Operative Management of Phalangeal and Sesamoid Fractures

Key Takeaway
Phalangeal and sesamoid fractures of the foot require precise clinical differentiation and tailored management. While most phalangeal fractures heal with conservative care, displaced intraarticular injuries demand open reduction and internal fixation. Sesamoid fractures, particularly of the tibial sesamoid, present unique biomechanical challenges. Surgical interventions, including partial or complete sesamoidectomy and autogenous bone grafting, are indicated for nonunions or severe comminution, emphasizing the critical restoration of the flexor hallucis brevis mechanism.
PHALANGEAL FRACTURES OF THE TOES
The vast majority of phalangeal fractures of the toes are successfully managed through conservative measures, including buddy taping, rigid-soled footwear, and progressive weight-bearing. Surgical intervention is rarely mandated; however, specific fracture patterns—particularly those involving the great toe—demand meticulous operative management to prevent long-term morbidity, post-traumatic arthritis, and biomechanical dysfunction of the forefoot.
Indications for Operative Intervention
Operative treatment is primarily indicated for intraarticular fractures of the interphalangeal (IP) or metatarsophalangeal (MTP) joints of the hallux that exhibit severe displacement or articular step-off. The great toe plays a critical role in the terminal stance phase of the gait cycle, bearing substantial loads. Failure to restore articular congruity in this digit inevitably leads to rapid degenerative arthritic changes, chronic pain, and significant gait alterations.
Clinical Pearl: A displacement of greater than 2 mm within the intraarticular surface of the hallucal interphalangeal joint is a strong indication for open reduction and internal fixation (ORIF).
Surgical Technique: Open Reduction and Internal Fixation (ORIF)
When surgical intervention is elected, the primary goal is anatomic reduction of the articular surface and stable fixation to allow for early mobilization.
- Surgical Approach: A dorsal or mid-axial longitudinal incision is utilized depending on the fracture geometry. The extensor mechanism is carefully retracted, and the joint capsule is incised to expose the fracture site.
- Reduction: The fracture fragments are cleared of interposed hematoma and periosteum. Anatomic reduction is achieved using small pointed reduction forceps.
- Fixation: Using a power drill, 0.045-inch Kirschner wires (K-wires) are inserted to secure the fragments. Depending on the fracture pattern, crossed K-wires or a single intramedullary wire may be utilized.
- Closure and Pin Management: The K-wires are typically bent and left proud outside the skin to facilitate easy removal in the clinic. The capsule and skin are closed in layers.
Postoperative Protocol:
No cast is strictly required. The patient is placed in a rigid postoperative shoe. Protected, heel-touch weight-bearing can commence as soon as soft-tissue healing permits. The K-wires are generally removed 3 to 4 weeks postoperatively once clinical and radiographic stabilization of the fracture is confirmed.
SESAMOID FRACTURES AND PATHOLOGIES
The hallucal sesamoids are integral components of the first MTP joint complex. Fractures of these structures can be broadly categorized into acute traumatic injuries—often associated with MTP joint dislocations following high-energy trauma—and chronic stress fractures, which are predominantly observed in high-demand athletes such as long-distance runners and ballet dancers.
Biomechanics and Anatomy of the Hallucal Sesamoids
The sesamoids are embedded within the tendons of the flexor hallucis brevis (FHB) muscle. They serve three primary biomechanical functions:
1. Absorbing weight-bearing forces transmitted through the first metatarsal head.
2. Increasing the mechanical advantage (lever arm) of the FHB.
3. Protecting the flexor hallucis longus (FHL) tendon as it glides between them.
The medial (tibial) sesamoid is larger, bears a greater proportion of the load, and is seated more directly beneath the metatarsal head compared to the lateral (fibular) sesamoid. Consequently, the tibial sesamoid is significantly more susceptible to both acute fractures and chronic stress injuries.
