Mastering Peroneal Tendon Subluxation and Occult Hindfoot Derangements

Key Takeaway
Chronic lateral ankle pain often masks complex underlying pathologies when standard ligamentous stress tests are negative. This comprehensive guide explores the diagnosis and surgical management of peroneal tendon subluxation, sinus tarsi syndrome, and occult hindfoot lesions. It provides step-by-step operative techniques, including peroneus longus tendon transfers, and details evidence-based postoperative rehabilitation protocols essential for restoring hindfoot biomechanics and achieving optimal patient outcomes.
INTRODUCTION TO CHRONIC LATERAL ANKLE PAIN
The evaluation of chronic lateral ankle pain requires a high index of suspicion and a meticulous clinical examination. While chronic lateral ankle instability secondary to anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) attenuation is the most common etiology, a subset of patients will present with persistent disability despite negative stress tests. In these scenarios, the orthopedic surgeon must pivot the diagnostic algorithm to evaluate for occult derangements.
These elusive conditions primarily include peroneal tendon subluxation and dislocation, occult hindfoot lesions (such as tarsal coalitions or subtle fractures), sinus tarsi syndrome, osteochondral impingement ridges, and osteochondritis dissecans (OCD) of the talus. Mastery of these pathologies is essential for the practicing foot and ankle surgeon to prevent prolonged patient morbidity and recurrent surgical failures.
PERONEAL TENDON SUBLUXATION AND DISLOCATION
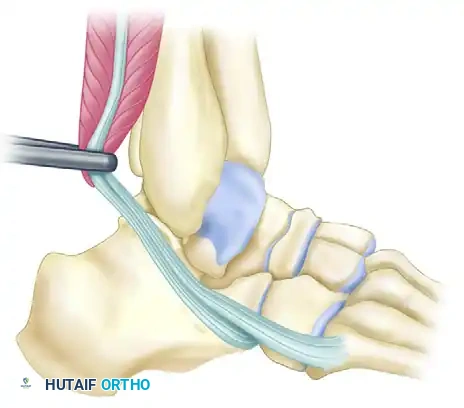
Peroneal tendon subluxation and dislocation typically result from a traumatic disruption or attenuation of the superior peroneal retinaculum (SPR), often combined with a congenitally shallow retromalleolar fibular groove. When conservative management fails, or in the presence of chronic, symptomatic instability that compromises hindfoot kinematics, surgical reconstruction is mandated.
While primary SPR repair and fibular groove deepening are standard for isolated lesions, complex cases involving severe hindfoot valgus or revision scenarios may require robust tenodesis or tendon transfer techniques utilizing the peroneus longus to restore stability and correct talar tilt.
Advanced Surgical Reconstruction: Peroneus Longus Transfer
In cases of profound instability where the talus exhibits significant valgus tilt and standard retinacular repairs are insufficient, a complex rerouting of the peroneus longus can be employed to act as a dynamic and static checkrein.
Surgical Pearl: The success of this procedure relies heavily on precise tunnel placement. Violation of the articular surfaces of the talus or the tibial plafond will lead to rapid joint degeneration. Fluoroscopic guidance is mandatory during tunnel drilling.
Step-by-Step Operative Technique:
- Talar Tunnel Creation and Graft Passage:
Identify the peroneus longus tendon and prepare the graft. Drill a tunnel through the body of the talus, directing the guide pin from lateral to medial. Pass the peroneus longus graft through the talar tunnel. Apply strict tension to the graft and secure it at the medial end of the tunnel using an appropriately sized interference screw. - Tibial Tunnel Creation:
Create a second osseous tunnel starting at the tip of the medial malleolus, specifically within the intercollicular groove. Angle this tunnel proximally and laterally at approximately 60 degrees so that it exits in the distal third of the tibia, just anterior to the fibula.
> Surgical Warning: Extreme care must be taken during the trajectory planning and drilling of this tibial tunnel to avoid violating the medial articular surface of the tibial plafond. - Graft Routing and Tensioning:
