INTRODUCTION TO ORTHOPAEDIC NONUNIONS
The development of a nonunion represents a profound failure of the physiological bone-healing cascade, often precipitated by mechanical instability, compromised vascularity, or inadequate initial reduction. The operative management of these complex scenarios demands a rigorous, evidence-based approach tailored to the specific anatomical region. This comprehensive guide delineates the biomechanical principles, preoperative planning, and step-by-step surgical techniques required to successfully manage nonunions of the pelvis, acetabulum, clavicle, proximal humerus, and femoral neck.
PELVIS AND ACETABULUM NONUNIONS
Nonunions and delayed unions of the pelvic ring are debilitating conditions that require meticulous surgical intervention. Patients typically present with a constellation of symptoms, including chronic pain, a pronounced limp, mechanical instability, and progressive clinical deformity.
Classification and Biomechanics
Pennal and Massiah classified pelvic nonunions into three primary groups based on the original deforming force vectors:
* Anteroposterior Compression (APC): Characterized by symphyseal diastasis and external rotation of the hemipelvis, often leading to anterior instability and posterior sacroiliac (SI) joint disruption.
* Lateral Compression (LC): Driven by internal rotation forces, frequently resulting in impacted sacral fractures and overriding pubic rami fractures.
* Vertical Shear (VS): The most unstable pattern, involving complete osteoligamentous disruption with cephalad displacement of the hemipelvis.
CLINICAL PEARL: In pelvic nonunions, the sacroiliac region typically exhibits an avascular nonunion pattern, necessitating aggressive decortication and robust autogenous bone grafting. Conversely, the pubic rami often present with hypervascular (hypertrophic) nonunions, where rigid stabilization alone may suffice to achieve union.
Clinical Presentation and Imaging
Insufficient immobilization and inadequate initial reduction are the primary culprits behind pelvic nonunions. Diagnostic imaging is paramount for surgical planning:
* Standard Radiographs: Anteroposterior (AP) views provide a baseline assessment.
* Pennal Views: Cephalad (Outlet) and caudal (Inlet) tangential views taken at 45 degrees relative to the standard AP projection are critical. The Inlet view assesses anterior-posterior translation and internal/external rotation, while the Outlet view evaluates vertical displacement.
* Computed Tomography (CT): High-resolution CT with 3D reconstructions is the gold standard for defining the exact osseous anatomy, identifying avascular fragments, and planning the trajectory of internal fixation.
Surgical Management and Techniques
Historically, nonoperative treatment yielded poor functional outcomes. Pennal and Massiah noted that of 24 patients treated nonoperatively, only five returned to their pre-injury employment. In stark contrast, operative stabilization and bone grafting result in high rates of solid bony union and functional restoration. Mears and Velyvis reported 79% excellent and 21% satisfactory results following bone grafting and realignment procedures.
Surgical Steps for Pelvic Nonunion:
1. Patient Positioning: Depending on the nonunion site, the patient is placed supine (for anterior ring) or prone (for posterior ring) on a radiolucent Jackson table.
2. Surgical Approach: The ilioinguinal or modified Stoppa approach is utilized for anterior pathology, while a posterior approach is used for the sacroiliac complex.
3. Debridement and Decortication: The nonunion site is radically debrided of fibrous tissue down to bleeding, punctate bone (the "paprika sign").
4. Reduction: Specialized pelvic reduction forceps (e.g., Jungbluth clamps) are applied to correct multiplanar deformities.
5. Bone Grafting: Copious autologous cancellous bone graft, typically harvested from the iliac crest, is packed into the defect.
6. Rigid Internal Fixation: Multi-hole reconstruction plates (3.5 mm or 4.5 mm) are contoured to the pelvic brim or posterior pelvis to provide absolute stability.
Acetabular Nonunions
Acetabular nonunions are exceedingly rare, typically occurring only in the context of widely displaced, unreduced articular fragments. Letournel and Judet reported a mere four nonunions out of 569 acutely fixed acetabular fractures. When they do occur, treatment requires complex intra-articular osteotomies, structural grafting, and occasionally, conversion to total hip arthroplasty (THA) if post-traumatic arthrosis is advanced.
CLAVICULAR NONUNIONS
While nonunion of clavicular fractures is generally rare, the midshaft is the most common anatomical site for nonunion due to its high overall incidence of fracture. Lateral clavicular fractures, however, carry the highest rate of nonunion per fracture.
Etiology and Biomechanics
Clavicular nonunions are frequently secondary to severe initial trauma, significant fragment displacement, soft tissue interposition, or refracture. The biomechanical environment of the clavicle is complex, subjected to the suspensory forces of the trapezius and the inferior pull of the pectoralis major and deltoid.
SURGICAL WARNING: Symptomatic nonunions of the middle third of the clavicle must be treated with rigid internal fixation. Conservative management of established symptomatic nonunions universally fails to relieve pain or restore shoulder girdle mechanics.
Surgical Indications and Approaches
Operative intervention is indicated for patients exhibiting pain, weakness, and cosmetic deformity.