Clinical Evaluation and Differential Diagnosis
Diagnosing a sesamoid fracture requires a high index of suspicion. The mechanism of injury is typically either direct (axial loading producing a comminuted fracture) or indirect (violent hyperextension of the first MTP joint, common in turf sports).
Patients typically present with:
* Point tenderness directly over the affected sesamoid.
* Localized plantar swelling.
* Pain exacerbated by passive extension of the great toe.
* An antalgic gait characterized by a shortened stance phase and avoidance of toe-off.
The Bipartite Sesamoid Conundrum:
A significant diagnostic challenge is differentiating an acute fracture from a bipartite sesamoid, which occurs in 5% to 30% of asymptomatic individuals. While bipartite sesamoids can be bilateral, a singular sesamoid in the contralateral foot does not definitively confirm a fracture on the symptomatic side; it may represent a symptomatic synchondrosis of a bipartite sesamoid.
Diagnostic Pitfall: Do not rely solely on contralateral radiographs. To differentiate a fracture from a bipartite sesamoid, evaluate the fragment morphology. Fractured sesamoids typically exhibit roughly equal-sized fragments with irregular, jagged, and uncorticated edges. Conversely, bipartite sesamoids usually present as one large and one small fragment with smooth, rounded, corticated margins.
If the fracture is minimally displaced, the differential diagnosis must also include osteochondritis dissecans (OCD) of the sesamoid, osteonecrosis (avascular necrosis), and generalized sesamoiditis.
Radiographic and Advanced Imaging
A comprehensive radiographic series is mandatory:
* Standard AP and Lateral Views: The forefoot should be in slight pronation during the lateral view to properly profile the sesamoids.
* Oblique Views: The medial oblique view isolates the tibial sesamoid, while the lateral oblique view isolates the fibular sesamoid.
* Axial Sesamoid View: Essential for evaluating the articular surface, joint space narrowing, and subchondral sclerosis associated with osteochondritis.
When plain radiographs are equivocal, advanced imaging is warranted. Computed Tomography (CT) provides excellent bony detail for assessing fracture comminution and healing. Radionuclide bone scanning can confirm an active osseous process; however, Chisin et al. caution that 26% to 29% of asymptomatic individuals exhibit increased uptake in the sesamoids. Therefore, bone scan results must be strictly correlated with clinical findings. Magnetic Resonance Imaging (MRI) is increasingly preferred over bone scans due to its superior ability to detect bone marrow edema and evaluate the integrity of the plantar plate and FHB mechanism.
MANAGEMENT OF SESAMOID FRACTURES
Nonoperative Management Protocols
Minimally displaced or nondisplaced acute fractures, as well as stress fractures, should initially be managed nonoperatively.
1. Immobilization: A short leg cast incorporating a toe plate is applied for 3 to 4 weeks to strictly immobilize the first MTP joint.
2. Re-evaluation: If symptoms persist, a second period of casting for an additional 3 to 4 weeks may be necessary.
3. Transition: Following cast removal, the patient is transitioned to an athletic shoe modified with a lightweight steel shank and a toe rocker to limit MTP dorsiflexion during gait.
Indications for Surgical Intervention
Surgical intervention is indicated for:
* Widely displaced fractures (>5 mm) associated with disruption of the FHB musculotendinous unit.
* Fractures that fail to unite after prolonged conservative management (nonunion).
* Severe comminution with loss of articular cartilage.
* Painful bipartite sesamoids that are refractory to conservative care.
Surgical Technique: Open Reduction and Internal Fixation
For acute, widely displaced fractures where the fragments are of roughly equal size, ORIF is the treatment of choice to restore the FHB mechanism.
* Fixation: An 18-gauge wire is looped around the proximal and distal poles of the sesamoid in a figure-of-eight configuration.
* Biologic Augmentation: Autogenous bone grafting, harvested from the calcaneus or the supramalleolar area of the distal tibia, is often packed into the fracture site to promote union.
