Partial Articular Fractureplate Fixation: Restore Anatomy

Key Takeaway
We review everything you need to understand about Partial Articular Fractureplate Fixation: Restore Anatomy. Partial articular fractureplate fixation addresses displaced intraarticular fractures, particularly those of the posterior distal tibia, to restore anatomical congruity and joint function. This open reduction internal fixation procedure often employs buttress plates to stabilize the fracture, ensuring proper length, alignment, and rotation for weight-bearing joints. This approach is crucial for complex ankle injuries.
Introduction and Epidemiology
Partial articular fractures, classified under the AO/OTA alphanumeric system as Type B fractures, represent a complex subset of orthopedic injuries where a portion of the articular surface is disrupted while the remainder of the joint remains in continuity with the metaphyseal and diaphyseal regions. The fundamental objective in the surgical management of these fractures is the restoration of articular congruity and the provision of absolute stability to permit early, active mobilization. Unlike extra-articular or diaphyseal fractures where relative stability and secondary bone healing via callus formation are acceptable, partial articular fractures demand anatomic reduction and primary bone healing to mitigate the risk of post-traumatic osteoarthritis.

The epidemiology of partial articular fractures exhibits a classic bimodal distribution. High-energy trauma, such as motor vehicle collisions and falls from significant heights, predominantly accounts for these injuries in the younger, active demographic. In this cohort, fractures are frequently characterized by severe soft tissue compromise, marked displacement, and significant comminution (e.g., split-depression tibial plateau fractures or high-energy pilon variants). Conversely, low-energy mechanisms, typically ground-level falls, are responsible for partial articular fractures in the elderly population. This demographic presents unique challenges, including osteopenia or osteoporosis, which compromises implant purchase and increases the propensity for articular impaction and secondary subsidence.
Historically, the management of these injuries was fraught with complications, including joint stiffness, malunion, and rapid chondral degeneration secondary to prolonged immobilization. The paradigm shifted dramatically with the establishment of the Arbeitsgemeinschaft für Osteosynthesefragen (AO) principles. The contemporary approach emphasizes meticulous soft tissue handling, direct visualization of the articular surface, interfragmentary compression utilizing lag screws, and the application of a buttress or neutralization plate to counteract axial, shear, and torsional forces.
Surgical Anatomy and Biomechanics
Articular Morphology and Cartilage Physiology
The articular surface is composed of hyaline cartilage, a highly specialized, avascular, and aneural tissue that relies on the diffusion of synovial fluid for nutrition. This diffusion is mechanically driven by joint motion and physiological loading. When a partial articular fracture occurs, the resulting step-off or gap disrupts the tribological properties of the joint, leading to focal areas of increased contact stress. Biomechanical studies indicate that articular step-offs greater than 2 millimeters exponentially increase peak contact pressures, precipitating chondrocyte apoptosis and extracellular matrix degradation. Therefore, the surgical anatomy dictates that the subchondral bone must be perfectly aligned to restore the congruent cartilaginous arc.
Biomechanics of Interfragmentary Compression
The cornerstone of partial articular fracture fixation is interfragmentary compression, typically achieved via lag screw technique. A lag screw is not a specific type of screw, but rather a biomechanical function. By overdrilling the near cortex (gliding hole) and engaging only the far cortex (thread hole), the tightening of the screw head against the near cortex compresses the fracture fragments together. This compression generates immense friction across the fracture plane, effectively neutralizing shear forces and providing the absolute stability required for direct osteonal remodeling (Haversian canal bridging) without callus formation.

Principles of Buttress Plating
While lag screws provide excellent interfragmentary compression, they possess minimal resistance to bending and shear forces when subjected to physiological loads. Therefore, partial articular fractures subjected to axial loading (e.g., tibial plateau, distal femur, distal radius) require the application of a buttress plate.
The buttress plate functions by rigidly opposing the direction of displacement. Biomechanically, the plate must be applied to the apex of the fracture (the axilla) to effectively counteract shear forces. When the joint is loaded, the articular fragment attempts to slide along the fracture plane; the buttress plate acts as a physical barrier, converting the shear force into compressive force across the fracture site.

