bundle is gently retracted posteriorly en masse. Overzealous dissection or skeletonization of the tibial nerve here is the primary cause of catastrophic postoperative tarsal tunnel syndrome.
4. Dynamic Posterior Inspection
With the tarsal tunnel contents safely protected and retracted posteriorly, the ankle is brought out of plantarflexion and forced into maximal dorsiflexion. This maneuver translates the posterior aspect of the talus into the surgical window, posterior to the medial malleolus. The posterior capsule is incised longitudinally. The posterior one-half of the superomedial border of the talus is now visible. The posterior aspect of the lesion is inspected, debrided, and treated with marrow stimulation or bone grafting as indicated.
The Trans-Sheath Approach (Bassett et al.)
The Bassett approach is an elegant, trans-sheath technique that utilizes the posterior tibial tendon itself as a physical barrier to protect the posterior neurovascular bundle. By entering the joint through the deep layer of the tendon sheath, the surgeon gains exceptional access to the posterior mortise while completely sparing the deep posterior tibiotalar fibers of the deltoid ligament.
1. Landmarks and Superficial Incision
The surgeon palpates the medial malleolus and the Achilles tendon. The interval between these two structures forms the surgical corridor. A 5- to 8-cm incision is made immediately overlying the posterior tibial tendon, located just behind the medial malleolus. The incision curves distally and slightly anteriorly, meticulously following the natural contour of the medial malleolus toward the navicular insertion.
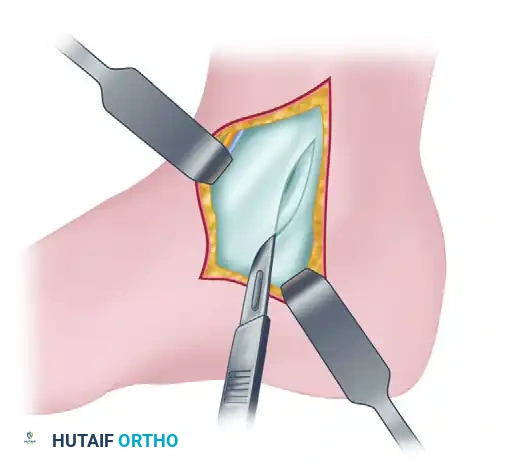
2. Superficial Dissection and Retinacular Incision
The incision is deepened through the subcutaneous tissue. Small crossing venous branches are electrocoagulated. The glistening white fibers of the flexor retinaculum (laciniate ligament) overlying the posterior tibial tendon are identified. The surgeon makes a 5- to 8-cm longitudinal incision directly into the superficial layer of the flexor retinaculum, following the exact curve of the underlying posterior tibial tendon.
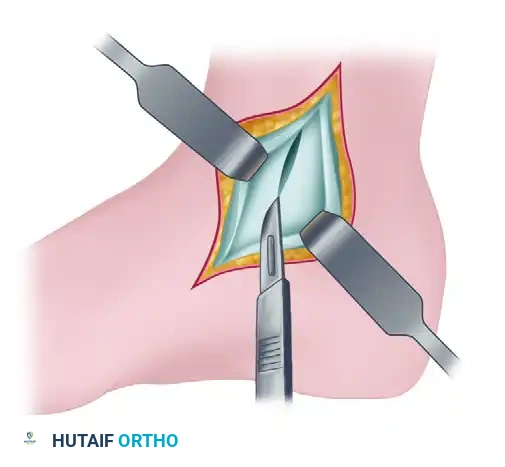
3. Tendon Retraction and Deep Exposure
The posterior tibial tendon is mobilized from its bed. Using a blunt retractor or a Penrose drain, the tendon is retracted posteriorly. This is the biomechanical cornerstone of the Bassett approach: the robust posterior tibial tendon acts as an impenetrable physical shield, protecting the tibial nerve and posterior tibial vessels from any inadvertent injury during the deep capsular dissection.
4. Deep Capsulotomy
With the tendon retracted posteriorly, the deep layer of the flexor retinaculum (which constitutes the deep posterior tibial tendon sheath) and the underlying posterior joint capsule are exposed. The surgeon makes a 3- to 5-cm longitudinal incision through this deep layer and the joint capsule. Precision is crucial here; the scalpel must penetrate the capsule to enter the tibiotalar joint without scoring the adjacent articular cartilage of the talus or tibia.
