Peroneal Tendon Repair and Reconstruction: Advanced Surgical Guide
Key Takeaway
Peroneal tendon repair and reconstruction are critical procedures for addressing lateral hindfoot pain and instability caused by traumatic or attritional ruptures. This comprehensive guide details the biomechanical principles, precise surgical techniques—including tenodesis, superior peroneal retinaculum reinforcement, and concurrent lateral ligament stabilization—and evidence-based postoperative protocols necessary to restore dynamic ankle stability and prevent recurrent subluxation in high-demand patients.
INTRODUCTION TO PERONEAL TENDON PATHOLOGY
Peroneal tendon disorders encompass a spectrum of pathologies ranging from tenosynovitis and tendinosis to acute ruptures, attritional tears, and chronic subluxation. The peroneus longus and peroneus brevis tendons serve as the primary dynamic stabilizers of the lateral ankle and hindfoot. When conservative management fails, surgical intervention via Peroneal Tendon Repair and Reconstruction becomes imperative to restore biomechanical function, alleviate debilitating lateral hindfoot pain, and prevent progressive hindfoot varus deformity.
This comprehensive guide delineates the advanced surgical management of peroneal tendon ruptures, detailing the nuances of primary repair, tenodesis, superior peroneal retinaculum (SPR) reconstruction, and the management of concurrent lateral ankle instability.
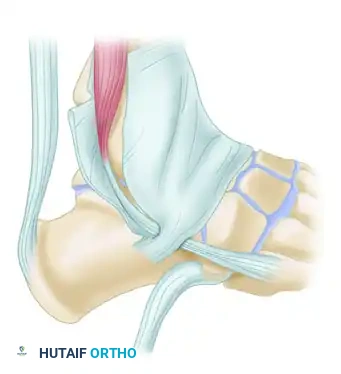
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the lateral ankle anatomy is non-negotiable for the operating surgeon.
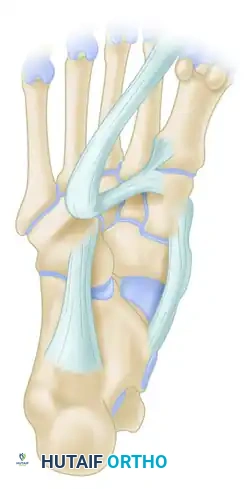
- Peroneus Brevis (PB): Originates from the distal two-thirds of the lateral fibula and inserts onto the base of the fifth metatarsal. It is the primary evertor of the foot. Within the retromalleolar groove, the PB lies anterior and medial to the peroneus longus, directly against the fibula, making it highly susceptible to mechanical attrition and longitudinal split tears.
- Peroneus Longus (PL): Originates from the proximal lateral fibula, courses posterior to the PB in the retromalleolar groove, wraps around the cuboid, and inserts onto the plantar aspect of the medial cuneiform and the base of the first metatarsal. It acts to plantarflex the first ray and evert the foot.
- Superior Peroneal Retinaculum (SPR): The primary static restraint preventing anterior subluxation of the peroneal tendons. It originates from the posterolateral ridge of the distal fibula and inserts onto the lateral calcaneal wall.
- Os Peroneum: A sesamoid bone located within the PL tendon at the level of the calcaneocuboid joint. It is present in approximately 20% of the population and can be a site of attritional rupture.
Clinical Pearl: The peroneal tendons share a common synovial sheath proximal to the lateral malleolus, which bifurcates at the level of the peroneal tubercle. A watershed hypovascular zone exists in both tendons at the turn of the lateral malleolus, predisposing them to degenerative tearing.
PREOPERATIVE EVALUATION AND INDICATIONS
Clinical Presentation
Patients typically present with posterolateral ankle pain, swelling, and a sensation of weakness or instability. Physical examination must localize the site of rupture. If the examination localizes the pathology to the lateral aspect of the hindfoot distal to the superior peroneal retinaculum, a limited incision may suffice. However, a more extensile approach is usually required to mobilize the proximal stump for adequate repair.
Indications for Surgery
- Acute or chronic ruptures of the peroneus brevis or longus.