To optimize the buttress effect, the plate is typically slightly under-contoured. When the plate is secured to the intact diaphyseal bone, the under-contouring causes the proximal portion of the plate to spring against the metaphyseal flare, actively compressing the articular fragment. Screws placed through the plate into the articular fragment are inserted in a neutralization capacity or as secondary lag screws, but the primary mechanical stability is derived from the plate's buttressing effect against the intact cortical shaft.
Indications and Contraindications
The decision to proceed with operative intervention for a partial articular fracture is predicated on a careful assessment of fracture morphology, patient physiology, and soft tissue integrity. The overriding goal is the prevention of post-traumatic arthrosis through the restoration of joint kinematics.

Operative vs Non Operative Management Parameters
| Parameter | Operative Indications | Non-Operative Indications |
|---|---|---|
| Articular Displacement | Step-off or gap > 2mm | Non-displaced or < 2mm step-off |
| Joint Stability | Clinical or radiographic instability (e.g., subluxation) | Stable joint through full range of motion |
| Axial Alignment | Metaphyseal/Diaphyseal malalignment > 5 degrees | Acceptable alignment maintained in cast/brace |
| Soft Tissue Status | Open fractures, compartment syndrome | Intact soft tissue envelope, unresolving severe edema (relative) |
| Patient Factors | Physiologically active, compliant with rehab | Non-ambulatory, severe medical comorbidities, extreme non-compliance |
| Associated Injuries | Concomitant ligamentous avulsions requiring repair | Isolated injury amenable to conservative care |
Contraindications to Immediate Plate Fixation
Immediate internal fixation is strictly contraindicated in the presence of compromised soft tissues. The "wrinkle sign" must be present before definitive surgical incisions are made. Operating through fracture blisters, severe ecchymosis, or massive edema exponentially increases the risk of deep infection and wound dehiscence. In such scenarios, damage control orthopedics utilizing joint-spanning external fixation is mandated until the soft tissue envelope recovers.

Pre Operative Planning and Patient Positioning
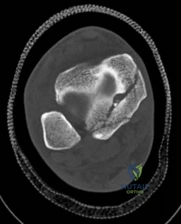
Advanced Imaging and Three Dimensional Mapping
Standard orthogonal radiographs (anteroposterior and lateral) are sufficient for initial diagnosis, but they routinely underestimate the complexity of partial articular fractures. A high-resolution computed tomography (CT) scan with two-dimensional multiplanar reformats (coronal and sagittal) and three-dimensional surface rendering is considered the standard of care.
CT imaging is critical for:
1. Identifying the exact location and size of the articular fragments.
2. Detecting central articular depression that is obscured by the cortical rim on plain films.
3. Mapping fracture lines extending into the diaphysis.
4. Planning the surgical approach to ensure direct access to the primary fracture line.

Surgical Templating
Digital or acetate templating is a mandatory step in preoperative planning. The surgeon must determine the appropriate plate morphology (e.g., T-plate, L-plate, pre-contoured anatomic locking plate), screw trajectories, and the necessity for structural bone graft or bone void fillers to support depressed articular segments. Templating ensures that the chosen implants will adequately capture the fragments without penetrating the joint space.

Patient Positioning and Operating Room Setup
Positioning is dictated by the specific anatomical location of the fracture. However, universal principles apply:
* Radiolucent Table: Essential for unimpeded fluoroscopic access in multiple planes.
* Tourniquet Application: Utilized for extremity fractures to provide a bloodless field, crucial for direct visualization of the articular cartilage.
* Fluoroscopy Positioning: The C-arm must be positioned to allow true orthogonal views of the joint without moving the patient's extremity, which could displace provisional reductions.
* Limb Positioning: For lower extremity injuries (e.g., tibial plateau), a bump under the ipsilateral hip prevents external rotation, and a sterile triangle or ramp facilitates knee flexion to relax the deforming forces of the gastrocnemius.

Detailed Surgical Approach and Technique
The surgical execution for partial articular fractures follows a rigorous, algorithmic sequence: Exposure, Joint Visualization, Reduction, Provisional Fixation, and Definitive Plating. We will utilize the lateral tibial plateau fracture (AO/OTA 41-B) as the archetypal model to describe these steps.
Surgical Exposure and Internervous Planes
An anterolateral approach to the proximal tibia is standard for lateral plateau fractures. The incision is centered over Gerdy's tubercle, extending proximally to the joint line and distally along the anterior crest of the tibia.
Deep dissection involves elevating the anterior tibialis muscle off the lateral tibial face. It is imperative to maintain full-thickness fasciocutaneous flaps to preserve the vascular supply to the skin.