Retrieve the peroneus longus graft from the medial talus and bring it through the newly created tibial tunnel, passing it from medial to lateral. Apply rigorous graft tensioning while manually reducing the valgus tilt of the talus to restore neutral hindfoot alignment. - Lateral Fixation:
Secure the exiting peroneus longus graft onto the lateral border of the tibia. A combination of a tenodesis screw and a supplemental staple is highly preferred for rigid biomechanical fixation. Alternatively, the graft can be secured directly to the fibula utilizing a screw post or a spiked washer, depending on bone quality and surgeon preference. - Concomitant Deformity Correction:
The procedure will fail if underlying structural deformities are ignored. It is absolutely essential to correct any concurrent foot deformities that drive recurrence, including hindfoot valgus, midfoot abduction, or first ray elevation. Medializing calcaneal osteotomies or first tarsometatarsal arthrodesis should be performed as indicated.
Postoperative Rehabilitation Protocol
Strict adherence to the postoperative protocol is critical to allow for osseous integration of the tendon transfer and healing of any concomitant osteotomies.
- Weeks 0-2: The patient is placed in a well-padded posterior splint with U-shaped stirrups. The ankle is locked in a strictly neutral position.
- Weeks 2-8: Sutures are removed at the 2-week mark. A solid, short-leg cast is applied with the ankle maintained in neutral. The patient remains strictly non-weight bearing (NWB).
- Weeks 8-10: At 8 weeks post-surgery, the patient is transitioned to a removable controlled ankle motion (CAM) boot. Gentle, active range of motion (ROM) exercises are initiated, but the patient must remain NWB.
- Weeks 10-12: Formal physical therapy commences. The patient begins progressive weight bearing within the CAM boot, utilizing a custom orthotic to support the corrected hindfoot alignment. By this stage, the tendon transfer and osteotomies should demonstrate clinical and radiographic healing.
- Week 12 and Beyond: The patient is advanced to a regular supportive shoe equipped with a custom orthotic insert. High-impact activities are restricted until functional strength is fully restored.
INTERNAL DERANGEMENTS OF THE ANKLE AND HINDFOOT
As previously established, if stress tests of the ankle (anterior drawer and talar tilt) are negative, yet the patient continues to experience profound pain and disability, occult internal derangements must be investigated. The differential diagnosis should immediately expand to include:
1. Occult hindfoot lesions (coalitions, subtle fractures, neoplasms).
2. Sinus tarsi syndrome.
3. Osteochondral ridges (impingement overuse syndromes).
4. Osteochondritis dissecans (OCD) of the talus.
OCCULT LESIONS OF THE TALUS AND CALCANEUS
Tarsal Coalition
Tarsal coalition frequently produces symptoms that perfectly mimic a chronic ankle sprain, particularly in the adolescent population. Snyder et al. documented that adolescents with underlying tarsal coalitions experience a statistically significant increase in the frequency of ankle sprains due to altered hindfoot kinematics and loss of subtalar accommodation. Clinical examination may reveal peroneal spastic flatfoot. High-resolution Computed Tomography (CT) scans are the gold standard for identifying fibrous, cartilaginous, or osseous coalitions, particularly at the middle facet of the talocalcaneal joint or the calcaneonavicular interval.
Talar Neoplasms
Benign and malignant neoplasms of the hindfoot can present insidiously, masquerading as chronic mechanical pain. Eosinophilic granuloma and Pigmented Villonodular Synovitis (PVNS) are notable examples that can erode the talus or invade the subtalar joint, causing deep, aching pain that is unresponsive to standard sprain protocols.
FIGURE 89-33 A: Talar neoplasms, which may mimic chronic ankle sprain. Eosinophilic granuloma demonstrating a lytic lesion within the talar body.