- Resection Arthroplasty: When the nonunion is located within 4 to 5 cm of either the acromioclavicular or sternoclavicular joint, and the fragment is small, resection of the short fragment may be performed.
- Rigid Internal Fixation: The gold standard for midshaft nonunions is compression plating combined with autologous iliac crest bone grafting. Davids et al. emphasize the importance of opening and reaming the sclerotic medullary canal to restore endosteal blood flow.
- Vascularized Bone Grafting: For highly recalcitrant cases, such as radiation-induced pathological fractures or post-infectious nonunions, Fuchs et al. demonstrated success utilizing a free vascularized graft harvested from the medial femoral condyle, combined with robust plate fixation.
Surgical Technique for Midshaft Clavicular Nonunion:
1. Approach: A superior or anteroinferior incision is made along the clavicular axis, preserving the supraclavicular nerves where possible.
2. Preparation: The fibrous nonunion is excised. The medullary canals of both the medial and lateral fragments are drilled to open the intramedullary space.
3. Grafting: Corticocancellous autograft from the iliac crest is contoured to fit the defect.
4. Plating: A specially contoured, low-profile locking clavicle plate is applied. Compression is achieved across the nonunion site using eccentric drilling techniques.

Figure A: Preoperative radiograph demonstrating a hypervascular nonunion of the clavicle. The patient presented with severe pain and instability 1.5 years following the initial fracture, exacerbated by a recent fall.
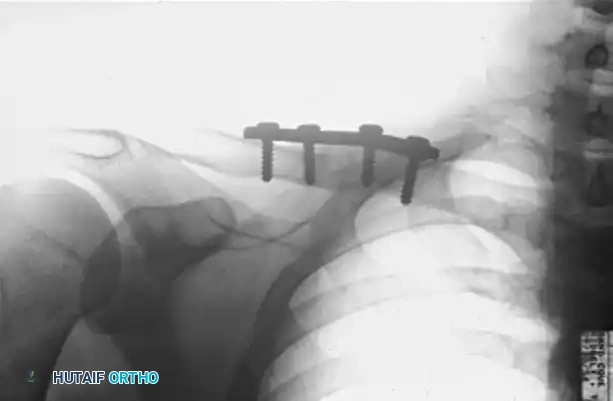
Figure B: Postoperative radiograph at 2.5 months demonstrating solid osseous union following aggressive decortication, application of a superior compression plate, and autologous bone grafting.
PROXIMAL HUMERUS NONUNIONS
Nonunions of the proximal humerus present a unique biomechanical challenge due to the multidirectional deforming forces exerted by the rotator cuff musculature. The proximal fragment is often osteopenic, making standard screw purchase precarious and leading to a high risk of hardware pullout.
Tension Band and Buttress Plate Technique
To counteract these deforming forces, Healy, Jupiter, Kristiansen, and White described a highly effective combination technique utilizing a buttress plate augmented with heavy tension band wiring.
Biomechanical Rationale:
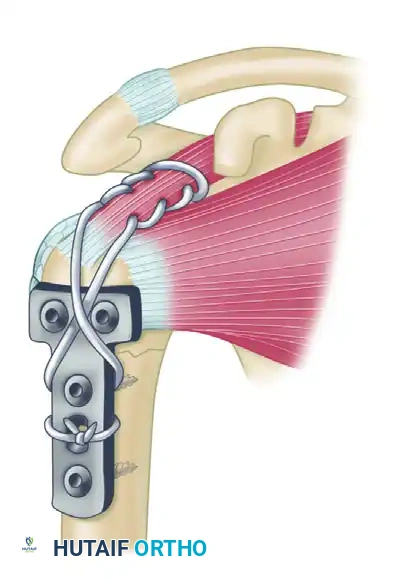
The supraspinatus and infraspinatus exert a powerful superior and posterior pull on the greater tuberosity fragment. By weaving a heavy nonabsorbable suture through the rotator cuff tendon insertions and anchoring it directly to the plate, the surgeon neutralizes the muscular pull. This converts the distracting forces into compressive forces across the fracture site and protects the proximal metaphyseal screws from catastrophic pullout.
Step-by-Step Execution:
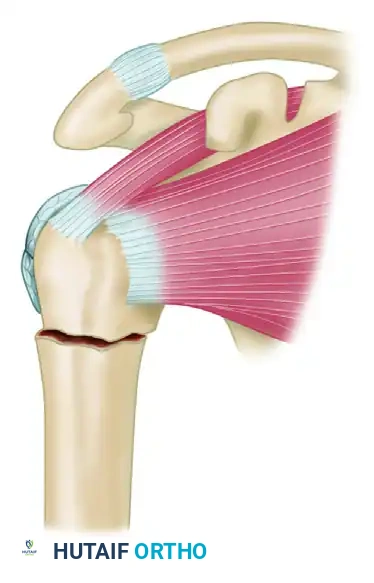
Step 1: Identification of the nonunion site. The proximal fragment is subjected to superior displacement by the supraspinatus, while the humeral shaft is pulled medially by the pectoralis major.