Arthrotomy and Joint Visualization
To achieve anatomic reduction, the surgeon must visualize the articular surface directly. A submeniscal arthrotomy is performed by incising the coronary ligaments, allowing the lateral meniscus to be elevated superiorly with a stay suture. The joint is thoroughly irrigated to remove hematoma and osteochondral debris.
Articular Reduction Techniques
Partial articular fractures typically present as a split (Type B1), depression (Type B2), or split-depression (Type B3).
1. Split Fractures: The peripheral fragment is hinged open like a book. Pointed reduction forceps (Weber clamps) are applied to the metaphyseal flare to compress the fragment back to the intact medial plateau.
2. Depression Fractures: A cortical window is created in the metaphysis distal to the fracture. A bone tamp is introduced through the window, and the depressed articular segment is carefully elevated under direct vision and fluoroscopic guidance.
3. Bone Grafting: Elevation of a depressed segment creates a metaphyseal void. This defect must be filled with autograft (e.g., iliac crest), allograft, or synthetic bone substitutes (e.g., calcium phosphate cement) to prevent secondary subsidence of the articular cartilage.

Provisional Fixation
Once the articular surface is anatomically reduced and supported by bone graft, provisional fixation is achieved using multiple Kirschner wires (K-wires). These wires are placed subchondrally, parallel to the joint line, ensuring they do not interfere with the planned trajectory of the definitive lag screws or the placement of the buttress plate.

Definitive Lag Screw and Plate Fixation
The definitive fixation sequence is critical to achieving absolute stability:
- Independent Lag Screws: If the fracture morphology permits, independent lag screws are placed perpendicular to the fracture plane. The standard sequence is utilized: 4.5mm gliding hole in the near cortex, insertion of the drill sleeve, 3.2mm thread hole in the far cortex, countersinking, measuring, tapping, and screw insertion.
- Plate Application: A pre-contoured anatomic locking plate or a standard buttress plate (e.g., L-buttress or T-plate) is applied to the lateral cortex. The plate must sit flush against the bone at the apex of the fracture.
- Diaphyseal Fixation First: To achieve the buttress effect, the plate is first secured to the intact distal diaphyseal segment using cortical screws. If the plate is slightly under-contoured, tightening these diaphyseal screws will drive the proximal portion of the plate into the metaphyseal flare, compressing the articular fragment.
- Periarticular Screws: Subchondral "rafting" screws are then inserted through the proximal holes of the plate. These screws support the elevated articular cartilage and neutralize any remaining forces. In modern osteosynthesis, locking screws are frequently utilized in the periarticular segment to create a fixed-angle construct, which is particularly beneficial in osteopenic bone.

Fluoroscopic Verification
Before closure, comprehensive fluoroscopic imaging is mandatory. True AP and lateral views, along with oblique projections, are obtained to confirm anatomic reduction of the joint line, verify restoration of mechanical alignment, and ensure that no hardware has penetrated the intra-articular space.
Complications and Management
Despite meticulous surgical technique, the management of partial articular fractures carries a significant risk of complications. Early recognition and aggressive management are paramount to preserving limb function.

Table of Common Complications and Salvage Strategies
| Complication | Incidence | Etiology/Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Deep Surgical Site Infection | 2% - 8% | Poor soft tissue envelope, early incision, diabetes, smoking | Aggressive serial debridement, hardware retention (if stable) vs removal (if loose), culture-directed IV antibiotics, soft tissue coverage (flaps). |
| Secondary Articular Subsidence | 5% - 15% | Inadequate bone grafting, premature weight-bearing, severe osteoporosis | Revision open reduction and internal fixation (ORIF) with structural grafting. In elderly patients with severe destruction, conversion to total joint arthroplasty may be indicated. |
| Post-Traumatic Osteoarthritis | 10% - 30% | Initial cartilage impaction damage, residual articular step-off > 2mm, malalignment | Conservative management initially (NSAIDs, injections). Definitive management via corrective osteotomy (if joint preserved) or arthrodesis/arthroplasty. |
| Joint Stiffness / Arthrofibrosis | 10% - 20% | Prolonged immobilization, excessive surgical trauma, prominent hardware | Aggressive physical therapy. If refractory, hardware removal and arthroscopic or open lysis of adhesions / manipulation under anesthesia (MUA). |
| Hardware Failure / Loss of Fixation | < 5% | Failure to achieve buttress effect, unrecognized diaphyseal extension, non-compliance | Revision ORIF with robust fixed-angle constructs, spanning plates, and augmentation with bone graft to address non-union or delayed union. |