- Intractable tendinosis or longitudinal split tears failing 3–6 months of conservative care.
- Recurrent peroneal tendon subluxation/dislocation.
- Attritional ruptures associated with an enlarged peroneal tubercle or os peroneum syndrome.
SURGICAL TECHNIQUE: STEP-BY-STEP APPROACH
1. Patient Positioning and Anesthesia
The procedure is performed under general or regional anesthesia. The patient is placed in the lateral decubitus position, or supine with a substantial bump under the ipsilateral hip to internally rotate the leg, providing unhindered access to the posterolateral ankle. A thigh tourniquet is applied and inflated after exsanguination.
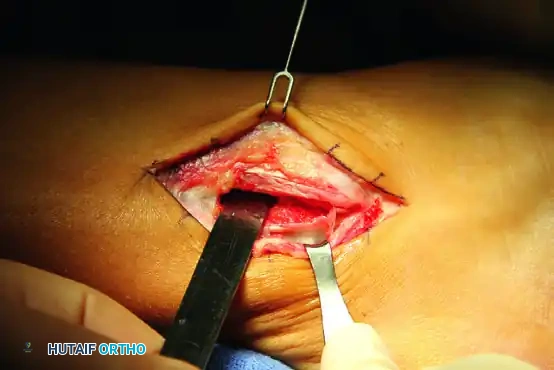
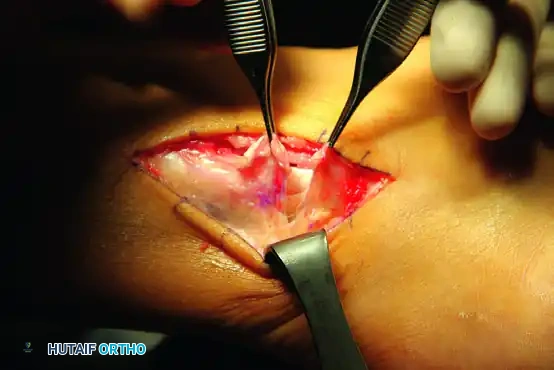
2. Incision and Exposure
An extensile posterolateral incision is utilized. The incision follows the posterior border of the fibula, extending distally toward the base of the fifth metatarsal or the cuboid, depending on the anticipated location of the pathology.
- Carefully dissect through the subcutaneous tissues.
- Identify and protect the sural nerve and the lesser saphenous vein, which typically cross the surgical field distally.
- Expose the superior peroneal retinaculum (SPR).
Surgical Warning: Aggressive retraction of the skin flaps can lead to sural nerve neuropraxia or postoperative wound necrosis. Maintain full-thickness fasciocutaneous flaps.
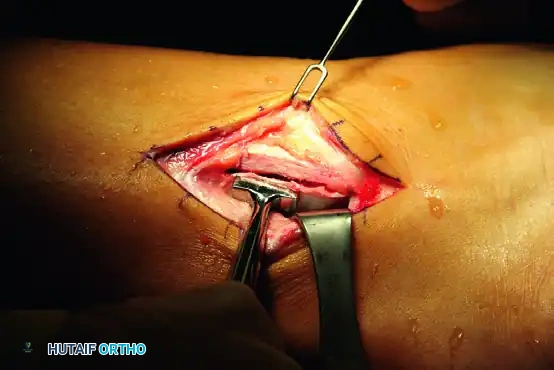
3. Retinaculum Incision and Tendon Assessment
Incise the SPR longitudinally, leaving a 2 to 3 mm cuff of tissue attached to the posterior border of the fibula to facilitate later repair.
Inspect both the peroneus brevis and longus tendons. Assess for longitudinal split tears, complete ruptures, or severe tendinosis.