5. Joint Inspection and Intra-Articular Management
A blunt retractor (such as a mini-Hohmann) is placed through the capsular incision, retracting the capsule anteriorly, while the posterior tibial tendon remains retracted posteriorly. The foot is then moved dynamically into dorsiflexion, plantarflexion, inversion, and eversion. This dynamic manipulation allows the surgeon to comprehensively examine the articular surface of the posterior talus, the posterior tibial plafond, and the posterior joint recess.
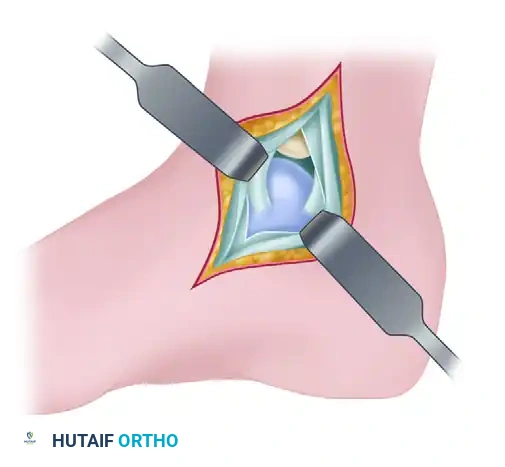
Utilizing the Bassett trans-sheath approach, the surgeon can successfully expose approximately 60% of the posterior talar dome and 50% of the posterior tibial articular surface. Once the target lesion (e.g., an OLT) is visualized, it is managed with specialized angled curettes. The sclerotic base is debrided to bleeding subchondral bone. If microfracture is performed, an awl is used to create holes 3-4 mm apart and 4-5 mm deep to allow the egress of marrow elements. For larger cystic lesions, the cyst is curetted, packed with cancellous autograft (often harvested from the ipsilateral proximal tibia or calcaneus), and sealed with a fibrin glue matrix.
Complications, Incidence Rates, and Salvage Management
While highly effective and generally safe when performed by experienced surgeons, posteromedial arthrotomies carry specific, potentially severe risks. The orthopedic surgeon must actively mitigate these risks through meticulous surgical technique and possess a clear algorithm for salvage management should complications arise.
Neurological Complications
The most devastating complication of a posteromedial arthrotomy is iatrogenic injury to the tibial nerve or its branches, leading to Tarsal Tunnel Syndrome or intractable medial neuralgia. This typically occurs not from direct transection, but from aggressive skeletonization, forceful retraction, or thermal injury from electrocautery. Incidence rates of transient neurapraxia range from 2% to 5%, while permanent neuralgia is rare (<1%) but catastrophic. Prevention relies entirely on utilizing the posterior tibial tendon as a protective barrier (as in the Bassett approach) and avoiding any direct dissection of the neurovascular bundle. If severe, unrelenting neuropathic pain develops postoperatively, early re-exploration and formal tarsal tunnel release may be required as a salvage procedure.
Additionally, injury to the saphenous nerve during the superficial dissection of the anteromedial approach can lead to painful neuromas or medial midfoot numbness. The surgeon must maintain a high index of suspicion for this structure during the initial skin incision.
Tendinopathy and Adhesions
Because the tendon sheath is incised longitudinally (and in the Bassett approach, both superficial and deep layers are violated), postoperative adhesions of the posterior tibial tendon to the underlying capsule or overlying skin are a significant risk. This manifests clinically as medial ankle pain, stiffness, and subjective weakness during active inversion and plantarflexion. The incidence of clinically significant adhesions is estimated at 5% to 10%. The primary defense against this complication is meticulous, layered closure of the tendon sheath (when possible without causing constriction) and, most importantly, the initiation of immediate postoperative range-of-motion (ROM) exercises. If dense adhesions form and fail conservative management (physical therapy, ultrasound-guided hydrodissection), a secondary tenolysis may be indicated.