SESAMOIDECTOMY: COMPLETE AND PARTIAL
Historically, complete excision of a fractured sesamoid was the standard of care following failed conservative treatment. However, due to the critical biomechanical role of the sesamoids—particularly the tibial sesamoid in maintaining the lever arm of the FHB and preventing hallux valgus—modern orthopedic practice favors partial excision or bone grafting whenever feasible.
If partial excision is planned, the patient must be counseled preoperatively that the remaining fragment may eventually require excision if symptoms persist. Complete sesamoidectomy is reserved for severely comminuted fractures devoid of large fragments or cases with profound articular cartilage destruction.
Surgical Warning: Excision of the tibial sesamoid carries a risk of iatrogenic hallux valgus, while excision of the fibular sesamoid can lead to hallux varus. Meticulous repair of the intrinsic musculature and joint capsule is paramount to preventing these deformities.
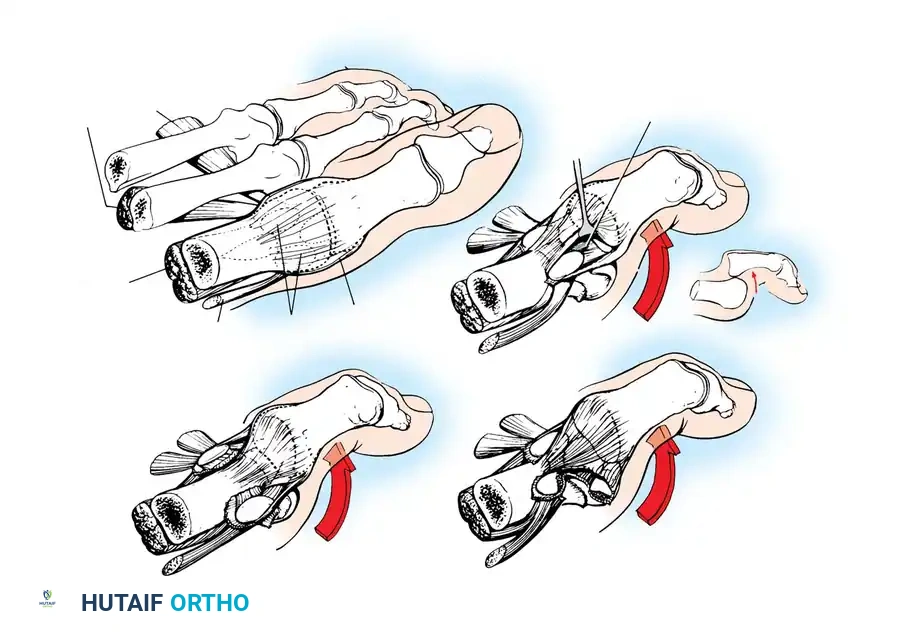
Technique 86-19: Sesamoidectomy
- Incision and Exposure: Make a medial longitudinal incision centered just plantar to the midline of the first MTP joint. Incise the capsule longitudinally in line with the skin.
- Joint Evaluation: Evaluate the intraarticular portion of the sesamoid to assess cartilage quality and fragment mobility. Inspect the plantar surface of the first metatarsal head for corresponding chondral damage.
- Nerve Protection: Approach the sesamoid via an extracapsular route. It is critical to identify and protect the proper medial plantar nerve to the hallux, which emerges plantarly at the musculotendinous junction of the abductor hallucis muscle. Gently retract this nerve plantarly.
- Excision: Make an incision directly over the sesamoid. Perform either a complete enucleation or a partial excision of the fragmented/necrotic portion.
- FHB Repair (Critical Step): The defect in the flexor brevis mechanism must be robustly repaired. Use a 2-0 nonabsorbable polyethylene suture. If a partial excision was performed, use a 0.045-inch K-wire to drill holes in the remaining sesamoid fragment, securing the FHB tendon directly to the bleeding cancellous surface.