Management of Intra-Articular Hardware Penetration
A critical intraoperative complication is the unrecognized penetration of screws into the joint space, leading to rapid chondral destruction. This must be avoided by utilizing multiple fluoroscopic views, including dynamic rotation of the C-arm. If suspected postoperatively, a CT scan is diagnostic. Immediate return to the operating room for hardware exchange or removal is required to prevent catastrophic joint damage.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to balance the conflicting needs of early joint mobilization for cartilage nutrition and the protection of the internal fixation construct from premature loading.

Phase I: Immediate Postoperative Period (Weeks 0 to 6)
- Weight-Bearing: Strict non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) is mandatory for lower extremity partial articular fractures. The buttress plate and lag screws provide absolute stability but cannot withstand the massive forces of full body weight prior to bone healing.
- Range of Motion (ROM): Early, active, and active-assisted ROM is initiated immediately. Continuous Passive Motion (CPM) machines may be utilized, though evidence suggests active motion is superior for preventing arthrofibrosis.
- Edema Control: Elevation, cryotherapy, and compressive dressings are utilized to manage soft tissue swelling and prevent wound complications.
Phase II: Intermediate Healing Phase (Weeks 6 to 12)
- Radiographic Assessment: Clinical follow-up with radiographs at 6 weeks to assess for maintenance of reduction and early signs of bone healing (blurring of fracture lines). Note that absolute stability constructs heal without visible callus.
- Weight-Bearing: Gradual progression of weight-bearing is initiated, typically advancing by 25% of body weight per week, guided by radiographic progression and patient tolerance.
- Strengthening: Introduction of isometric and progressive resistance exercises for the surrounding musculature to counteract disuse atrophy.
Phase III: Late Rehabilitation and Return to Function (Months 3 to 6+)
- Weight-Bearing: Progression to full, unrestricted weight-bearing.
- Functional Training: Proprioceptive training, gait normalization, and sport-specific or occupation-specific functional drills.
- Hardware Removal: Routine hardware removal is not recommended. It is considered only after 12-18 months if the patient experiences symptomatic hardware prominence (e.g., iliotibial band friction over a lateral tibial plate) and radiographs confirm complete union.
Summary of Key Literature and Guidelines
The surgical management of partial articular fractures is heavily guided by established literature and biomechanical studies.

Foundational AO Principles
The AO Foundation's principles of fracture management remain the gold standard. Müller et al. established that articular fractures require absolute stability to allow primary bone healing, which is achieved through anatomic reduction and interfragmentary compression. The concept of the buttress plate, specifically designed to counteract shear forces in Type B fractures, is a direct application of these biomechanical tenets.
Articular Congruity and Osteoarthritis
Key literature, including classic studies by Radin and modern finite element analyses, demonstrates that articular step-offs alter joint contact mechanics. A step-off of greater than 2mm is universally recognized as the threshold for an unacceptable reduction, as it leads to focal cartilage overloading and predictable degeneration. However, recent literature also emphasizes that the initial trauma to the chondrocytes at the time of impact (the "first hit") plays a significant role in post-traumatic osteoarthritis, regardless of the quality of the surgical reduction.
Evolution of Plating Technology
The transition from conventional plates to locking compression plates (LCP) has influenced the management of partial articular fractures, particularly in osteoporotic bone. While standard buttress plating relies on friction between the plate and bone, fixed-angle locking constructs provide enhanced pull-out strength in metaphyseal bone. However, literature cautions that locking screws cannot be used to lag fragments to the plate; therefore, standard lag screw techniques must still be employed prior to the application of locking screws to ensure articular compression.
In conclusion, the successful management of partial articular fractures via plate fixation requires a profound understanding of joint anatomy, rigorous adherence to biomechanical principles, and meticulous surgical execution to restore anatomy and optimize patient outcomes.