Inadequate Exposure and Iatrogenic Cartilage Injury
Attempting to access a lesion that is situated too far anteriorly via a purely posterior approach, or vice versa, will lead to immense surgical frustration and high potential for iatrogenic cartilage damage from forced, off-angle instrumentation. If the exposure is deemed inadequate intraoperatively, the surgeon must not force instruments into the joint. Instead, the approach must be extended, or the surgeon must pivot to a formal medial malleolar osteotomy. Precise preoperative MRI templating is the only reliable method to prevent this pitfall.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Tibial Neuralgia / Tarsal Tunnel Syndrome | 2% - 5% (Transient) <1% (Permanent) |
Avoid direct dissection of the NV bundle; utilize PTT as a physical retractor shield. | Gabapentinoids; formal surgical tarsal tunnel release and neurolysis if refractory. |
| Posterior Tibial Tendon Adhesions | 5% - 10% | Meticulous sheath closure; strict adherence to early postoperative ROM protocols. | Aggressive physical therapy; ultrasound-guided hydrodissection; formal surgical tenolysis. |
| Saphenous Nerve Neuroma | 1% - 3% | Careful superficial dissection; anterior retraction of the vein and nerve en bloc. | Diagnostic block; surgical neuroma excision and proximal burying into muscle belly. |
| Medial Ankle Instability | <1% | Strict preservation of the deep posterior tibiotalar ligament (DPTTL) during capsulotomy. | Bracing; formal ligamentous reconstruction (e.g., Deltoid reconstruction with allograft). |
Phased Post-Operative Rehabilitation Protocols
The postoperative management following a posteromedial ankle arthrotomy is intimately dictated by the specific intra-articular pathology addressed. A simple arthrotomy for the removal of a loose body allows for rapid rehabilitation, whereas an extensive debridement and microfracture for a massive OLT requires a highly protected, phased approach to allow for fibrocartilage generation. However, the foundational principles of early motion and progressive loading remain consistent across all indications.
Phase 1: Maximum Protection and Early Motion (Weeks 0-2)
In the operating room, the wound is closed in anatomical layers. A bulky, sterile soft compressive dressing (e.g., a Jones dressing) is applied to minimize hemarthrosis and obliterate dead space. A posterior splint in neutral dorsiflexion is typically applied for the first 48 to 72 hours to provide immediate pain control and soft-tissue rest. However, prolonged immobilization is strictly discouraged.
Immediate, gentle active and active-assisted range-of-motion (ROM) exercises are initiated as soon as the patient's pain allows, typically by postoperative day 3. Early ROM is critical for three reasons: it prevents capsular adhesions, it minimizes posterior tibial tendon tethering within the incised sheath, and it provides the essential mechanical stimulation required for multipotent mesenchymal stem cells to differentiate into fibrocartilage if marrow stimulation was performed. Weight-bearing status is pathology-dependent. For simple loose body removal, weight-bearing as tolerated (WBAT) in a controlled ankle motion (CAM) boot is permitted. If extensive microfracture or bone grafting was performed, the patient is restricted to strict non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) to protect the fragile clot matrix.
Phase 2: Progressive Weight-Bearing and Strengthening (Weeks 2-6)
Sutures are removed at approximately 14 days postoperatively, provided the medial wound demonstrates robust healing. For patients who underwent marrow stimulation, they are typically transitioned from NWB to progressive weight-bearing in a CAM boot over weeks 4 through 6.
Physical therapy during this phase intensifies, focusing on restoring full, symmetric dorsiflexion and plantarflexion. Isometric strengthening is initiated. Particular attention must be paid to posterior tibial tendon rehabilitation. Because the tendon was mobilized and its sheath violated during the surgical approach, targeted inversion strengthening and eccentric loading protocols are essential to restore dynamic medial arch support and prevent chronic tendinopathy.
Phase 3: Advanced Function and Return to Play (Weeks 6-12+)
By week 6, patients are typically transitioned into standard, supportive footwear. The focus of physical therapy shifts toward proprioceptive training (utilizing BAPS boards, single-leg stance exercises, and uneven surface training) to restore neuromuscular control of the ankle mortise. Progressive resistance exercises are advanced.
Return to high-impact activities, running, and competitive