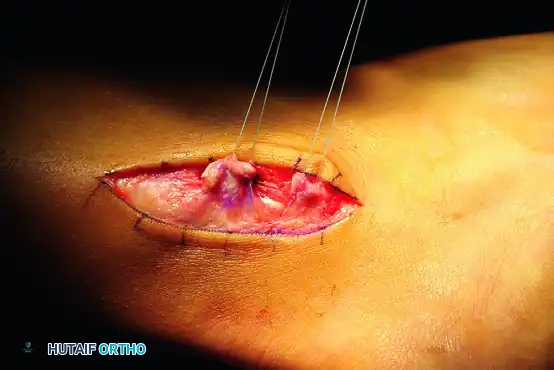
4. Management of Tendon Ruptures
A. Double Tendon Rupture (Rare)
If both tendons are ruptured—a scenario uncommon in standard traumatic injuries—attempt to repair both primarily. Use a robust 2-0 or 0 nonabsorbable suture (e.g., FiberWire or Ethibond) using a modified Kessler or Krackow technique. Ensure the repair is tubularized.
B. Single Tendon Rupture and Tenodesis
If one tendon is severely degenerated or irreparably ruptured (often the peroneus brevis) while the other remains intact, a tenodesis is indicated.
* Debride the degenerative segments of the ruptured tendon.
* Suture the proximal and distal stumps of the ruptured tendon to the adjacent intact tendon (side-to-side tenodesis) using 2-0 nonabsorbable sutures.
C. Attritional Rupture of the Peroneus Longus (Cuboid Level)
Attritional ruptures of the peroneus longus frequently occur beneath the cuboid, often associated with the os peroneum.
- Identify the attritional rupture site.
- Resect the distal end of the ruptured peroneus longus 1 to 2 cm plantarward. If an os peroneum (sesamoid) is present within this degenerative segment, it must be excised concurrently to prevent ongoing impingement.
- Perform a tenodesis: Suture the proximal end of the peroneus longus to the intact peroneus brevis tendon.
- Critical Positioning: This tenodesis must be performed under moderate tension while the foot is held in mild equinovalgus. This ensures appropriate resting tension and prevents postoperative over-lengthening.
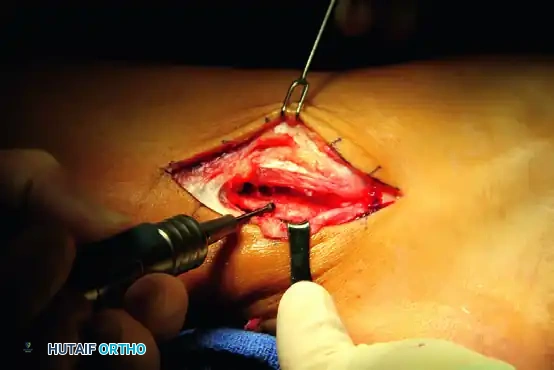
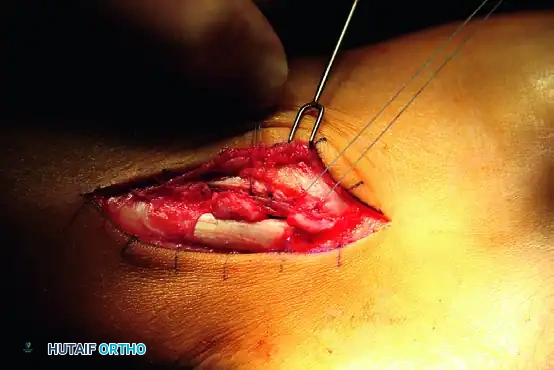
5. Fibular Groove Deepening and SPR Reconstruction
To prevent postoperative subluxation, the retromalleolar groove may require deepening, and the SPR must be meticulously reconstructed.
- If the fibular groove is shallow or convex, perform a groove-deepening procedure. Use a high-speed burr to decorticate the cancellous bone beneath the cortical floor, then tamp the cortical floor down to create a concave sulcus.
- Prepare the fibula for SPR reattachment. Place suture anchors (e.g., Acuflex anchors or equivalent 2.5mm to 3.0mm anchors) along the posterolateral ridge of the fibula. Alternatively, drill transosseous tunnels.

- Pass the sutures through the SPR. Firmly secure the retinaculum to the fibula, ensuring the tendons glide smoothly without subluxation during dynamic ankle range of motion.
The "Trapdoor" Reinforcement Technique
In cases of severe retinacular attenuation, a periosteal flap is utilized to reinforce the repair.