- Closure: Repair the joint capsule with 2-0 absorbable sutures and close the skin with nylon.
Postoperative Protocol (Sesamoidectomy):
The patient is placed in a short leg plaster splint, rendering the hallux completely immobile. The patient is strictly non-weight-bearing for 3 to 4 weeks. Subsequently, a short leg walking cast is applied for an additional 4 weeks (total 8 weeks of immobilization). Upon cast removal, a soft medial longitudinal arch support and a firm-soled shoe are prescribed. Active range-of-motion exercises are initiated, progressing to passive stretching as tolerated.
BONE GRAFTING FOR SESAMOID NONUNION
For active patients and athletes with a symptomatic sesamoid nonunion, autogenous bone grafting is an excellent joint-preserving alternative to excision. Anderson and McBryde demonstrated high rates of bony union and return to preinjury activity levels using this technique.
Technique 86-20: Autogenous Bone Grafting (Anderson and McBryde)
- Incision: Make a 5-cm longitudinal skin incision along the medial plantar aspect of the first ray, centered over the MTP joint.
- Capsular Approach: Identify the capsule and abductor hallucis tendon. Divide them in line with the skin incision, entering the joint dorsal to the tibial sesamoid.
- Articular Inspection: Retract the tissues to expose the articular surface of the sesamoid. If severe cartilaginous destruction is present, abort the grafting procedure and proceed with excision. If the cartilage is intact, proceed with extraarticular bone grafting.
- Extraarticular Exposure: Dissect plantar to the abductor hallucis tendon to expose the plantar aspect of the tibial sesamoid. Strictly avoid injury to the plantar digital nerve.
- Preparation of the Nonunion: Following sharp periosteal elevation, identify the nonunion site. Gross motion is often palpable. Using a small dental curet, meticulously debride all fibrous and necrotic tissue from the nonunion interface without violating the dorsal articular cartilage. (Send debrided tissue for histological examination).
- Graft Harvesting and Placement: Harvest cancellous autogenous bone graft locally through a small cortical window created in the medial eminence of the first metatarsal head. Pack this graft tightly into the sesamoid defect. The intact tendinous expansion surrounding the sesamoid usually provides sufficient stability, keeping the fragments in close apposition without the need for internal hardware.
- Closure: Meticulously approximate the periosteal layers and close the wound with absorbable sutures.
Postoperative Protocol (Bone Grafting):
A short leg cast with a toe plate is applied. Weight-bearing is delayed for 2 to 3 weeks, followed by transition to a walking brace. Gentle range-of-motion exercises begin at 2 to 3 weeks. Light jogging may resume at 8 weeks. Tomography or CT scanning is recommended at 10 to 12 weeks to definitively assess bony union, as radiographic healing can lag clinically.
OSTEOCHONDRITIS AND OTHER SESAMOID CONDITIONS
Osteochondritis of the Sesamoid:
Osteochondritis is characterized radiographically by a deformed, fragmented sesamoid with irregular areas of sclerosis and radiolucency, best visualized on an axial radiograph or CT scan. While the exact etiology remains debated, repetitive microtrauma is considered the primary catalyst. Management must exhaust all nonsurgical modalities—specifically, orthotics featuring a sesamoid relief well, a lateral forefoot post, and a full-length steel shank—before any surgical excision is contemplated.
Sesamoiditis and Intractable Plantar Keratoses:
"Sesamoiditis" is a broad, often vague clinical diagnosis encompassing peritendinous inflammation, bursitis, and chondromalacia. Surgical intervention for pure sesamoiditis should be delayed indefinitely until every conservative measure has failed. Other associated pathologies, such as intractable plantar keratoses (IPK) beneath the sesamoid or localized nerve impingement, require highly specific, tailored interventions, often involving offloading orthoses or, rarely, precise plantar condylectomy of the metatarsal head rather than primary sesamoidectomy.
You Might Also Like