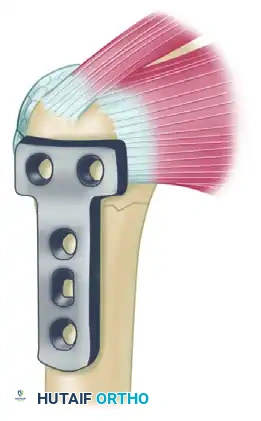
Step 2: Following debridement of the nonunion and bone grafting, a T-plate or proximal humeral locking plate is applied to the lateral aspect of the humerus to provide a rigid buttress.
Step 3: A heavy, nonabsorbable suture (e.g., #5 FiberWire) is woven through the rotator cuff utilizing a Krackow stitch configuration. The suture is then passed through the proximal holes of the plate and tied securely in a figure-of-eight fashion, effectively neutralizing the pull of the rotator cuff on the proximal fragment.
FEMORAL NECK NONUNIONS
Nonunion of the femoral neck is a devastating complication that threatens the viability of the femoral head and the biomechanical integrity of the hip joint. Treatment algorithms are dictated by the patient's physiological age, the viability of the femoral head (assessed via MRI or intraoperative bleeding), and the chronicity of the nonunion.
Angulation Osteotomy
The angulation (valgus-producing) osteotomy is a powerful joint-preserving procedure based on Pauwels' biomechanical principles. It is primarily indicated for younger patients (typically under 60 years of age) with a viable femoral head.
Biomechanical Principles:
Femoral neck nonunions often fail due to excessive vertical shear forces (Pauwels Type III fractures). The angulation osteotomy is designed to change the inclination of the fracture surfaces, converting destructive shear forces into constructive compressive forces that promote osteogenesis. Additionally, it shifts the mechanical axis and line of weight-bearing medially, reducing the bending moment on the hip.
Surgical Evolution and Outcomes:
Historically, this osteotomy was fraught with complications due to inadequate fixation methods. The introduction of the Blount blade plate revolutionized the procedure by holding the fragments securely without the need for external spica casting. Today, the osteotomy is typically stabilized using variable-angled dynamic hip screws (DHS) or specialized locking side plates. Modern literature reports union rates ranging from 86% to 88% following this procedure.
CLINICAL PEARL: The functional outcome of an angulation osteotomy is directly proportional to the mechanical and physiological status of the nonunion prior to surgery. While function can approach normal if the head is viable and union is achieved, surgeons must counsel patients that excellent early results may degrade over 3 to 5 years due to progressive post-traumatic arthritic changes.
Prosthetic Replacement
Prosthetic replacement (hemiarthroplasty or total hip arthroplasty) offers an immediate, definitive solution to femoral neck nonunions, particularly in the elderly population.
Indications:
* Age: Generally reserved for patients older than 60 years.
* Head Viability: Indicated in adults younger than 50 to 60 years old only if the femoral head is avascular (avascular necrosis) and an arthrodesis is deemed undesirable.
* Arthritis: Hemiarthroplasty is strictly contraindicated if there is pre-existing traumatic or primary osteoarthritis of the acetabulum; in such cases, Total Hip Arthroplasty (THA) is the mandatory procedure.
While prostheses were historically overutilized due to poorly defined indications, modern orthopaedics reserves them for specific physiological profiles. It is important to note that complication rates (such as dislocation and periprosthetic fracture) are higher when performing arthroplasty for nonunions compared to acute fractures, necessitating meticulous surgical technique and soft-tissue balancing.
Arthrodesis
Hip arthrodesis is a salvage procedure that is rarely performed in the modern era of advanced arthroplasty, but it remains a viable option in highly specific scenarios—particularly in young, heavy laborers with unilateral hip pathology and a non-viable femoral head.
According to Gill, the primary advantages of an arthrodesis for nonunion of the femoral neck are absolute freedom from pain and permanent mechanical stability. However, the profound alteration in gait kinematics and the subsequent accelerated degeneration of the lumbar spine and contralateral knee make this a procedure of last resort.
POSTOPERATIVE PROTOCOLS
Regardless of the anatomical site, the postoperative management of surgically treated nonunions requires a delicate balance between protecting the osteosynthesis and preventing soft-tissue contractures.
- Pelvis: Patients are typically restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) on the affected side for 8 to 12 weeks, pending radiographic evidence of bridging callus. Deep vein thrombosis (DVT) prophylaxis is mandatory.
- Clavicle: The arm is supported in a sling for 2 to 4 weeks. Pendulum exercises begin immediately, but active elevation above 90 degrees and heavy lifting are restricted until clinical and radiographic union is confirmed (usually 8 to 10 weeks).
- Proximal Humerus: Passive range of motion (PROM) is initiated early to prevent adhesive capsulitis. Active range of motion (AROM) is delayed until 6 weeks to protect the tension band construct and allow the tuberosities to heal.
- Femoral Neck (Osteotomy): Protected weight-bearing with crutches or a walker is required for 8 to 12 weeks. Serial radiographs are scrutinized for maintenance of the valgus correction and progressive obliteration of the nonunion line.