- Create a posteriorly based "trapdoor" using the periosteum from the anterior aspect of the lateral fibula.
- Turn this periosteal trapdoor back over the tendons.
- Suture it directly on top of the repaired superior peroneal retinaculum to provide a robust, double-layered reinforcement.
6. Concurrent Lateral Ankle Ligament Repair
Peroneal tendon pathology is frequently accompanied by chronic lateral ankle instability. Failure to recognize and treat concurrent lateral ankle instability can lead to recurrent laxity, altered kinematics, and subsequent failure of the peroneal tendon repair.
- Extend the incision distally with anterior retraction of the full-thickness flaps.
- Identify the attenuated anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL).
- Perform a primary repair or imbrication (Modified Broström-Gould technique) using suture anchors placed into the distal fibula.
7. Final Assessment and Closure
Before closure, a rigorous dynamic assessment is mandatory.
- Subluxation Test: Place the ankle through a full range of motion, applying eversion stress and tension on the peroneus longus tendon. Verify that the tendons remain stable within the retromalleolar groove.
- Laxity Test: Test the tightness of the lateral ankle ligament repair with a gentle anterior drawer test. Compare this with the preoperative laxity noted under anesthesia.
- Deflate the tourniquet and achieve meticulous hemostasis.
- Perform routine layered closure. Use 2-0 or 3-0 absorbable sutures for the subcutaneous tissue and nonabsorbable monofilament or staples for the skin.
- Apply a sterile, compressive soft-tissue dressing followed by a rigid posterior splint or short-leg cast with the ankle in neutral dorsiflexion and slight eversion.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative protocol must balance the protection of the delicate tendon and retinacular repairs with the prevention of arthrofibrosis. The protocol varies slightly depending on the nature of the repair.
Standard Repair / Tenodesis Protocol
- Weeks 0 to 2: The patient is kept strictly non-weight-bearing (NWB) in the initial posterior splint or cast. Elevation is critical to manage edema.
- Weeks 2 to 6: At the 2-week mark, sutures are removed. A short-leg walking cast or a rigid controlled ankle motion (CAM) boot is applied. The patient may begin progressive weight-bearing as tolerated.
- Weeks 6 to 10: The cast or boot is removed. An air splint or functional lace-up ankle brace is applied and worn for an additional 4 weeks.
- Physical Therapy: Formal rehabilitation begins at week 6. Initial focus is on active and active-assisted range of motion (avoiding extreme inversion). Peroneal strengthening exercises (isometric progressing to isotonic) are initiated. Proprioceptive training is integrated as strength improves.
Protocol for End-to-End Attritional Rupture Repair
If a tendon was repaired end-to-end at an attritional rupture site (which inherently carries a higher risk of re-rupture due to compromised tissue quality), a more conservative orthotic approach is mandated.
* The initial 6-week protocol remains similar (NWB progressing to protected weight-bearing).
* Months 3 to 6: Following the removal of the cast, the patient is transitioned to a double-upright brace with limited ankle motion and an outside T-strap. This brace is worn for 3 to 6 months to mechanically unload the repaired tendon and prevent excessive inversion stress while the tendon undergoes the prolonged remodeling phase of healing.
COMPLICATIONS AND PITFALLS
- Sural Nerve Injury: The most common complication. Meticulous dissection and avoidance of aggressive retraction are paramount. Neuromas can be highly debilitating.
- Recurrent Subluxation: Often due to inadequate deepening of the fibular groove, failure to repair the SPR under appropriate tension, or missed lateral ankle instability.
- Overtightening of the Tenodesis: Suturing the PL to the PB under excessive tension or in excessive dorsiflexion can lead to a fixed eversion contracture and lateral column overload. Always set tension in mild equinovalgus.
- Adhesions and Stiffness: Prolonged immobilization beyond the recommended timeframes can lead to tethering of the tendons within the reconstructed retinaculum. Early, protected range of motion is essential.
By adhering to these rigorous anatomical principles and precise surgical techniques, orthopedic surgeons can reliably restore lateral hindfoot stability and achieve excellent functional outcomes in patients with complex peroneal tendon pathology.
You Might Also Like