FIGURE 89-33 B: Pigmented villonodular synovitis (PVNS) invading the talus and surrounding articular spaces.
Occult Fractures
Subtle fractures of the hindfoot are frequently missed on initial plain radiographs in the emergency department.
Fracture of the Anterior Process of the Calcaneus:
Often resulting from an inversion and plantarflexion injury (avulsion by the bifurcate ligament), this fracture causes pinpoint tenderness just distal and anterior to the lateral malleolus. If conservative treatment (immobilization) fails and non-union occurs, surgical excision of the fracture fragment yields excellent clinical results.

FIGURE 89-34: Fracture of the anterior process of the calcaneus. After conservative treatment failed, the fracture fragment was excised with good results.
Avulsion Fractures of the Talus:
Lateral process fractures of the talus (often termed "snowboarder's fractures") or other talar avulsions can lead to chronic lateral pain and subtalar joint incongruity. Advanced imaging, including bone scans and CT, is highly sensitive for detecting these lesions when plain films are equivocal.

FIGURE 89-35 A: Bone scan demonstrating intense focal uptake in the lateral aspect of the talus, indicative of an occult avulsion fracture.

FIGURE 89-35 B: CT scan confirming the precise anatomical location and displacement of the talar avulsion fracture.
SINUS TARSI SYNDROME
Historical Context and Definition
First described by O’Connor in 1958, "sinus tarsi syndrome" is characterized by persistent pain localized to the sinus tarsi that lasts for months or even years following the nonoperative treatment of an inversion ankle sprain. Despite its prevalence in clinical practice, the condition remains poorly defined in the literature. The hallmark physical finding is exquisite, localized tenderness in the lateral region of the ankle, specifically over the sinus tarsi.
Pathoanatomy and Etiology
The etiology of sinus tarsi syndrome is multifactorial and heavily debated:
* Subtalar Instability: Some authors suggest the syndrome is a subtle, localized variation of subtalar instability.
* Soft Tissue Degeneration: Anatomical and histological studies have demonstrated extensive scarring, fat pad atrophy, and degenerative changes within the soft tissue elements of the sinus tarsi (including the cervical and interosseous talocalcaneal ligaments).
* Neurological Dysfunction: Others propose that the primary driver is an initial nerve injury within the sinus tarsi that results in a profound loss of proprioceptive function, leading to microtrauma and chronic inflammation.
Advanced Imaging Diagnostics
- Subtalar Arthrography: Taillard et al. historically recommended subtalar arthrography to establish the diagnosis. Normal arthrograms display multiple microrecesses and interdigitations within the joint capsule, particularly near the interosseous and cervical ligaments. Taillard suggested that the absence of these microrecesses and an abrupt cutoff of contrast dye at the interosseous ligament strongly correlate with sinus tarsi syndrome. Goossens et al. supported this, noting less marked microrecesses, anterior ganglions, capsular retraction, and a "frozen" subtalar joint appearance in 27 patients. However, Clanton and Schon were unable to conclusively confirm these arthrographic findings as pathognomonic.
- Magnetic Resonance Imaging (MRI): MRI has largely superseded arthrography. In 1993, Klein and Spreitzer noted that the absence of anterior microrecesses could be a normal variant (found in 46 of 90 normal studies), likely reflecting a lack of iatrogenic joint distention rather than pathology. However, in 33 patients with clinical sinus tarsi syndrome, MRI consistently revealed evidence of fibrosis, chronic synovitis, nonspecific inflammatory changes, and synovial cysts. Furthermore, Lektrakul et al. (2001) demonstrated that reconstructed MRI arthrograms perpendicular to the interosseous talocalcaneal and cervical ligaments are highly sensitive for diagnosing specific ligamentous tears. Ganglion cysts within the sinus tarsi are also frequently identified as a primary source of space-occupying pain.
Diagnostic Injections
Clinical Pearl: The diagnostic injection is the most critical step in confirming sinus tarsi syndrome. If the precise injection of a local anesthetic agent (often combined with a corticosteroid) into the sinus tarsi does not provide at least temporary, complete relief of symptoms, the diagnosis is highly questionable, and other pathologies must be sought.
In many instances, a therapeutic injection provides permanent resolution of the inflammatory cycle. However, if significant pain recurs after the anesthetic wears off, despite a period of temporary relief, surgical intervention may be indicated.
Surgical Management
When conservative measures and injections fail, surgical debridement of the sinus tarsi yields favorable outcomes. Across four major series (Brown, O’Connor, Regnauld, and Taillard et al.) reporting on 96 surgically treated patients, results were excellent in 69% (66 patients), good in 24, and poor in only six.
Surgical Techniques and Philosophies:
* O’Connor: Advocated for the complete excision of the "fat pad in the sinus tarsi and resection of the superficial ligamentous floor," reporting complete pain relief in the majority of his cohort.
* Taillard et al.: Recommended a more conservative approach, confining the excision strictly to the tissue filling the lateral 1.0 to 1.5 cm of the sinus tarsi. This limitation is crucial to avoid iatrogenic damage to the delicate blood supply of the talus, which traverses the medial aspect of the tarsal canal.
* Regnauld: Advised meticulous curettage of the fatty neurovascular tissue within the sinus, while strictly preserving the interosseous ligament unless it is visibly torn or irreparably damaged.
* Clanton and Schon: Emphasized the preservation of both the interosseous talocalcaneal and cervical ligaments whenever possible. Their technique focuses on the targeted resection of the inflamed fibrofatty tissue and the fibrotic extensions originating from the inferior extensor retinaculum.
Differential Diagnosis Warning:
Surgeons must remain vigilant. We have encountered patients who perfectly fit the clinical profile of sinus tarsi syndrome—presenting with chronic, localized pain post-sprain with no obvious ligamentous laxity. However, advanced imaging eventually revealed discrete osteoblastic lesions within the calcaneus. Excision of these occult bone lesions provided immediate and complete relief, underscoring the necessity of comprehensive imaging before committing to soft-tissue debridement of the sinus tarsi.
📚 Medical References
- Peroneal tendon subluxation in athletes: fi bular groove deepening and retinacular reconstruction, Foot Ankle Int 26:436, 2005.
- Raatikainen T, Karpakka J, Orava S: Repair of partial quadriceps tendon rupture: observation of 28 cases, Acta Orthop Scand 65:154, 1994.
- Roberts C, Rosenblum S, Uhl R, et al: Surgical treatment of Achilles tendon rupture, Orthop Rev 18:513, 1989.
- Roels J, Martins M, Mulier JC, et al: Patellar tendinitis (jumper’s knee), Am J Sports Med 6:363, 1978.
- Ruland RT, Dunbar SR, Bowen JD: The biceps squeeze test for diagnosis of distal biceps tendon ruptures, Clin Orthop Relat Res 437:128, 2005.
- Sanches-Sotelo J, Morrey BF, Adams RA, et al: Reconstruction of chronic ruptures of the distal biceps tendon with use of an Achilles tendon allograft, J Bone Joint Surg 84A:999, 2002.
- Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: outcome after repair of acute and chronic injuries, Am J Sports Med 28:9, 2000.
- Schepsis AA, Leach RE: Surgical management of Achilles tendinitis, Am J Sports Med 15:308, 1987.
- Scuderi C: Ruptures of the quadriceps tendon: study of twenty tendon ruptures, Am J Surg 95:626, 1958.
- Shah MK: Outcomes in bilateral and simultaneous quadriceps tendon rupture, Orthopedics 26:797, 2003.
- Shelbourne KD, Darmelio MP, Klootwyk TE: Patellar
You Might Also Like